

Theme № 14 Radio methods of the thoracic cavity organs examination. Radio signs of the respiratory organs diseases
The Radio methods of the thoracic cavity organs examination and their description: the methods of the respiratory organs morphological changes study (fluoroscopy |, sciagraphy, fluorography |, linear tomography |, computer tomography|, ultrasonic examination, magnetical resonance imaging|, bronchography |, angiopulmonography |, bronchial arterioraphy| CT-| and МР- angiography |); the lungs function methods of the study (inhalation and perfusion scintigraphy|, fluoroscopy |), functional tests and their value|importance,meaning| for the lungs function study. The image receipt principles |representation|, the testimony. Choice of radio apaque| matters and RPhP|. The respiratory organs radio anatomy and physiology: thorax, thracheo-bronchial tree, lungs roots and lung pattern, their morphological substrate|. Ages features of the lungs radio anatomy and physiology.
The respiratory organs diseases roentgenologic signs: darkenings and brightening of the pulmonary field, changes oflung pattern, changes of the lungs roots, displacement of the mediastinal organs|. Description of darkenings on sizes|dimensions|, amount|quantity|, intensity, form|shape|, structure, contours. Symptoms of the lungs ventilation violation and perfusion. Plan of the thoracic cavity organs surveying|survey study. The lungs and mediastinum pathology main|main| roentgenologic syndromes|, their morphological substrate|.
The magnetical resonance imaging semiotics of the lugs and mediastinum pathology|. Basic|main| magnetical resonance imaging syndromes of the lugs and mediastinum pathology|, their morphological substrate|.
The radionuclei | semiotics of the lugs pathology - violations of pulmonary perfusion | and ventilation, diffuse and focal processes in lungs, pathological content, in a pleura cavity. Basic|main| radionuclei | syndromes of the lungs pathology, their morphological substrate|.
Ultrasonic semiotics of the lungs pathology (subpleurae exudate|), pleura cavity and mediastinum| - tumours|swelling|, cavernous educations|formations| megascopic lymphatic nodes. Basic|main| ultrasonic syndromes of the lungs and mediastinum pathology|, their morphological substrate|.
Methods of roentgenological examination
The roentgenological examination methods of thoracic cavity organs are divided into contrasting, non-contrasting and radiofunctional. To the non-contrasting methods belong:
1. Fluorography;
2. Sciagraphy;
3. Roentgenoscopy;
4. Tomo- and zonography;
5. Computer tomography;
6. Electro-sciagraphy
The contrasting methods of roentgenological examination are:
1. Bronchography;
2. Angiopulmonography;
3. Artificial pneumothorax;
4. Pneumoperitoneography;
5. Pneumomediastinography;
6. Pleurography;
7. Fistulography and others.
Roentgenofunctional methods are:
1. The methods of roentgenological examination which use the Valsalve’s, Muller’s functional tests;
2. Roentgenokymography;
3. Roentgenocinematography and others.
The fluorography is applied for conducting of the population large contingents prophylactic inspections.

Fig.14.1The principle of fluorography (chart)
The roentgenoscopy is used for the study of respiratory organs structure and function.
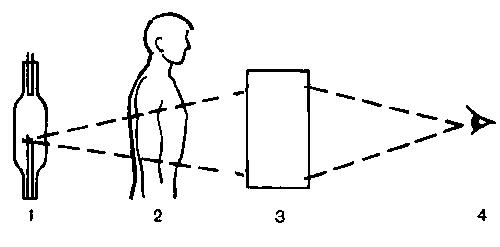
Fig.14.2 The principle of roentgenoscopy
1- radiation sourses; 2- examination object; 3- image collector; 4 - doctor-roentgenologist
The sciagraphy image of the thoracic organs


Fig.14.3 Sciagrams of normal thorax are in anterior view and lateral projection
The linear tomography is used for study of the pathological educations structure; the trachea, large bronches, lungs root, and mediastinum state.

