CHRONIC DISSEMINATED TUBERCULOSIS.
Usually develops slowly as a result of repeated waves of lymphohematogenous dissemination, which are not diagnosed in time. Repeated waves of dissemination cause "staged" location of foci in both lungs, first in the apical and posterior segments. The greatest number of foci are found in the upper and middle parts of the lungs, they are localized mainly subpleural. In the lungs there is a thin looping network of whitish-gray fibrous bands associated with diffuse perivascular and peribronchial fibrosis, which are most pronounced in the upper lungs, and vicarious emphysema develops in the lower lungs. Sometimes massive scarring in the lung tissue and pleural fibrosis can be found.

The foci have significant morphological differences (polymorphic dissemination): fresh ones are dominated by a pronounced productive tissue reaction, old ones are surrounded by a capsule, partially replaced by fibrous tissue, with inclusions of calcium salts. The tendency to foci fusion and decay formation is weakly expressed, so decay cavities form slowly, cavities (stamped, or spectral, caverns) are located in the upper lobes of both lungs, partially symmetrically, their lumen is completely free from caseous-necrotic masses; walls are thin, perifocal infiltration and edema of surrounding tissues is absent.

Clinical picture of chronic disseminated pulmonary tuberculosis:
1.In exacerbation: symptoms of intoxication, dry cough, sometimes with a small amount of sputum, shortness of breath, functional changes in the central and autonomic nervous system, endocrine disorders (hyper- or hypothyroidism).
2.Percussion sound shortening over the upper parts of the chest, the appearance of dry rales or numerous wet rales, over the lower parts of the chest - tympanic percussion.
3.Caverns are often "mute", i.e. they are not detected by percussion and auscultation.
4.Without treatment, chronic disseminated pulmonary tuberculosis progresses and transforms into fibrous cavernous pulmonary tuberculosis.
5.sound, attenuated vesicular breathing.

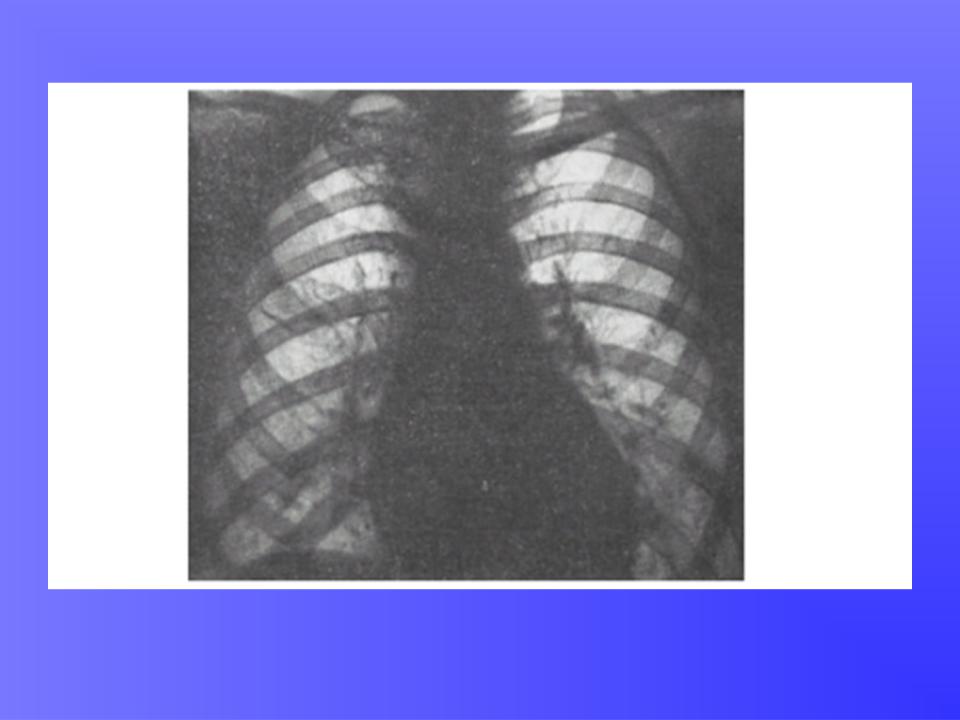
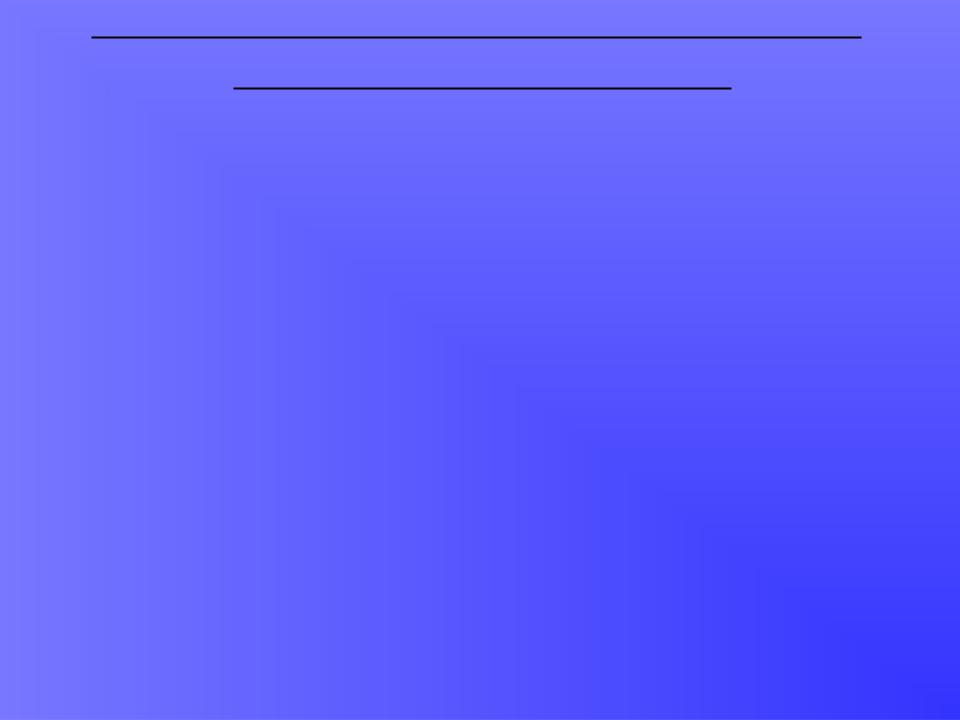
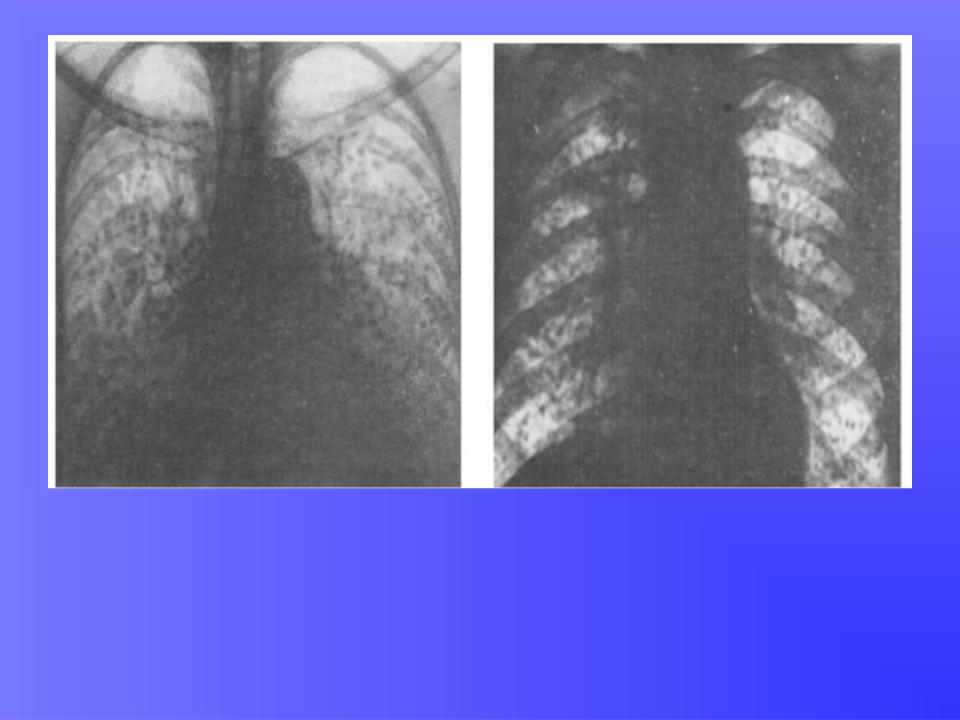
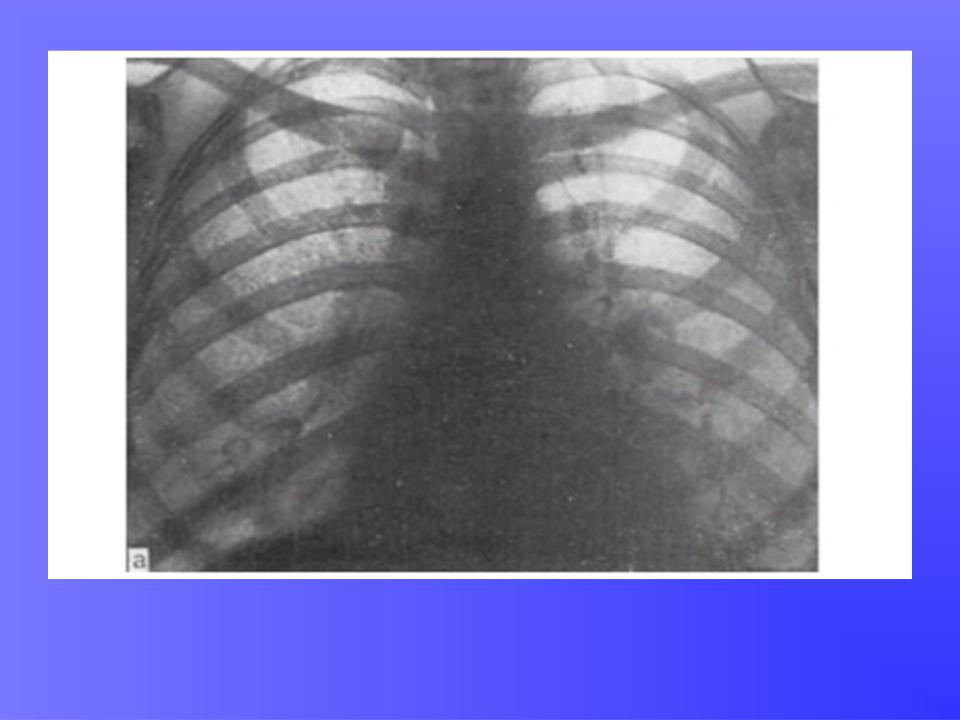
X-ray characteristics of chronic disseminated pulmonary tuberculosis:
This process corresponds to chronic hematogenous dissemination syndrome:
1.Presence of different-type (polymorphic) foci in size, shape, intensity; conglomerates of foci (type of tuberculoma) are possible.
2.Process localization is bilateral, in upper and middle parts of lungs.
3.Location of shadows is asymmetrical.
