

100_Cases_in_Clinical_Medicine
.pdfThis page intentionally left blank
CASE 50: CHEST PAIN AND SHORTNESS OF BREATH
History
A 29-year-old woman complained of a sudden onset of right-sided chest pain with shortness of breath. It woke her from sleep at 3.00 am. The pain was made worse by a deep breath and by coughing. The breathlessness persisted over the 4 h from its onset to her arrival in the emergency department. She has a slight non-productive cough. There is no relevant previous medical history except asthma controlled on salbutamol and beclometasone. There is no family history of note. She works as a driving instructor and had returned from a 3-week holiday in Australia 3 weeks previously. She had no illnesses while she was away. She has taken an oral contraceptive for the last 4 years.
Examination
She has a temperature of 37.4°C, her respiratory rate is 24/min, the jugular venous pressure is raised 3 cm, the blood pressure is 110/64 mmHg and the pulse rate 128/min. Peak flow rate is 410 L/min. In the respiratory system, expansion is reduced because of pain. Percussion and tactile vocal fremitus are normal and equal. A pleural rub can be heard over the right lower zone posteriorly. There are no other added sounds. Otherwise the examination is normal.
INVESTIGATIONS
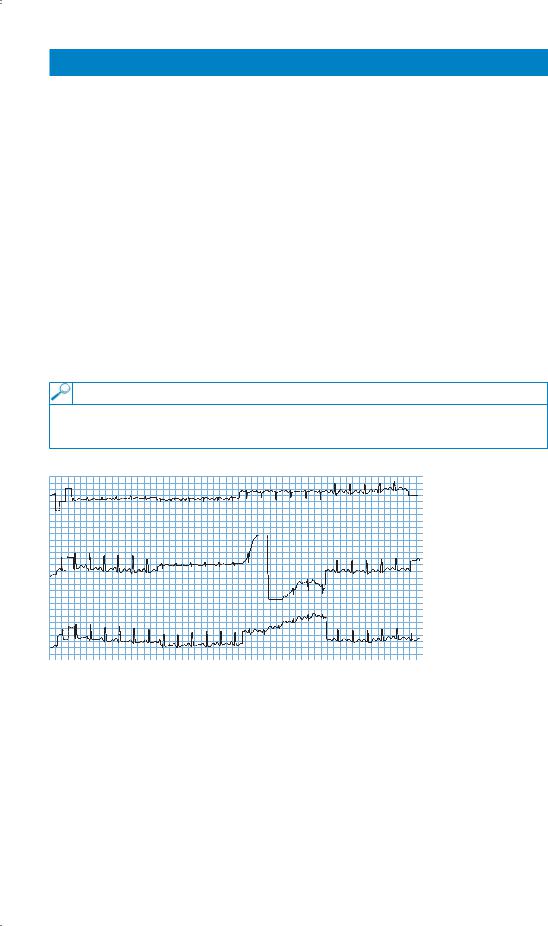
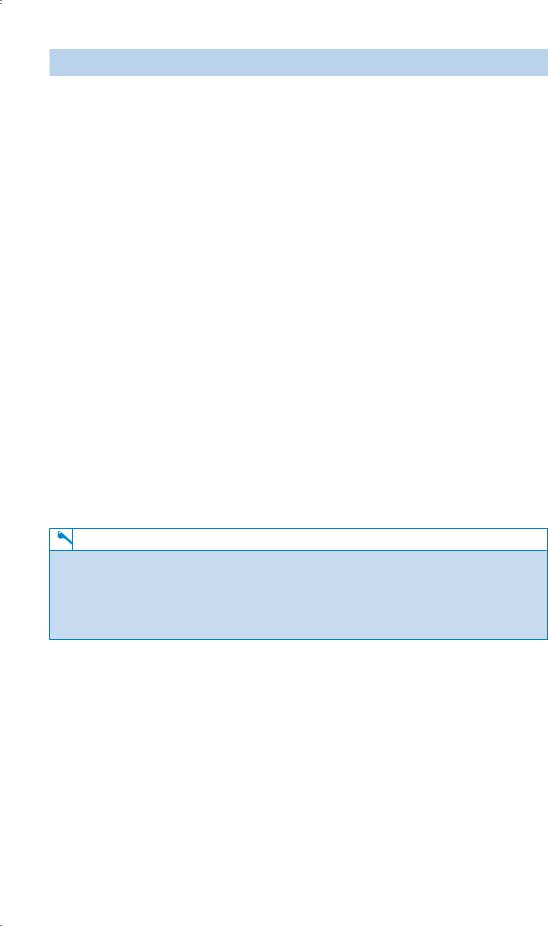
•An electrocardiogram (ECG) is shown in Fig. 50.1.