Fig.14.4The linear tomography principles
The X-ray computer tomography is used to study the pathological process structure, its extension in surrounding organs, and lungs diseases differential diagnostics. It is possible to distinguish shades of the pulmonary vessels, the bronches, and lymphatic nodes in thoracic cavity with lungs computer tomography. The pulmonary tissue densitometrical closeness is 650 - 850 НU, mediastinal adipous tissue - 70 - 120 НU.
Spiral CT-angiography – method of the lungs vessels defeats diagnostics. It gives diagnostic information about narrowing nature|nature|, morphology of atherosclerotic plague and vascular wall, about pathological arteries deformation. The method allows to expose the vessels blood thrombus.


Fig.14.5 a) a survey sciagram of thorax is in the anterior view; b) linear tomograma of thorax in the anterior view of a patient with pathological education in right lung; in) thoracal computer tomography in an axillar projection at the pathological education level.
The magnetical resonance imaging is used as addition to computer tomography mainly for examination of mediastinal organs, because pulmonary tissue gives a weak signal.
By MRI it is possible to get cuts not only in axillar but also in other planes – the sagital and anterior view.
The bronchography is used to expose the trachea and bronches morphological changes, anomalies of development, bronchoectasis, bronchial fistules, and tumours by contrasting matters which are entered through a catheter.

Fig.14.6 a) normal bronchogram of the right lung, anterior view: b) lateral bronchogram of a patient with bronchoectatic disease.
The angiopulmonography - lungs vessels contrasting examination after catheterisation of the median basilica vein (general angiopulmonography) with subsequen series implementation of sciagrams with a short interval by an automatic device. For implementation of the selective angiopulmonography catheter is entered into the subclavian vein and farther under X-ray control consistently is conducted through superior vena cava, right auricle, right ventricle, and pulmonary trunk to the necessary pulmonary, partial or segmentar artery. Indication for angiopulmonography is a suspicion on tromboembolism of pulmonary artery, arteries development anomalies, such as arteriovenular fistula and aneurysm.
Sometimes bronchial artery contrasting is conduct for differential diagnostics of the lungs tumours|swelling| and chronic inflammatory processes.

Fig.14.7Angiopulmonograma
The ultrasound is used for examination of the heart, other mediastinal organs, pleura, diaphragm, superficial departments of lungs, patological maintenance in a pleura cavity, and integrity of ribs. Deep into pulmonary parenchym an ultrasound does not penetrate.
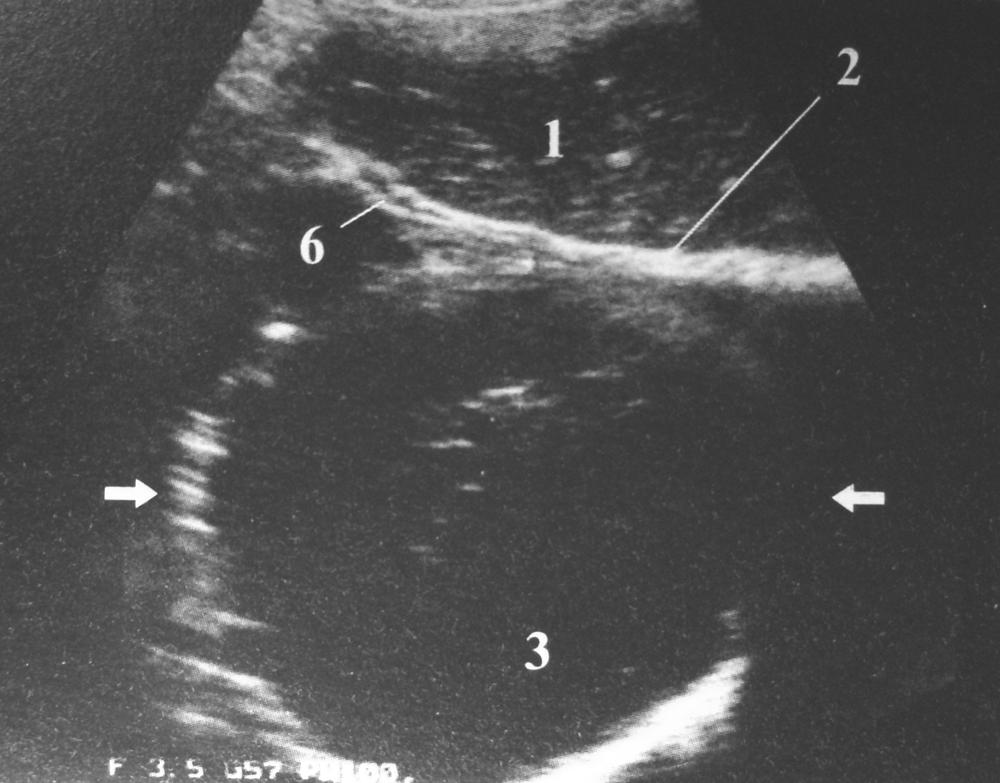
Fig.14.8 The malignant tumour in lungs: 1 liver: 2 diaphragma; 3 tumour; 6 diafragmal pleura
The radionuclear method is a basic method of the lungs function, studing which allows to study consisting of ventilation, blood stream and lungs perfusion.
For inhalation scintigraphy rare gases like 133Хе, 81тCr and aerosol 99mТс are used; the areas of the reduced accumulation of radiopharmaceutic preparation (RPhP) in lungs are observed at bronchial asthma, bronchitis, bronchial tumour and other diseases which are accompanied by the decline of ventilation.