4.Upward displacement of lung roots, their deformation and fibrosis.
5.Retinal deformity of the lung pattern.
6.Emphysema, pleural changes.
Differential diagnosis of disseminated
pulmonary tuberculosis:
1. Tuberculosis.
2. Sarcoidosis.
3. Pneumoconiosis.
4. Histiocytosis X.
5. Pneumomycoses.
6. Fibrosing alveolitis (different variants of interstitial pulmonary fibrosis).
7. Metastatic lung lesions.
8. Bronchioloalveolar cancer.
9. Non-specific inflammatory processes.
10.Pulmonary edema (consequence of cardiac or renal failure).
11.Diffuse diseases of lung tissue.
12.Systemic vasculitis.
13.Accumulation diseases (primarily alveolar proteinosis).

Overview X-ray of massive bilateral enlargement of bronchopulmonal lymph nodes, strengthening of the pulmonary pattern, dissemination in the middle lower lungs. Biopsy of the lung and lymph nodes. Sarcoidosis
Overview X-ray. A characteristic picture of carcinomatosis with a predominant lesion of the middle and lower lungs.
Overview X-ray. Lung carcinomatosis with a uniform lesion of all departments. Central cancer of the upper lobular bronchus on the right. Bronchobiopsy
Overview radiograph of the lungs. Silicotuberculosis: intensive nodular formations in the cortical parts of both lungs, marginal calciner of intrathoracic lymph nodes
Оverview X-ray: Microlithiasis