•Fig. 50.2 shows her chest X-ray.
Figure 50.1 Electrocardiogram.
130

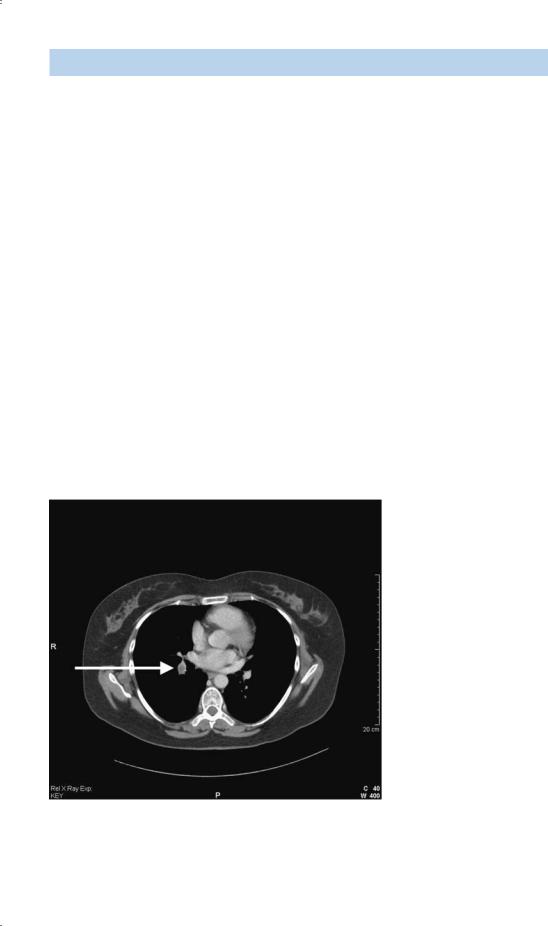
Figure 50.2 Chest X-ray.
Questions
•What is the likely diagnosis?
•How can it be confirmed?
131
ANSWER 50
This woman has had a sudden onset of pleuritic pain, breathlessness and cough. The physical signs of tachypnoea, tachycardia, raised jugular venous pressure and pleural rub would fit with a diagnosis of a pulmonary embolus. The peak flow of 410 L/min indicates that asthma does not explain her breathlessness.
The differential diagnosis would include pneumonia, pneumothorax and pulmonary embolism. The clinical signs do not suggest pneumothorax or pneumonia. Possible predisposing factors for pulmonary embolism are the history of a long aeroplane journey 3 weeks earlier, oral contraception and her work involving sitting for prolonged periods. Other predisposing factors such as intravenous drug abuse should be considered. The ECG shows a sinus tachycardia. The often-quoted pattern of S-wave in lead I, Q-wave and T inversion in lead III (S1Q3T3) is not common except with massive pulmonary embolus. Other signs such as transient right ventricular hypertrophy features, P pulmonale and T-wave changes may also occur. The chest X-ray is normal, ruling out pneumothorax and lobar pneumonia.
A ventilation–perfusion lung scan could be done looking for a typical mismatch with an area which is ventilated but not perfused. This result would have a high probability for a diagnosis of pulmonary embolism. A pulmonary arteriogram has been the ‘gold standard’ for the diagnosis of embolism but is a more invasive test. In cases with a normal chest X-ray and no history of chronic lung disease, equivocal results are less common and it is not usually necessary to go further than the lung scan. In the presence of chronic lung disease such as chronic obstructive pulmonary disease (COPD) or significant asthma, the ventila- tion–perfusion lung scan is more likely to be equivocal and further tests are more often used. In this case a computed tomography (CT) pulmonary angiogram was carried out (Fig. 50.3). This showed a filling defect typical of an embolus in the right lower lobe pulmonary artery.
Figure 50.3 Computed tomography pulmonary angiogram.
A search for a source of emboli with a Doppler of the leg veins may help in some cases, and the finding of negative D-dimers in the blood makes intravascular thrombosis and embolism unlikely.
