


146 Chapter 16
16.5 Suggested further reading
Blair, F.M. & Wassell R.W. (1996) A survey of the methods of disinfection of dental impressions used in dental hospitals in the United Kingdom. Br. Dent. J. 180, 369.
Donovan, T.E. & Chee, W.W. (2004) A review of contemporary impression materials and techniques. Dent. Clin. North Am. 48, 445.
Wassell, R.W., Barker, D. & Walls, A.W.G. (2002) Impression materials and technique. In A Clinical Guide to Crowns and other Extra-coronal Restorations (R.W. Wassell, A.W.G. Walls, J.G. Steele & F.S. Nohl, eds), pp. 9–17. BDJ Books: London.

Chapter 17
Non-elastic Impression Materials
17.1 Introduction
Four main types of products form the group of impression materials classified as non-elastic materials:
(1)Impression plaster;
(2)Impression compound;
(3)Impression waxes;
(4)Zinc oxide/eugenol impression pastes.
They are classified together for convenience rather than for reasons of similarity in composition or properties. A factor which links the materials is their inability to accurately record undercuts. One of the materials (plaster) is brittle when set and fractures when withdrawn over undercuts. The other products are likely to undergo gross distortions due to plastic flow if used in undercut situations.
17.2 Impression plaster
Impression plaster is similar in composition to the dental plaster used to construct models and dies (Chapter 3). It consists of calcined, β-calcium sulphate hemihydrate which when mixed with water reacts to form calcium sulphate dihydrate.
The material is used at a higher water/powder ratio (approximately 0.60) than is normally used for modelling plasters. The fluid mix is required to enable fine detail to be recorded in the impression and to give the material mucostatic properties. The setting expansion of dental plaster is reduced to minimal proportions by using antiexpansion agents. Potassium sulphate is the most common of these and has the secondary effect of accelerating the setting reaction, details of which are discussed on p. 37. A retarder, such as borax, is normally incorporated, in order to give a mate-
rial in which the setting characteristics are controlled. A pigment such as alazarin red is also commonly used, in order to make a clear distinction between the impression and the model after casting of the model. The anti-expansion agent, retarder and pigment are incorporated into the impression plaster powder by some manufacturers. As an alternative an anti-expansion solution, containing potassium sulphate, borax and pigment, may be prepared and used with a standard white plaster.
Freshly mixed plaster is too fluid to be used in a stock impression tray and is normally used in a special tray, constructed using a 1–1.5 mm spacer. The tray may be constructed from acrylic resin or shellac. Another technique is to record the plaster impression as a wash in a preliminary compound impression. The compound is deliberately moved during setting to create space for the plaster wash. The technique for insertion of the impression into the mouth involves ‘puddling’ the impression into place. With other materials the tray is simply seated home in a single movement. With plaster the tray is gently moved from side to side and antero-posteriorly to best take advantage of the handling characteristics of the material, particularly its fluidity.
Before casting a plaster model in a plaster impression, the impression must be coated with a separating agent, otherwise separation is impossible.
The mixed impression material is initially very fluid and is capable of recording soft tissues in the uncompressed state. In addition, the hemihydrate particles are capable of absorbing moisture from the surface of the oral soft tissues, allowing very intimate contact between the impression material and the tissues. The fluidity of the material, combined with the ability to remove moisture from
147
148 Chapter 17
tissues and a minimal dimensional change on setting, results in a very accurate impression which may be difficult to remove.
The water-absorbing nature of these materials often causes patients to complain about a very dry sensation after having impressions recorded. Disinfection of a plaster impression can be achieved with a 10 minute soak in sodium hypochlorite solution as described previously.
Following setting, the plaster impression material is very brittle. It can undergo virtually no compressive or tensile strain without fracturing. The material is, therefore, not suitable for use in any undercut situations.
One technique for recording impressions of undercut areas, commonly used before the advent of elastic materials, was to allow the impression plaster to ‘set’ and then to fracture it in order to facilitate removal from the mouth. The material is weak and easily fractured due to its high water/ powder ratio. The fragments are then reconstructed in order to form the completed impression.