Fig.14.9 Chart of lungs inhalation scintigraphy
To conduct the perfusional scintigraphy intravenously introduct albumen, marked of 99mТс; the RPhP decline accumulation is observed in the certain areas of pulmonary parenchyma, where is the blood circulation is reduced.


Fig.14.10 Feathers perfusious scintigraphy. Chart
а) lungs scintigram, a norm; b) lungs scintigram, the RPhP fixing absence in the right lung superior lobe(tumour)
The Punction biopsy – excision of the lungs tissues under roentgencontrol with bronchoscope through nasal ways (aspirational bronchoscopy), or by a punctional needle through a thoracic wall.

Fig.14.11 A trance-bronchial biopsy of the left lung upper lobar bronchus
The thoracic organs roentgenanatomy
On a survey sciagram in the anterior view almost on all of draught the superior are determined 7 pair of ribs. Lower ribs are partly hidden by the diaphragmal shade and abdominal region organs. Cartilaginous parts of the ribs do not give noticeable shade on sciagrams. Only after 30, beginning from the 1th costal cartilage, for them a lime is put aside as narrow ribbons along contour and small aits in the center of cartilage.
A shoulder-blade and collar-bone is well noticeable at X-ray scopy and on the sciagram. At the patient correct position in the anterior view, the collar-bones sternumends are disposed symmetric on identical distance from a vertebral column.The sternumsade in the anterior view is non-noticeable. In a lateral projection shade of sternum is formed.

