

clavien_atlas_of_upper_gastrointestinal_and_hepato-pancreato-biliary_surgery2007-10-01_3540200045_springer
.pdfSECTION 3
Liver
Pierre-Alian Clavien

Introduction
Pierre-Alain Clavien
Liver surgery was considered until the early 1980s as a “heroic” field of medicine associated with much blood loss, and high patient morbidity and mortality. With such a reputation only life-threatening conditions were usually referred for liver surgery. As surgeons acquired a better understanding of surgical anatomy and physiology, a better understanding of periand intraoperative management, and importantly formal training periods in this field, hepatic surgery began to enjoy rapid expansion and high credibility among colleagues and patients. Today, liver surgery is one of the most complex and successful areas of medicine with the availability of a variety of highly sophisticated procedures for many indications including complex liver resection or transplantation of only one part of the liver from a living donor.
The first chapter presents a comprehensive approach to the terminology of liver anatomy and resection (Brisbane 2000 terminology), according to an international effort including leaders from all continents. The next three chapters present available techniques for vascular exclusion, parenchyma dissection and the “hanging” maneuver, which may enable better exposure for anatomic resections. The hepatic surgeon must be familiar with all these techniques, which may be of great help in many difficult situations. Then, the focus turns to formal anatomic and non-anatomic liver resections, including laparoscopic approaches, which are gaining increasing popularity. As liver resection is often not possible due to local difficult situations (poor liver reserve or location of a tumor) or poor general condition of the patient, alternative techniques
are presented including cryosurgery, radiofrequency ablation and selective intra-arterial chemotherapy. Benign and infectious cysts require particular strategies, which are well covered in two separate chapters. A chapter also comprehensively covers the available strategies for liver trauma in the modern area of “damage control injury.” The last
six chapters cover various aspects of liver transplantation from organ procurement, to partial living or cadaveric orthotopic liver transplantation, as well as auxiliary liver transplantation.
While there is no substitute for experience in performing complex surgical procedures, we hope that this section, prepared by worldwide experts, will clarify standards and limitations for surgeons in performing hepatic surgery.

Terminology of Liver Anatomy and Resections:
The Brisbane 2000 Terminology
Steven M. Strasberg
In 1998 at its meeting in Berne, Switzerland, the Scientific Committee of the International Hepato-Pancreato-Biliary Association (IHPBA) established a Terminology Committee to deal with the confusion in terminology of hepatic anatomy and liver resections (see below: members of the committee). The recommendations of the Terminology Committee were presented to the Scientific Committee at the biannual meeting of the IHPBA in Brisbane, Australia, in 2000. These recommendations, consisting of a new terminology termed The Brisbane 2000 Terminology of Liver Anatomy and Resections, were unanimously accepted by the Scientific Committee of the IHPBA and were presented to the membership as the official terminology of the IHPBA. The terminology was published in the official journal of the IHPBA in 2000.
The terminology shown below is based on the hepatic artery and bile duct (Figures 1–3). A terminology based on the division of the portal vein was added as an addendum.
The terminology is presented as a set of four figures. The liver is divided in the tables into successive orders. The following notes serve as a guide to the tables.
Note 1
Couinaud segments are indicated in short form as Sg1–9 (e.g., Sg6).
Comment: Sg is chosen rather than S to avoid confusion of segment with section or sector. Arabic numerals are chosen rather than Roman numerals because many nonWestern nations do not use Roman numerals.
Note 2
Anatomical and surgical terms are underlined. Explanatory terms and notes within the figures are in italics.
Note 3
Wherever the word “OR” (uppercase, bold) appears in the table it indicates equally acceptable terminology; e.g.,“right hemiliver” OR “right liver.” The choice is that of the user. Wherever the word “or” (lowercase, bold) appears in the table or these notes it indicates that the first choice is preferred but that the second is acceptable; e.g.,“right trisectionectomy” or “extended right hepatectomy.” The choice is up to the user but the first term is the preferred term. The reason in this case is as follows. As some use the adjective “extended” to indicate any degree of extension of a resection over the midplane, which in some cases is less than a whole section, the terms in the table containing the word “extended,” while acceptable, are less preferred.