132
Immediate management should involve heparin, usually as subcutaneous low-molecular- weight heparin. The anticoagulation can then transfer to warfarin, continued in a case like this for 6 months. Alternative modes of contraception should be discussed and advice given on alternating walking or other leg movements with her seated periods at work. Thrombolysis should be considered when there is haemodynamic compromise by a large embolus.
KEY POINTS
•In the presence of a normal chest X-ray and no chronic lung disease, the ventilation–perfusion lung scan has good sensitivity and specificity.
•The chest X-ray and ECG are often unhelpful in the diagnosis of pulmonary embolism.
•CT pulmonary arteriogram is used when ventilation–perfusion scanning is likely to be unhelpful.
133
CASE 51: CHEST PAIN
History
A 62-year-old man is admitted to hospital with chest pain. The pain is in the centre of the chest and has lasted for 3 h by the time of his arrival in the emergency department. The chest pain radiated to the jaw and left shoulder. He felt sick at the same time. He has a history of chest pain on exercise which has been present for 6 months. He has smoked 10 cigarettes daily for 40 years and does not drink alcohol. He has been treated with aspirin and with beta-blockers regularly for the last 2 years and has been given a glyceryl trinitrate spray to use as needed. This turns out to be two or three times a week. His father died of a myocardial infarction aged 66 years and his 65-year-old brother had a coronary artery bypass graft 4 years ago.
He has no other previous medical history. He works as a security guard.
Examination
He was sweaty and in pain but had no abnormalities in the cardiovascular or respiratory systems. His blood pressure was 138/82 mmHg and his pulse rate was 110/min and regular.
INVESTIGATIONS
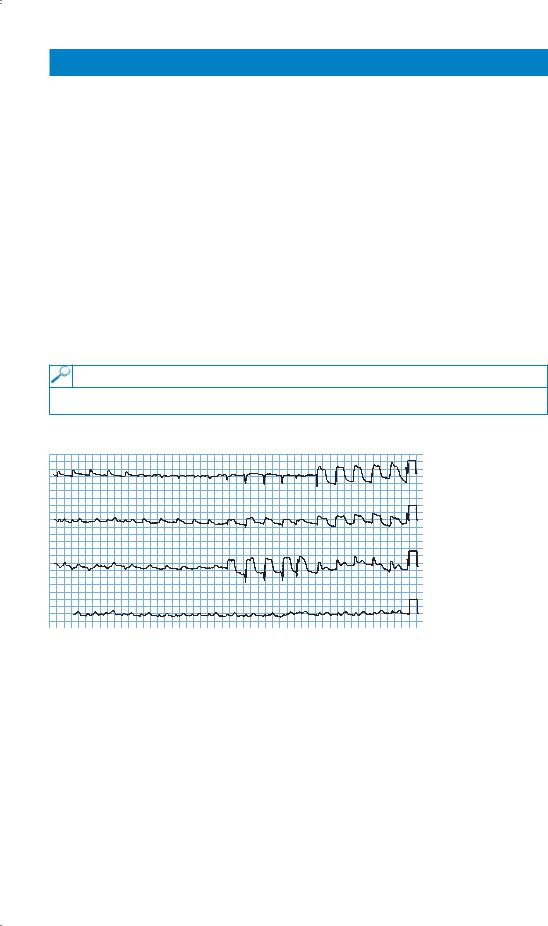
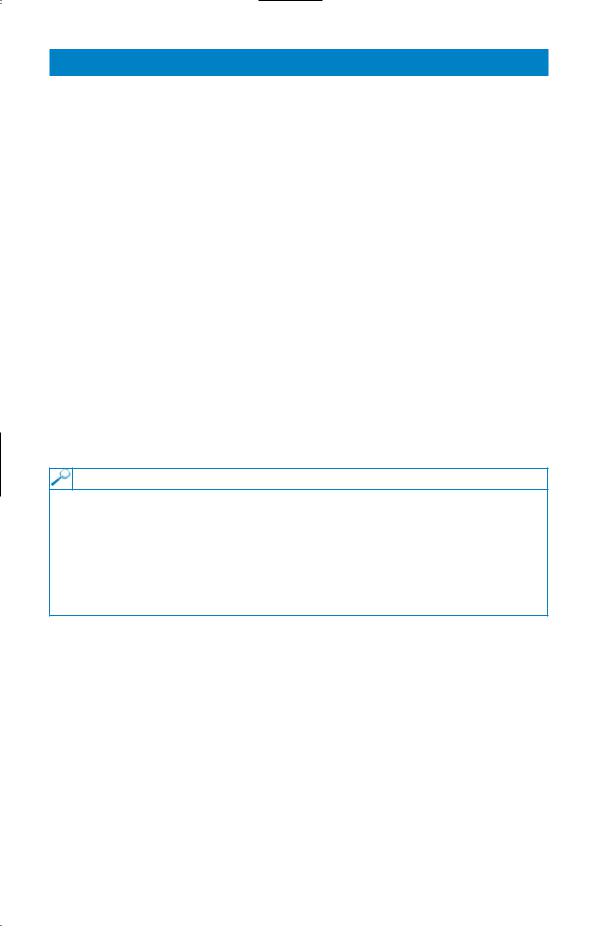
His electrocardiogram (ECG) is shown in Fig. 51.1.