Fig.14.12 Image on the anterior view sciagram (chart)
1-sternocleidomastoid muscle; 2-first rib; 3 collar-bone; 4-breastbone handle; 5-trachea; 6-greater petoral muscle; 7-calcification of costal cartilage; 8-nipple; 9-mammary gland; 10-armpit cavity; 11-shoulder-blade.
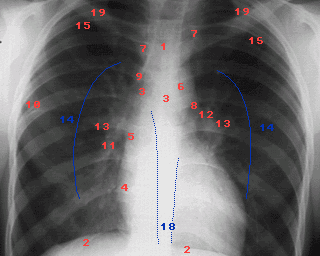
Рiс.14.13 Sciagram of the thoracal|mew| organs (marked elements of anatomic formations|formations|):1-trachea; 2-diaphragm; 3-right and left main|head,leading| bronches; 4-arc of the right auricle; 5-descendence| part|portion| of aorta; 6-aortal arc; 7-projection of subclavial arteries; 8-right heart border|line,boundary| (from above to downof the| arc: ascending part|portion| of aorta, the cone of pulmonary artery, auricle of the left auricle and left ventricle); 9-azygos vein; 10-horizontal interlobar| fissura; 11-intermediate pulmonary artery; 12-left main|head,leading| pulmonary artery; 13-lungs roots; 14-segmentar arteries(sub-root| area|zone|); 15-vessels of a 2nd intervertebral| interval|space| (in the norm|standard| 3 mm| in a diameter); 16-rounded shades|shadows| of anterior segmentar bronches; 18-back bends of pleura;19-ribs;
Diaphragm as the light pulmonary fields together with the organs of abdominal region limit from below as the clear arched intensive shade. Only on the left of medial line it is possible to see brightening air of stomach bubble. The right cupula of diaphragm takes a place at the level of anterior ends of 5-6th ribs, and left - on one rib below.
The costaodiaphragmal receses (or sines) are noticeable in the lateral corners of diaphragm cupulas, and in medial corners are costomediastinal recesses. In lateral projection anterior costodiaphragmal recesses are placed higher of back.
In the anterior view select such pulmonary fields: 1) apex placed higher collar-bones; 2) superior - from a collar-bone to the 2 rib; 3) middle - from 2 to the 4 rib; 4) inferior - from the 4 rib to the diaphragm.
In a lateral projection well is evidently the shade of breastbone, shoulder-blades, 6th -9th thorasic vertebraes from which obliquely shades of ribs followed downward. Narrower and more expressly are shadesof the ribs near the cassette. Light areas between a breastbone and a heart with an aorta name retrosternalis space, and between a heart and vertebral column - retrocardialis space.