314 SECTION 3 Liver
Note 4
When segment 1 is resected as part of a procedure, it should be stated as in the following example: “left hemihepatectomy with resection of segment 1” or “left hemihepatectomy extended to segment 1.”
Note 5
It is always correct to refer to any resection by its segments. For instance,“right hepatectomy” and “resection Sgs 5–8” are equally acceptable.“Left lateral sectionectomy” and “resection Sgs 2, 3” are equally acceptable.
Reference
Terminology Committee of the International Hepato-Pancreato-Biliary Association: SM Strasberg (USA), J Belghiti (France), P-A Clavien (Switzerland), E Gadzijev (Slovenia), JO Garden (UK), W-Y Lau (China), M Makuuchi (Japan), and RW Strong (Australia).
The Brisbane 2000 Terminology of Liver Anatomy and Resections. HPB 2:333–339, 2000
Anatomical |
Couinaud segments |
Term for |
Diagram |
Term |
referred to |
surgical resection |
(pertinent area is shaded) |
Right Hemiliver |
Sg 5–8(+/Sg1) |
Right Hepatectomy |
|
OR |
|
OR |
|
Right Liver |
|
Right Hemihepatectomy |
|
|
|
(stipulate +/-segment 1) |
|
Left Hemiliver |
Sg 2–4 (+/-Sg1) |
Left Hepatectomy |
OR |
|
OR |
Left Liver |
|
Left Hemihepatectomy |
|
|
(stipulate +/-segment 1) |
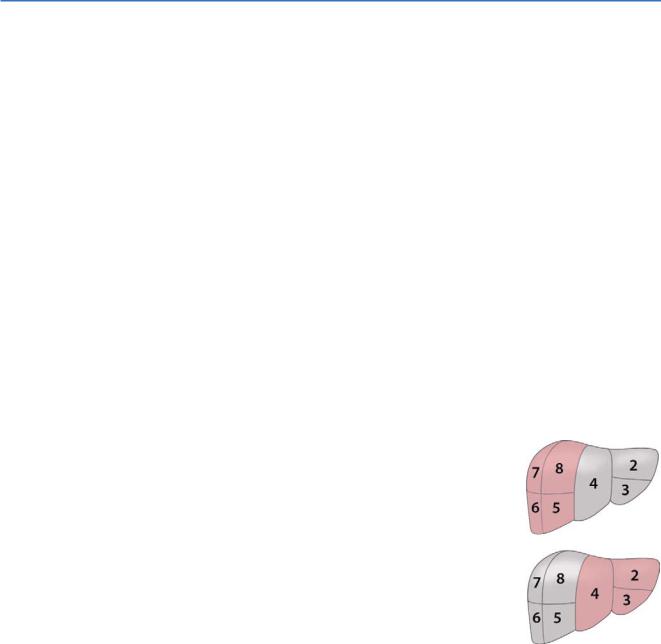
Border or watershed: The border or watershed of the first order division which separates the two hemilivers is a plane which intersects the gallbladder fossa and the fossa for the IVC and is called the “midplane of the liver”.
Fig 1. Nomenclature for first order division anatomy and resections

Terminology of Liver Anatomy and Resections:The Brisbane 2000 Terminology |
|
315 |
|
|
|
|
|
Anatomical |
Couinaud segments |
Term for |
Diagram |
Term |
referred to |
surgical resection |
(pertinent area is shaded) |
Right |
Sg 5,8 |
Add (-ectomy) to any of |
|
Anterior Section |
|
the anatomical terms an in |
|
|
|
Right anterior sectionectomy |
|
Right |
Sg 6,7 |
Right |
|
Posterior Section |
|
posterior sectionectomy |
|
Left |
Sg 4 |
Left medial sectionectomy |
|
Medial Section |
|
OR |
|
|
|
Resection segment 4 |
|
|
|
(also see Third order) |
|
|
|
OR |
|
|
|
Segmentectomy 4 |
|
|
|
(also see Third order) |
|
Left |
Sg 2,3 |
Left lateral sectionectomy |
|
Lateral Section |
|
OR |
|
|
|
Bisegmentectomy 2,3 |
|
|
|
(also see Third order) |
|
|
Other “sectional liver resections |
|
|
|
Sg 4–8 |
Right Trisectionectomy |
|
|
(+/-Sg1) |
(preferred term) |
|
|
|
or |
|
|
|
Extended Right Hepatectomy |
|
|
|
or |
|
|
Extended Right Hemihepatectomy |
|
|
|
|
(stipulate +/-segment 1) |
|
|
Sg 2, 3, 4, 5, 8 |
Left Trisectionectomy |
|
|
(+/-Sg1) |
(preferred term) |
|
|
|
or |
|
Extended Left Hepatectomy
or
Extended Left Hemihepatectomy
(stipulate +/-segment 1)
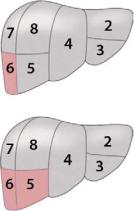
Border or watershed: The borders or watersheds of the sections are planes referred to as the right and left intersectional planes. The left intersectional plane passes through the umbilical fissure and the attachment of the falciform ligament. There is no surface marking of the right intersectional plane.
