

clavien_atlas_of_upper_gastrointestinal_and_hepato-pancreato-biliary_surgery2007-10-01_3540200045_springer
.pdfExtended Hemihepatectomies
Stefan Heinrich, Pierre-Alain Clavien
Extended Right Hemihepatectomy
(Right Trisectionectomy)
The extended right hemihepatectomy (also called right trisectionectomy) includes resection of segments 4–8. For cholangiocarcinoma of the liver hilum (Klatskin’s tumor) or carcinoma of the gallbladder, an en-bloc resection including segments 1 and 9 is usually performed. This procedure should only be performed if the remnant liver (segments 2 and 3) provides sufficient liver function. Therefore, preoperative assessment of liver function, a volumetric assessment of the expected remnant liver volume, and exclusion of liver fibrosis or cirrhosis are essential before extended resections.
Dependent on the vascular anatomy, two different approaches can be used for the anatomic resection of Sg4 in addition to segments 5–8. The classical anatomic resection of Sg4 is performed by selective ligation of the pedicle to Sg4 prior to tissue transsection. Alternatively, tissue transsection can be performed first with ligation of the pedicle to Sg4 during parenchymal transsection. Here, we describe the classical approach of resection.
STEPS 1–7 are the same as for a right hemihepatectomy.
364 |
SECTION 3 |
Liver |
|
|
|
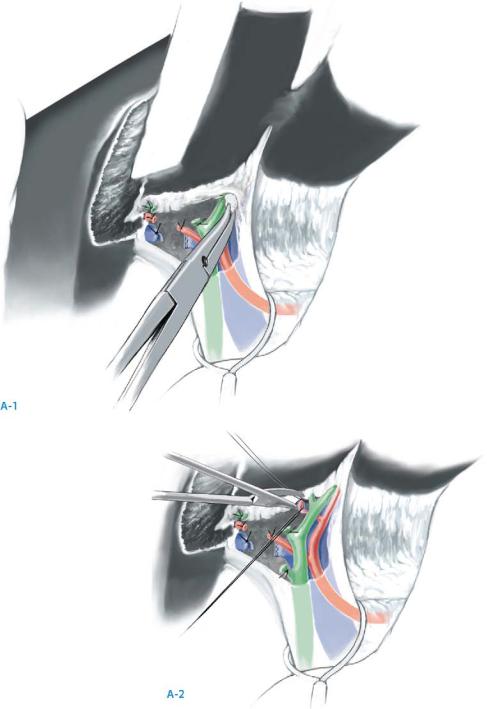
STEP 8 |
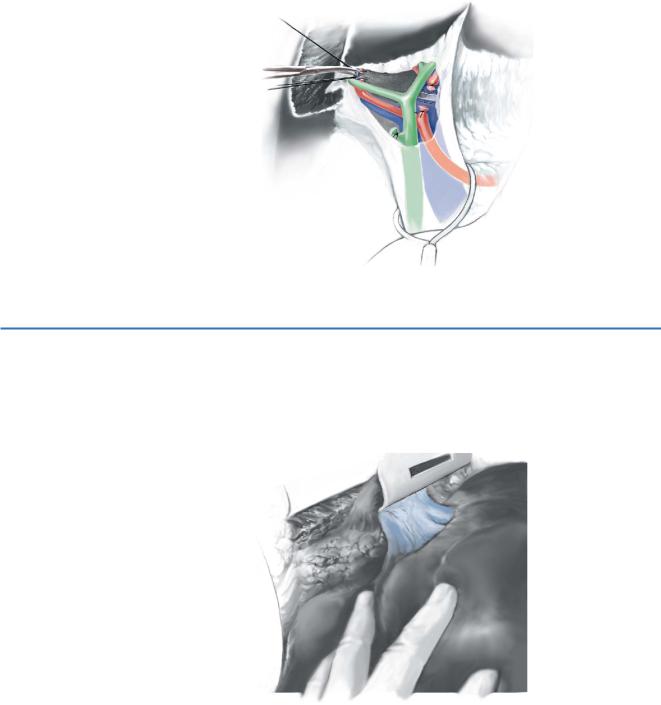
Selective ligation of the pedicle to segment 4 |
|
|
|
|
After mobilization of the right liver and ligation of the right branches of the hepatic artery and portal vein, careful blunt dissection along the left portal sheath is performed (A-1). The pedicle to segment 4 is then identified, carefully dissected and the vessels selectively ligated (A-2).