Shade of root lungs are formed large pulmonary arteries, veins, bronches, lymphatic vessels and nodes. In the anterior view this shade is not homogeneous (structured), located at the level of anterior ends of the 2-4th ribs, in a widdth about 2sm, occupies the not more than fourth of transversal size lungs. A root of left lungs placed higher than right, and his lower part close cardiac shade. In a lateral projection roots of lungs are under the arc of aorta.
Most thoracic lymphatic nodes are in the lungs roots and mediastinum. In the case of inflammatory and tumour processes they are increased and shade of root becomes homogeneous and unstructured.
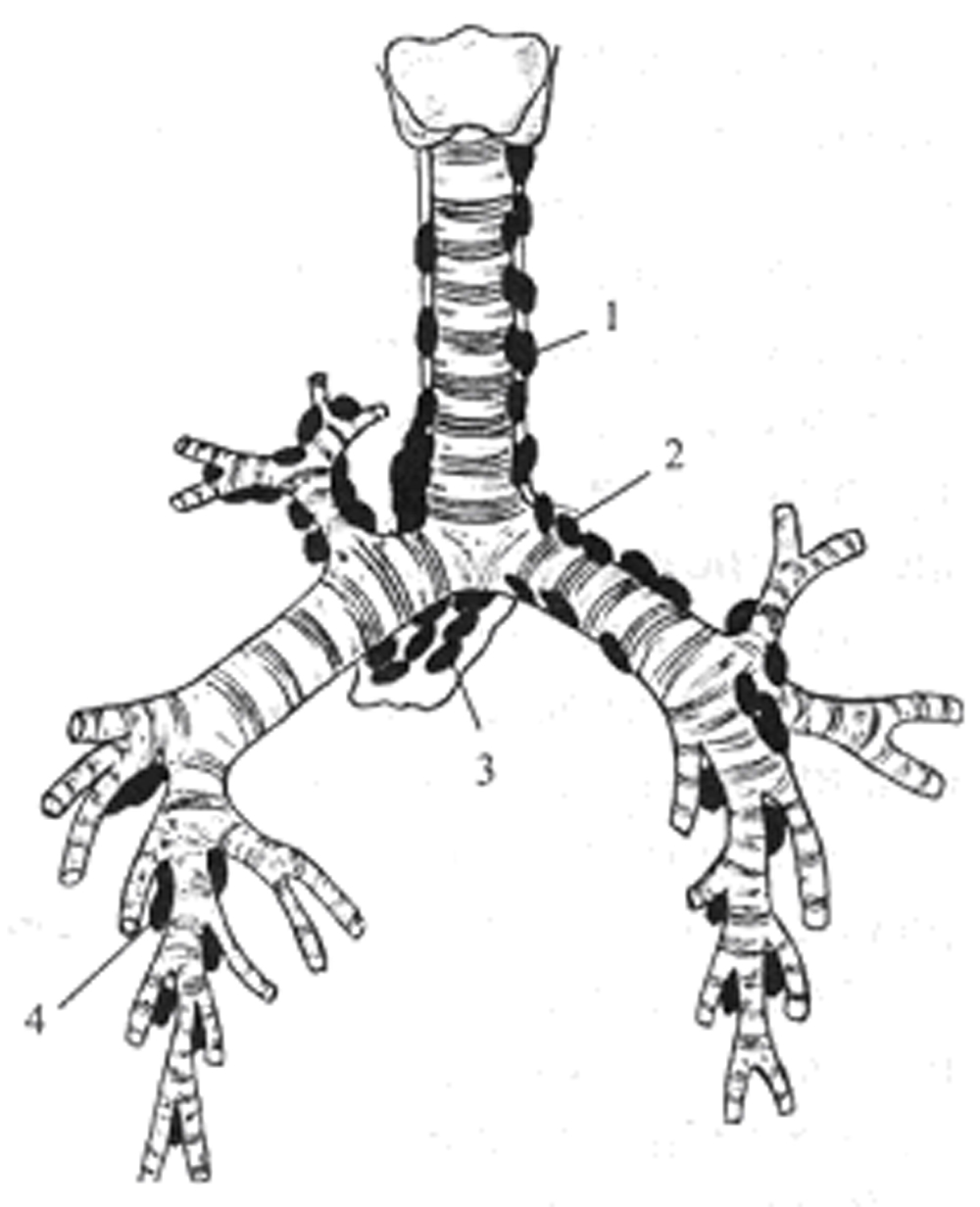
Fig.14.14 Intrathorasic lymphatic nodes
1 – paratrachealis; 2 – tracheobronchealis; 3 – bifurcational; 4 – bronchopulmonalis
Name linear shades of pulmonary vessels which walk away from the roots of lungs and a lung pattern, interlacing, are formed ansiform structure. The caliber of these shades gradually diminishes in anterior alion from roots and on 2 sm does not reach to the thorasic wall.
Parietal pleura can be traced in the anterior view as the thin arched strip which stretches from the apex of lateral surface lungs. Interlobar pleura and clear border between pulmonary lobes in the anterior view is not traced. The anterior view of oblique fissura goes from the 3rd thorasic vertebra obliquely aside and downward to the lateral surface of 4th rib and farther obliquely downward and priseredne to the diaphragm. A horizontal fissura of the right lung goes horizontally from the lateral surface of the 4th rib medialy. In a lateral projection the pleura of oblique interlobar fissura forms thin "hair" shade, that folowing from the level of 4th thorasic vertebra obliquely downward and anterior aly to the diaphragm. A horizontal fissura in a lateral projection begins from oblique at the level of root lungs and walks ahead to the thorasic wall almost horizontally.
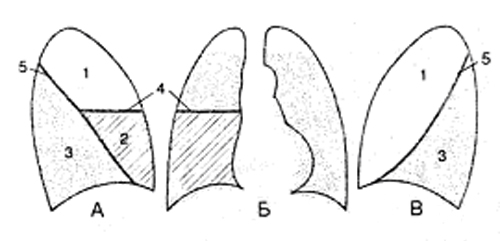
Fig.14.15 a projection of lobes and interlobar fissuras is on a sciagram (chart)
a) right lateral projection; b) anterior view; c) left lateral projection.
1-superior lobes; 2-middle lobe; 3-inferior lobes; 4-horizontal fissura; 5-oblique fissura
Lobes consist of segments, which have a wrong pyramids form the apexes of which are anterior aled to the roots, and bases - to the surface lungs.
Roentgenological border between bronchopulmonal segments is not traced; however for the pattern of localization of pathological process it is necessary to know the topographical structure of bronchial tree, lobes and segments. A right lung consists of 3 lobes 10 segments, left - from 2 lobes and 10 segments.