Fig 2. Nomenclature for second order division anatomy and resections, based on bile ducts and hepatic artery
316 |
SECTION 3 |
|
|
Liver |
|
|
|
|
|
|
Anatomical |
Couinaud segments |
Term for |
Diagram |
|
Term |
referred to |
surgical resection |
(pertinent area is shaded) |
|
Segments 1-9 |
Any one of |
Segmentectomy |
|
|
|
Sg 1 to 9 |
(e.g. segmentectomy 6) |
|
2 contiguous |
Any two of Sg 1 to Sg 9 |
Bisegmentectomy |
sements |
in continuity |
(e.g. bisegmentectomy 5,6) |
For clarity Sg.1 and 9 are not shown. It is also acceptable to refer to ANY resection by its third-order segments, eg. right hemihepatectomy can also be called resection Sg 5–8.
Border or watershed: The borders or watersheds of the segments are planes referred to as intersegmental planes.
Fig 3. Nomenclature for third order division anatomy and resections
Terminology of Liver Anatomy and Resections:The Brisbane 2000 Terminology |
|
317 |
|
|
|
|
|
Anatomical |
Couinaud segments |
Term for |
Diagram |
Term |
referred to |
surgical resection |
(pertinent area is shaded) |
Right |
|
Anterior Sector |
|
OR |
Sg 5,8 |
Right |
|
paramedian Sector |
|
Right |
|
Posterior Sector |
|
OR |
Sg 6,7 |
Right lateral Sector |
|
Left |
Sg 3,4 |
Medial Sector |
|
OR |
|
Left |
|
Paramedian Sector |
|
Left |
Sg 2 |
Lateral Sector |
|
OR |
|
Left |
|
Posterior Sector |
|
Add (-ectomy) to any of the anatomical terms as in
Right anterior sectorectomy
OR
Right paramedian sectorectomy
Right posterior sectorectomy
OR
Right lateral sectorectomy
Left medial sectorectomy
OR
Left paramedian sectorectomy
OR
Bisegmentectomy 3,4
Left lateral sectorectomy
OR
Left posterior sectorectomy
OR
Segmentectomy 2
Right anterior sector and Right anterior section are synonyms. Right posterior sector and Right posterior section are synonyms. Left medial sector and Left medial section are NOT synonyms and are NOT exchangeable terms. They do not describe the same anatomic areas. Left lateral sector and Left lateral section are also NOT synonyms and are NOT exchangeable terms.
Border or watershed: The borders or watersheds of second-order division based on PV are called right and left intersectoral planes. These have no surface markings.
Fig 4. (Addendum) Nomenclature for alternative second order division, based on portal vein

Techniques of Liver Parenchyma Dissection
Mickaël Lesurtel, Pierre-Alain Clavien
Parenchyma dissection of the liver may cause complications including blood loss, hematoma, infection, bile leakage and liver failure. Various surgical techniques have been developed for careful and safe dissection of the liver parenchyma to prevent intraoperative and postoperative complications.