I |
aVR |
V1 |
V4 |
II |
aVL |
V2 |
V5 |
III |
aVF |
V3 |
V6 |
II
Figure 51.1 Electrocardiogram.
He was given analgesia and thrombolysis intravenously and his aspirin and beta-blocker were continued. His pain settled and after 2 days he began to mobilize. On the fourth day after admission, he became more unwell.
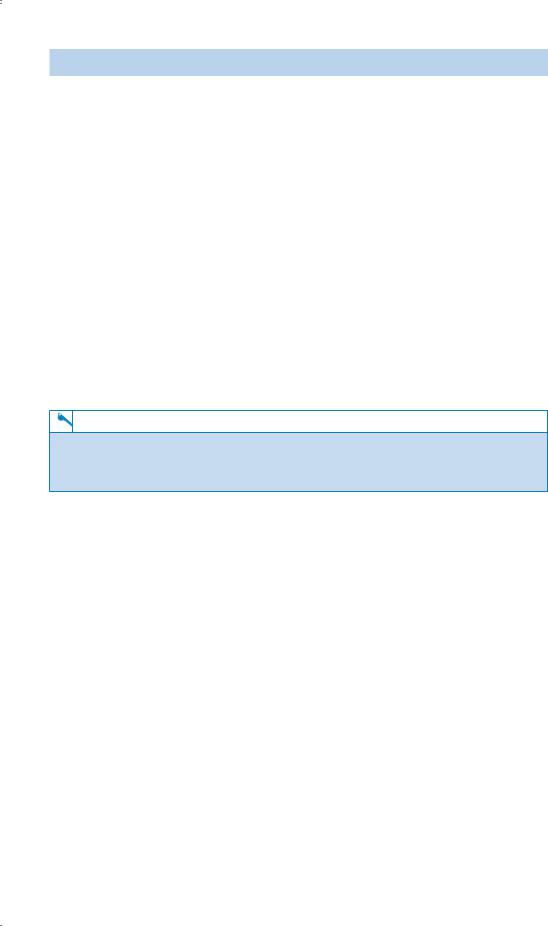
On examination, now his jugular venous pressure is raised to 6 cm above the manubriosternal angle. His blood pressure is 102/64 mmHg, pulse rate is 106/min and regular. His temperature is 37.8°C. On auscultation of the heart, there is a loud systolic murmur heard all over the praecordium. In the respiratory system, there are late inspiratory crackles at the lung bases and heard up to the mid-zones. There are no new abnormalities to find elsewhere on examination. His chest X-ray is shown in Fig. 51.2.
134

Figure 51.2 Chest X-ray.
Questions
•What is the likely diagnosis?
•How might this be confirmed?
135
ANSWER 51
This 62-year-old man had an anteroseptal myocardial infarction indicated by Q-waves in V2 and V3 and raised ST segments in V2, V3, V4 and V5. He became unwell suddenly 4 days later having had no initial problems. The late inspiratory crackles are typical of pulmonary oedema and the chest X-ray confirms this showing hilar flare with some alveolar filling, Kerley B lines at the lung bases and blunting of the costophrenic angles with small pleural effusions.
The problems likely to occur at this time and produce shortness of breath are a further myocardial infarction, arrhythmias, rupture of the chordae tendinae of the mitral valve, perforation of the intraventricular septum or even the free wall of the ventricle, and pulmonary emboli. The first four of these could produce pulmonary oedema and a raised jugular venous pressure as in this man. Pulmonary embolism would be compatible with a raised jugular venous pressure but not the findings of pulmonary oedema on examination and X-ray.