The properties of impression plasters can be compared with those of model plasters and stones by reference to Table 3.2. The main differences between impression plaster and model plaster are: more rapid setting in order to avoid inconvenience/discomfort to both the patient and dentist; smaller setting expansion for greater accuracy – the expansion is actually equivalent to that observed for a low expansion die stone (type 4) and much lower strength so that fracture can occur easily if the material engages an undercut.
Dental impression plaster remains a useful material, particularly when recording impressions of patients with excessively mobile soft tissues overlying the residual alveolar bone (a ‘flabby’ ridge). It is important to capture such tissue at rest rather than risk an abnormal pattern of displacement with a more viscous impression material. A two-stage technique is commonly used in which a special tray is made with appropriate spacing for zinc oxide/eugenol paste where the mucosa is well supported and having a window overlying the ‘flabby’ area. An impression of the bulk of the ridge is recorded in zinc oxide/eugenol paste. Any excess material is removed from the window and the impression re-seated in the mouth. The shape of the flabby ridge at rest is then recorded by painting plaster into its surface with a brush and keying this impression into the impression tray.
17.3 Impression compound
Impression compound (see Fig. 17.1) is a thermoplastic material, having properties which in many ways are similar to those of the dental waxes discussed in Chapter 4. The composition varies from one product to another but an indication of typical composition is given in Table 17.1. Two types of impression compound are available. These are usually classified as type I (lower fusing) and type II (higher fusing). The type I materials are impression materials whereas the type II materials are used for constructing impression trays. The difference in fusing temperature between type I and type II materials naturally reflects a difference in the composition of the thermoplastic components of each.
The lower fusing, type I impression materials may be supplied in either sheet or stick form. The sheet material is used for recording impressions of edentulous ridges, normally using stock trays. The stick material is used for border extensions on impression trays or for recording impressions of single crowns using the copper ring technique.
The sheet material is normally softened using a water bath. Both the temperature and time of conditioning in the water bath affect the performance of the material. If the conditioning temperature is too low the material does not soften properly, and if too high, it becomes sticky and unmanageable. A temperature in the range 55– 60ºC is normally found to be ideal.
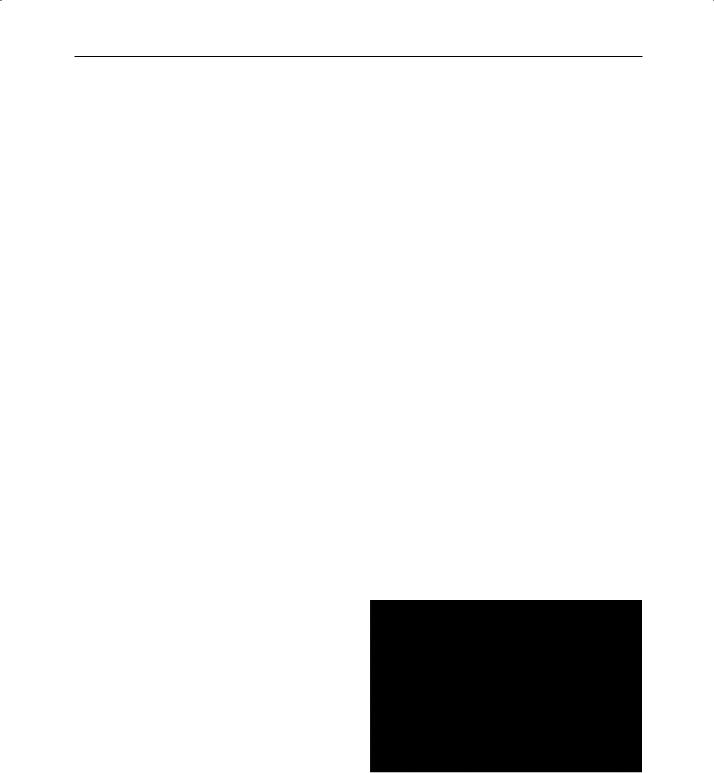
Fig. 17.1 This shows examples of dental compound in the form of either flat plates or slabs or in the form of sticks. The slabs are used to make impressions of edentulous areas in the mouth whilst the sticks are used as tray extension materials or for extending special (individual) trays.