Extended Hemihepatectomies |
365 |
|
|
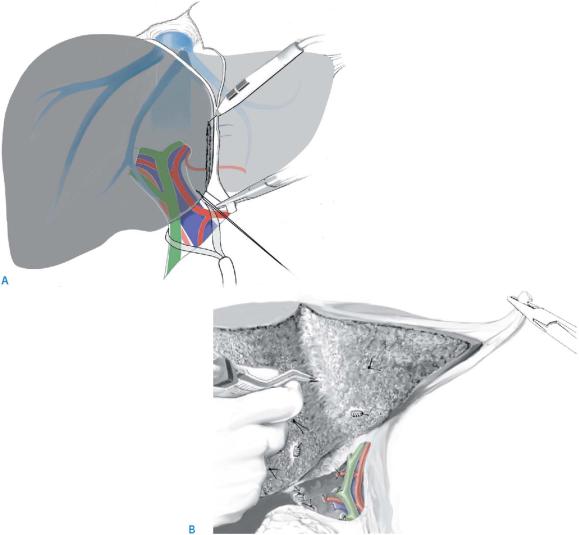
STEP 9 |
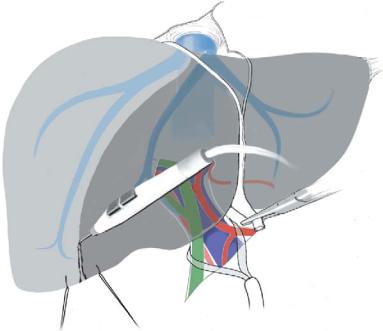
Exposure of the right hepatic vein and parenchymal transsection |
|
The right hepatic vein is isolated from below and marked with a rubber band as for a |
|
|
|
right hepatectomy. If the transection is going to be performed with a suspension tech- |
|
nique, the right and middle hepatic veins can be isolated from the top as described in |
|
the chapter “Hanging Maneuver for Right Hepatectomy.” |
|
The resection margin for the extended right hepatectomy is the right side of the falci- |
|
form ligament. Since the round ligament harbors the fetal connection of the umbilical |
|
cord with the left hepatic vein (Arantius’ duct), it can be used as a guide. It is fixed with |
|
a Kelly clamp and retracted to the left, while a stay suture is placed to the right (A). |
|
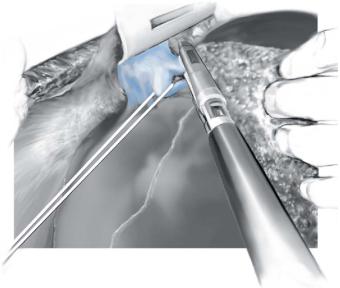
Intraoperative ultrasound is routinely performed to define the exact extent of the |
|
lesion and to identify vascular anatomy. |
|
Tissue transsection is started just to the right of the round ligament. All branches |
|
from the right side of the round ligament into the liver need to be ligated selectively (B). |
|
If not performed prior to the parenchymal transsection, the pedicle to segment 4 can |
|
now be selectively ligated (this approach can be advantageous in tumors involving the |
|
left portal sheath). The right bile duct and the bile duct to segment 4 can now be ligated |
|
safely. |

366 |
SECTION 3 |
Liver |
|
|
|
STEP 10 |
Ligation of the right and middle hepatic veins |
|
|
|
|
Approaching the hepatic veins, the middle hepatic vein is now isolated. As the right hepatic vein has been prepared before, both can be divided at the end of the parenchymal dissection by means of a vascular stapler.
Of note, the middle and left hepatic veins usually share a common trunk. Make sure that the left hepatic vein is preserved!
In addition to this extended right hemihepatectomy, the caudate lobe (segments 1, 9) can be approached and resected en bloc, if needed (see Section 4).