Acute mitral regurgitation from chordal rupture and ischaemic perforation of the interventricular septum both produce a loud pansystolic murmur. The site of maximum intensity of the murmur may differ being apical with chordal rupture and at the lower left sternal edge with ventricular septal defect, but this differentiation may not be possible with a loud murmur. The differentiation can be made by echocardiography.
The management of acute ventricular septal defect or chordal rupture would be similar and should involve consultation with the cardiac surgeons. When these lesions produce haemodynamic problems, as in this case, surgical repair is needed, either acutely if the problem is very severe, or after stabilization with antifailure treatment or even counterpulsation with an aortic balloon pump. Milder degrees of failure with a pansystolic murmur may occur when there is ischaemia of the papillary muscles of the mitral valve. This is managed with antifailure treatment, not surgical intervention, and can be differentiated by echocardiography.
KEY POINTS
•The cause of breathlessness after myocardial infarction needs careful evaluation.
•The signs of ischaemic ventricular septal defect and mitral regurgitation due to chordal rupture after myocardial infarction may be very difficult to differentiate.
•Patients with angina or myocardial infarction can also present with the radiating pain but no central chest pain, or with only the cardiac effects and no pain at all.
136
CASE 52: GENERAL WEAKNESS
History
An 82-year-old man is sent up to the emergency department by his general practitioner (GP). He is complaining of weakness and general malaise. He has complained of general pains in the muscles and he also has some pains in the joints, particularly the elbows, wrists and knees. Three weeks earlier, he fell and hit his leg and has some local pain related to this.
He is a non-smoker who does not drink any alcohol and has not been on any medication. Twelve years ago he had a myocardial infarction and was put on a beta-blocker but he has not had a prescription for this in the last 6 years. Twenty years ago he had a cholecystectomy. He used to work as a labourer until his retirement at the age of 63 years.
He lives alone in a second-floor flat. His wife died 5 years ago. He has one son who lives in Ireland and whom he has not seen for 3 years.
Examination
He is tender over the muscles around his limb girdles and there is a little tenderness over the elbows, wrists and knees. The mouth looks normal except that his tongue appears rather smooth. He has no teeth and has lost his dentures. There are no other abnormalities to find in the cardiovascular, respiratory or alimentary systems. In the legs, he has a superficial laceration on the front of the right shin. This is oozing blood and has not healed. There is a petechial rash on some areas of the legs. There are some larger areas of bruising on the arms and the legs which he says have not been associated with any trauma.
INVESTIGATIONS
|
|
Normal |
Haemoglobin |
10.1 g/dL |
13.7–17.7 g/dL |
Mean corpuscular volume (MCV) |
74 fL |
80–99 fL |
White cell count |
7.9 % 109/L |
3.9–10.6 % 109/L |
Neutrophils |
6.3 % 109/L |
1.8–7.7 % 109/L |
Lymphocytes |
1.2 % 109/L |
1.0–4.8 % 109/L |
Platelets |
334 % 109/L |
150–440 % 109/L |
Questions
•What essential area of the history is not covered above?
•What is the likely diagnosis?
137
ANSWER 52
A dietary history is an essential part of any history and is particularly important here where a number of features point towards a possible nutritional problem. He has been a widower for 5 years with no family support. He lives alone on a second-floor flat which may make it difficult for him to get out. He has lost his dentures which is likely to make it difficult for him to eat.
He has a petechial rash which could be related to coagulation problems, but the platelet count is normal. It would be important to examine the rash carefully to see if it is distributed around the hair follicles. A number of the features suggest a possible diagnosis of scurvy from vitamin C deficiency. Body stores of vitamin C are sufficient to last 2–3 months. The rash, muscle and joint pains and tenderness, poor wound healing and microcytic anaemia are all features of scurvy. The classic feature of bleeding from the gums would not be present in an edentulous patient.
Plasma measurements of vitamin C are difficult because of the wide range in normal subjects. In this patient, replacement with ascorbic acid orally cleared up the symptoms within 2 weeks. It would be important to look for other nutritional deficiencies in this situation and to make arrangements to ensure that the situation did not recur after his discharge from hospital.
KEY POINTS
•A nutritional history should be part of any clinical assessment, particularly in the elderly.
•Vitamin deficiencies can occur in patients on a poor diet in the absence of any problem with malabsorption.
138