|
|
Non-elastic Impression Materials |
149 |
|
|
|
|
Table 17.1 Composition of a typical impression compound material. |
|
|
|
|
|
|
|
Component |
Example |
Function |
|
|
|
|
|
Thermoplastic material (47%) |
Natural or synthetic resins |
Characterises the softening temperature |
|
|
and waxes |
|
|
Filler (50%) |
Talc |
Gives ‘body’ by increasing viscosity of the softened |
|
|
|
material; reduces thermal contraction |
|
Lubricant (3%) |
Stearic acid |
Improves flow properties |
|
|
|
|
|
The conditioning time must also be carefully monitored. It should not be so long that important constituents, such as stearic acid, can be leached out, nor should it be so short that the material is not thoroughly softened. The materials are poor conductors of heat and it may take several minutes for the centre of the material to become softened. It is considered, that for optimal results, type I impression compound should undergo considerable flow at temperatures above 45ºC but flow should be minimal at or below 37ºC. The stick material is generally softened using a flame. A measure of skill and experience is required in order to soften the material sufficiently without causing it to become too fluid or to ignite. The material is tempered in a water bath before placing in the patient’s mouth.
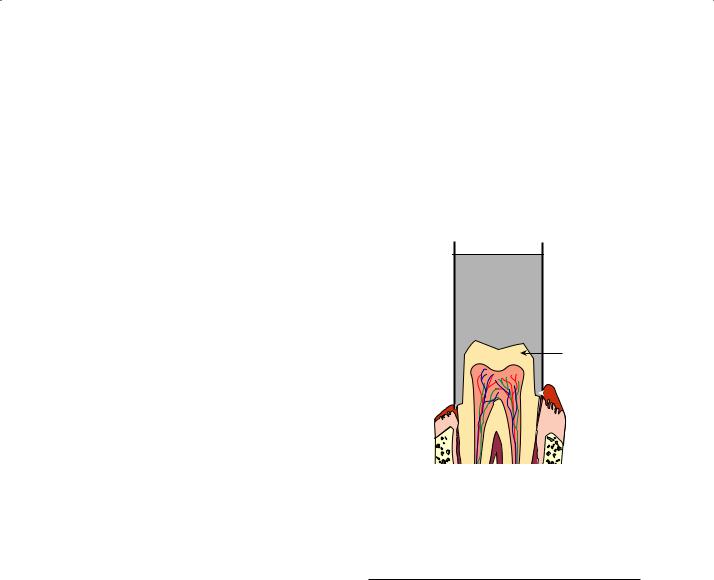
The copper ring technique involves the recording of single crown preparations in stick compound employing a hollow, open-ended copper tube as a type of ‘tray’. The principle is illustrated in Fig. 17.2. The surface of the compound is copper plated in an electroplating bath and an epoxy resin/metal die made. A separate locating impression is also recorded of the prepared tooth. The die is inserted into this impression and then a stone working model is made by pouring stone into the impression. This technique has largely been superseded by the use of silicone rubbers for crown and bridgework. However, it can be of value, particularly in areas where moisture control is a problem.
One of the main requirements for impression compound, set out in American and British Standards, is for the value of flow at mouth temperature (37ºC) and 45ºC (Table 17.2). It is this test which primarily distinguishes the type I and type II materials. The type I material should flow readily at just above mouth temperature, whilst the type II material should ideally not distort at mouth temperature. The flow is measured at the
 Copper
Copper
tube
Impression  compound
compound
Crown
preparation
 Crown
Crown
shoulder
Fig. 17.2 Diagram illustrating the principle of the copper ring technique for obtaining impressions of crown preparations.
Table 17.2 Flow of impression compound as required by ADA specification no 3, and BS 3886.
Flow |
at 37ºC |
at 45ºC |
|
|
|
Type I |
20% or less† |
85% or more |
|
6% or less* |
|
Type II |
2% or less |
between 70 and 85% |
|
|
|
* ADA specification no 3.
† BS 3886.
stated temperature by applying a load of 2 kg to the flat ends of a cylindrical specimen 6 mm high by 10 mm diameter for 10 minutes.
The other main requirement of standards is for impression taking properties. This applies to type I materials only. The material should be capable of recording sharp grooves 0.2–4 mm wide cut into the surface of a metal test block.