The aim of this chapter is to give an overview of the techniques and devices frequently used to perform parenchyma dissection of the liver, including:
■Kelly clamp and bipolar forceps
■Water jet dissection
■Ultrasonic dissection
■Ultrasound cutting
■Dissecting sealer
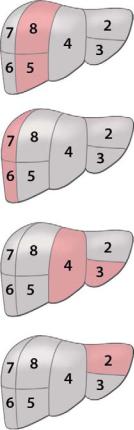
Preparation of Parenchyma Dissection
The liver capsule is incised with diathermy on the resection line. For a better exposure, two stay sutures (2-0 silk) can be placed at the inferior margin of the liver, one on each side of the resection line. These stay sutures are used to lift up the liver and the resection line. Care should be taken not to pull and tear the liver parenchyma, leading to bleeding. To prevent unnecessary liver ischemia, the Pringle maneuver for continuous or intermittent inflow occlusion is applied individually depending on the intraoperative surgical
situation. Indeed, except for the Kelly clamp, the other techniques were developed to avoid use of the Pringle maneuver and to minimize risk of liver ischemia.
320 SECTION 3 Liver
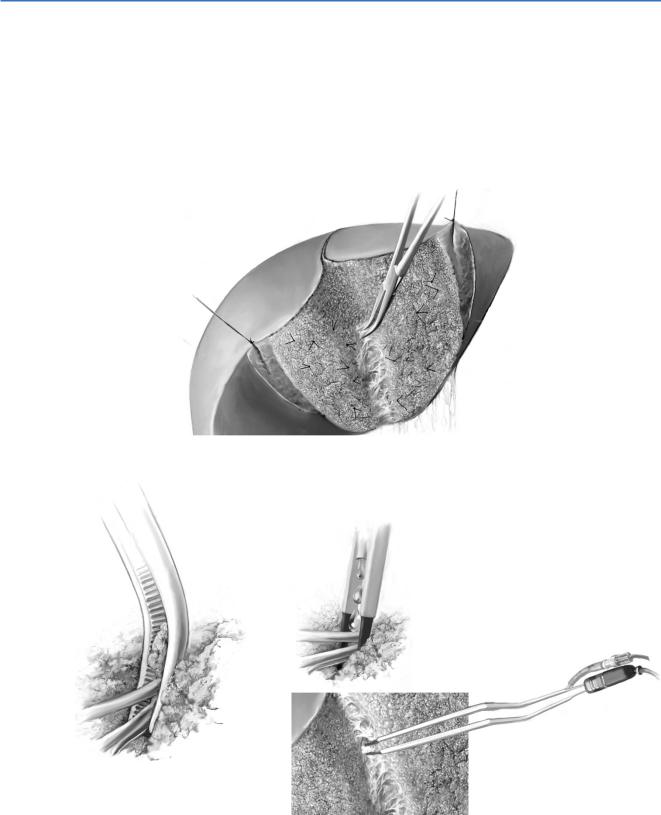
Kelly Clamp and Bipolar Forceps
A small clamp (Kelly) is used to crush parenchyma between its blades in order to isolate vessels and bile ducts (A-1, A-2). Fine branches of Glisson’s tree or tiny tributaries of hepatic veins (<3mm) are coagulated using a bipolar forceps and are cut by scissors (A-3). Bipolar forceps cautery is equipped with a channel for water dripping, which prevents adhesion of debris to the cautery blades. Bigger identified vessels or bile ducts (>3mm) are ligated or clipped on the remnant liver slice before cutting. The alternative is to use clips only to secure vessels and bile ducts.
A-1
A-2
A-3

Techniques of Liver Parenchyma Dissection |
321 |
|
|
Water Jet Dissection (Helix Hydro-Jet, Erbe)
With this device the liver parenchyma is dissected by a jet of water (A-1). Saline is pressurized by high pressure pump and is conducted by a high pressure hose to the nozzle. Here the pressure is converted into kinetic energy. For liver parenchyma, pressures of 30–50bar should be used. The soft liver tissue is washed off the more resistant vessels and bile ducts (A-2). The applicator should be used in direct contact with the tissue and moved like a paintbrush. It can be used in combination with suction and with an electrosurgical unit. Vessels and bile ducts are isolated and can be secured using bipolar forceps, clips or ligatures as with the Kelly clamp. They can then be transected under controlled conditions.
A-1
A-2