Extended Hemihepatectomies |
367 |
|
|
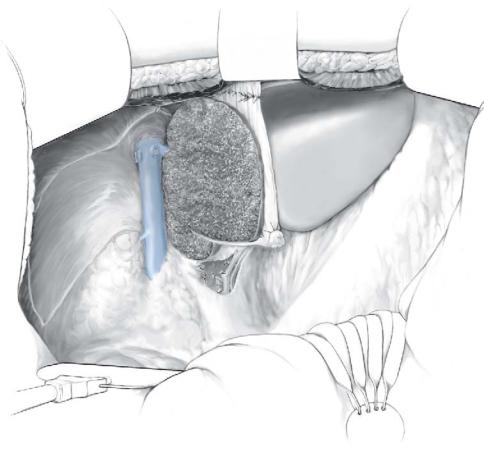
STEP 11 |
Reattachment of the falciform ligament |
|
The falciform ligament must be reattached to prevent rotation of the remnant liver, since |
|
|
|
this can result in an acute Budd-Chiari syndrome (obstruction of the venous outflow of |
|
the liver), which is a fatal complication after extended right liver resections . |
368 SECTION 3 Liver
Extended Left Hemihepatectomy
(Left Trisectionectomy)
The extended left hemihepatectomy includes resection of segments 2, 3, 4, 5 and 8. This procedure should only be performed if the remnant liver (segments 1/9+6+7)
provides sufficient liver function. Preoperative assessment of liver function, volumetric evaluation of the expected remnant liver volume and exclusion of liver fibrosis or even cirrhosis are essential.
Depending on the vascular anatomy, two different approaches can be used for the anatomic resection of segments 5 and 8 in addition to the left liver. The classical anatomic resection of segments 5 and 8 is performed by selective ligation of the pedicle to these segments prior to tissue transsection. Alternatively, tissue transsection can be performed with ligation of the pedicle to segments 5 and 8 during parenchymal transsection. Here, we describe the classical approach of resection.
STEPS 1–7 are the same as for a left hemihepatectomy.
To prepare an extended left hemihepatectomy, the right liver must be mobilized as for a formal right hemihepatectomy including the division of the short hepatic veins (see chapter “Right Hemihepatectomy”).
Extended Hemihepatectomies |
369 |
|
|
STEP 8 |
Selective ligation of the pedicle to segments 5 and 8 |
|
The pedicle to segments 5 and 8 (right anterior pedicle) is identified by careful blunt |
|
|
|
dissection on the right portal sheath. The vessels are selectively ligated, while the right |
|
posterior pedicle needs to be preserved. For tumors involving the right portal sheath, |
|
the anterior pedicle should not be dissected in the hilum, but ligated during tissue |
|
transsection. Intraoperative ultrasound is a helpful tool to define the exact extent of the |
|
lesion and to identify vascular anatomy. |
STEP 9 |
Exposure of the left and middle hepatic vein |
|
The middle and left hepatic veins, which usually share a common trunk, are isolated |
|
|
|
by careful dissection from above and marked with a rubber band for later dissection, |
|
while the right hepatic vein is identified and preserved. |
370 |
SECTION 3 |
Liver |
|
|
|
STEP 10 |
Parenchymal transsection |
|
|
|
|
The resection is performed along the demarcation line, which can be seen after ligation of the pedicles to segments 5 and 8. Stay sutures allowing gentle traction are placed on each side of the demarcation. If the pedicle cannot be ligated first, the plane of transsection is about 1cm to the left of the right hepatic vein as defined by intraoperative ultrasound.
Particular attention must be paid to the right hepatic vein and its course needs to be known during the whole period of tissue transsection. The left bile duct and the bile duct to segments 5 and 8 can be safely ligated at the end of parenchyma dissection.
Extended Hemihepatectomies |
371 |
|
|
STEP 11 |
Ligation and transsection of the left and middle hepatic veins |
|
At the end of tissue transsection, the left and middle hepatic veins are transsected by |
|
|
|
means of a vascular stapler and the resected part is removed, leaving segments 6 and 7 |
|
and the caudate lobe. In addition to this formal extended left hemihepatectomy, the |
|
caudate lobe can be approached and resected en bloc, if needed (see Section 4). |
372 |
SECTION 3 |
Liver |
|
|
|
|
Tricks of the Senior Surgeon |
|
■Extended hemihepatectomies are typically performed for large tumors partially invading segment 4 (extended right hemihepatectomy) or segments 5/8 (extended left hemihepatectomy) or hilar cholangiocarcinoma. In these cases, we do not selectively ligate the pedicles to segments 4 or 5 and 8, respectively, but rather perform a formal hemihepatectomy and extend the resection margin into the contralateral liver (extended wedge resection). This approach may spare liver parenchyma and operative time.
■In the case of tumor involvement of the hilum, dissection and selective ligation of segmental pedicles should be performed during tissue transsection.
■Similarly, in some situations preparation and transsection of the hepatic veins may prove difficult. Two strategies should be considered:
–Transsection of the hepatic veins during parenchymal transsection without previous isolation.
–Total vascular exclusion (TVE).
■Portal vein embolization with delayed hepatectomy (about 4weeks) should be considered prior to resection, if the remnant liver is judged too small.