Impression compound is the most viscous of the impression materials in common use. Table 17.3
150 Chapter 17
Table 17.3 Viscosity values for some impression materials.*
Material |
Viscosity (Pas) |
|
|
Impression compound |
4000 |
Impression plaster |
60 |
Zinc oxide/eugenol paste |
60 |
Alginate |
50 |
Light-bodied elastomer |
30 |
‘Putty’ elastomer |
800 |
* Measured at 50 s−1 shear rate at 23ºC and 1 minute after mixing – for materials which require mixing.
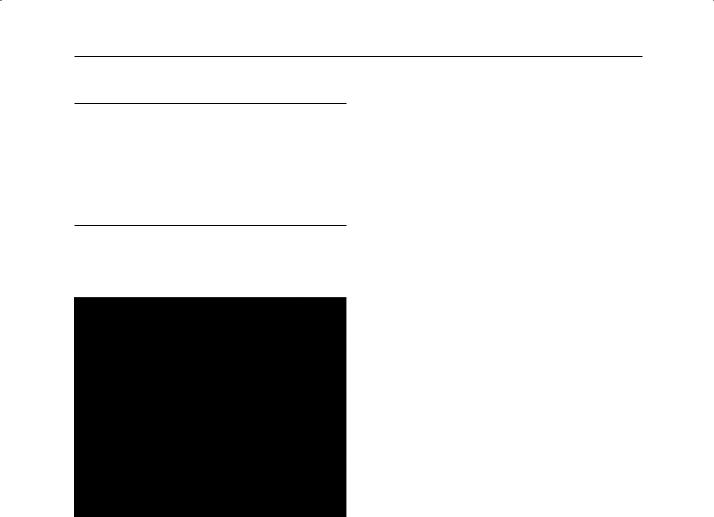
Fig. 17.3 This shows a typical edentulous impression recorded in impression compound. Note the lack of any fine detail in this impression due to the very high viscosity of the material.
gives typical values of viscosity for some materials, measured at a given shear rate. It can be seen that under these conditions the viscosity is some 70 times greater than that for impression plaster and more than 100 times greater than values for some of the light-bodied elastomers. The very high viscosity of impression compound is significant in two ways. Firstly, it limits the degree of fine detail which can be recorded in an impression. (see Fig. 17.3) Secondly, it characterises compound as a mucocompressive impression material. In certain circumstances, the high viscosity is used to advantage. For example, when recording impressions of some edentulous patients it is necessary to record the full depth of the sulcus so that a denture with adequate retention can be designed.
Only a viscous material, such as compound, is able to displace the lingual and buccal soft tissues sufficiently.
Compound is fairly rigid after setting and has poor elastic properties. A large stress would be required to remove an impression from undercut areas and the resultant impression would be grossly distorted. The materials have large values of coefficient of thermal expansion and undergo considerable shrinkage on removal from the mouth. This can be partially overcome by resoftening the surface of the impression with a flame and reseating the impression.
Three factors combine to produce significant internal stresses within the compound impression.
(1)The high value of coefficient of thermal expansion.
(2)The poor thermal conductivity.
(3)The relatively large temperature drop from the softening temperature to room temperature.
The gradual relief of internal stresses may cause distortion of the impression. For the most accurate results, the model should be poured as soon as possible after recording the impression.
Impression compound is most widely used for recording preliminary impressions of edentulous arches. The high viscosity of the material enables the full depth of the sulcus to be recorded. This gives a model on which a special tray can be constructed. A major impression is recorded in the special tray using a less viscous material, such as zinc oxide/eugenol impression paste.
The use of impression compound has declined markedly over recent years as newer materials and techniques have become available. The declining use of impression compound is reflected in the lack of any development of an international standard (ISO) for these materials. Impression compound is still used widely in stick form to modify/refine the peripheral extent of a special tray, particularly for complete dentures or in the edentulous regions for partial dentures. Denture retention relies on a number of factors including developing an adequate border seal around the denture against the soft tissues. This is achieved by extending the denture so that it just begins to displace the movable soft tissues at the periphery of the denture. Obviously such extensions cannot impinge on areas of muscle activity or the denture