

62M.R. Zaontz
››Not all cases of hypospadias require surgical correction particularly those contained well within the glans in the absence of penile curvature.
››Boys with associated penile curvature, misdirected downward urinary stream and or abnormal positioning of the scrotum with respect to the penis require surgical correction.
››Timing for surgery is usually performed around
6 months of age as a single stage outpatient procedure in the majority of cases although, more severe cases may need to be completed in two stages.
››The most common complications of surgery include urethrocutaneous fistula, urethral/meatal stenosis and recurrent penile curvature, all of which are correctable surgically.
7.1 Hypospadias
7.1.1 Introduction
Hypospadias (Fig. 7.1) is one of the more common conditions treated by pediatric urologists. Its incidence is around 8–16/1,000 live births.1 The penis is fully developed within the first 12–16 weeks of embryonic life so there is no associated increased risk of having hypospadias in premature neonates. This entity is usually referred after recognizing the defect at birth. The examiner will note in 95% of the cases that boys with hypospadias will have an incomplete hooded foreskin that is mostly dorsally located and that the opening of the penis is somewhere beneath the normal orthotopic location at the tip of the glans. The opening can be anywhere from 1 mm below the glanular tip to the level of the perineum in the most severe cases. The majority of hypospadias defects are distal in about 70% of the cases.

Chapter 7. Disorders of Male External Genitalia |
63 |
FIGURE 7.1. Example of classic distal hypospadias.
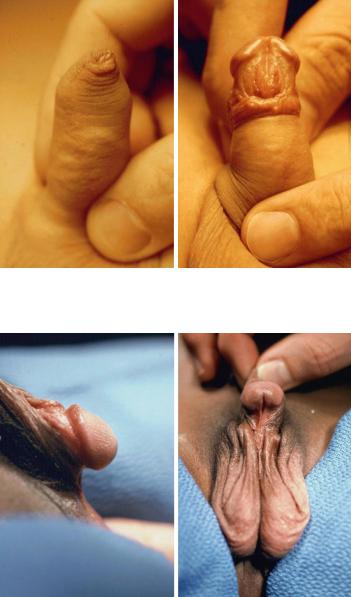
Practitioners need to beware of the boys born with a normal prepuce and have hidden beneath the foreskin hypospadias (Fig. 7.2a and b).This is noted in about 5% of hypospadias boys. Thus, it is imperative that all boys undergoing circumcision have their foreskins fully retracted before cutting, to determine where the urethral meatus is located, and if abnormal avoid circumcision.4
Penile curvature (Fig. 7.3), which commonly accompanies hypospadias, may or may not be appreciated at birth. Without seeing an erection, this is a difficult assessment especially in the boys with mild hypospadias. Curvature and/or ventral tethering of the penis is often more obvious visually in the boy with more proximal meatal locations.
On occasion the examiner may note an incomplete foreskin that has an orthotopic meatus. This boy has the hypospadias complex without hypospadias and, may or may not have penile curvature. Circumcision should be avoided in these boys.
64 M.R. Zaontz
a |
b |
FIGURE 7.2. (a) Complete prepuce. (b) Same boy showing distal megameatus hypospadias after retracting foreskin.
a |
b |
FIGURE 7.3. (a, b) Proximal hypospadias with ventral chordee.
Chapter 7. Disorders of Male External Genitalia |
65 |
Associated anomalies found in about 10–15% of boys with hypospadias include undescended testes, hernia and hydrocele. In boys that have associated undescended testes or nonpalpable testes, it is imperative to obtain a serum karyotype, as intersex conditions are common. Ultrasound screening of the kidneys are not routinely recommended for the majority of boys with hypospadias. However should he have a penoscrotal or more proximal meatus or associated midline anomalies, then it is reasonable to perform the ultrasound exam to rule out potential renal anomalies.
Circumcision should be avoided in all of the aforementioned scenarios so that the pediatric urologist can operate on a virginal, nonscarred penis and also has the ability to use the foreskin as needed for reconstructive purposes.
Fertility in boys with hypospadias, to our knowledge is not different from that of boys without hypospadias.
7.1.2 Management Issues
Assuming that the boy with hypospadias was born at term and had no significant respiratory or hematological issues, surgical timing for repair of hypospadias is recommended for around age 6 months as an outpatient procedure. In cases of severe prematurity, a history of respiratory problems, especially a history of apnea, surgery is generally held off until the infant is one year of age.
In the majority of cases, hypospadias repair is done as a single stage procedure. However, in cases of proximal hypospadias with severe chordee with or without penoscrotal transposition, a two-stage approach may be used. Depending on the appearance of the penis preoperatively and in particular the size of the glans, preoperative depotestosterone may be given intramuscularly in the thigh or given as a cream directly to the penis to enhance growth and help facilitate surgery. This is generally taken care of by the pediatric urologist’s office but certainly the primary care physician can arrange to give the shots in their office if desired.