Fig.14.16 The schematic image of the lungs segments. Anterior view (А), right lateral (Б), left lateral (В) projections
1 - apex, 2 - back, 3 - anterior , 4 - lateral (in left lungs - superior uvular), 5 - medial (in left lungs - lower uvular), 6 – superior lower lobe; 7 - cardial (in left lungs absents often), 8 – anterior bazal, 9 – lateral basal, 10 - back basal.
RIGHT LUNG |
LEFT LUNG |
Superior lobe: |
Superior lobe: |
Apex segment (D1) |
Apex segment (S1) |
Back segment (D2) |
Back segment (S2) |
Anterior segment (D3) |
Anterior segment (S3) |
Middle lobe: |
Middle lobe: |
Lateral segment (D4) |
Superior uvular segment (S4) |
Medial segment (D5) |
Lower uvular segment (S5) |
Lower lobe: |
Lower lobe: |
Apex superior segment (D6) |
Apex superior segment (S6) |
Medial (cardiac) basal (D7) |
|
Anterior basal segment (D8) |
Anterior basal segment (S8) |
Lateral basal segment (D9) |
Lateral basal segment (S9) |
Back basal segment (D10) |
Back basal segment (S10) |
Organs inter localisation of superior mediastinum is on the horizontal (axial) cuts of thorasic cavity, got by CT and MRI.
Roentgen-anatomy| features of the children respiratory organs|kids|.
Thorax in new-born is short and wide.Intervertebral intervals|spaces| are wide. | The breast-bone consists of separate ossificated kernels.
A diaphragm at children|kids| under age one year is located on either side at the level of anterior departments of the 5th-6th ribs.
In new-born trachea is short (4-5 sm|). At children|kids| under age 3-4 years on the mediastinum background |a trachea and main|head,leading| bronches are differentiated as lengthened brithness|.
Lungs The obiqua pleural fissuras in new-born are located highly, that is why|that is why| inferior pulmonary lobes|bottom|lobes are greater than superior|upper,top|. Interlobar fissures do not reach to|by| the roots, in this connection an inflammatory|hot-tempered,ardent| process in sub-root areas|zones| can pass|turns| from one lobe|part,stake,portion,share| on other. In the bronches mucus shell lot of circulatory and lymphatic vessels are located, that is why|that is why| at inflammatory|hot-tempered,ardent| processes, communicating|passable| of bronches is often violated|excited| (hyperinflation, atelectasis |).
Lungs vessels. The pulmonary trunk|barrel| diameter at children|kids| is greater, than aortal one (to 10 years). The segmentar and sub-segmentar arteries at children|kids| under age 3 years relatively|in relation to| short, that is why|that is why| on the sciagram their transversal cuts are form the outlined focal| shades|shadows| of round and oval form|shape|.
The lungs roots at the children|kids| of early age are located at one level, their structure is homogeneous.
The computer tomography anatomy of the thoracic cavity organs. It is accepted to execute|implements| computer tomography| at certain|definite| anatomic levels. In accordance with|according to| these levels is developed a computer roentgen-anatomy| | (fig.17, A|but|, B, C, D, E, F, and G).
I. An apex|top| level or level of the|upper,top| superior thoracal aperture (0 mm|) passes through incisura|cutting| and sterno-clavicular connections|halving,compounds,junctions,joints,coupling|, 7th neck or 1st thoracic vertebra and 1st or 2nd ribs. Pulmonary parenchyma| shows itself as the lungs superior lobe apex|tops| segments. A trachea is expressly looked over in the tomography| cut center. Between the trachea anterior wall and.
quite often is visualized thyroid | gland |, and|but| between the trachea back wall and column anterior surface - esophagus|bac. In anterior lateral departments on trachea either side the brachiocephalic veins and arteries are located. The para-tracheal lumphatic nodes are visualized| round|about| the trachea (their diameter in a norm|standard| no more than 5 mm|). The vascular pattern at this level has the appearance of shallow|small| roundish or short line-like shades|shadows|.
II. The level of sternoclavicular joint (20 mm|) - along the collar-bone inferior|bottom| surface, through|from,because of| the handle of breast-bone|, areas of superior|upper,top| ribs and 2nd thoracic vertebra. Pulmonary parenchyma | is the lungs superior lobe apex|tops| segments|upper,top|. A vascular pattern has the appearance of roundish shades|shadows|. The brachiocephalic| veins are located at front trachea with diameter about 2 sm|. The common|common| carotid aryery is located between the left brachiocephalic| vein and anterior-left trachea | wall, behind from it - |left subclavian artery. Between a right brachiocephalic| vein and anterior trachea wall located right arterial brachiocephalic| trunkus|barrel| wider than the alongside located arteries. Between a trachea and the 2nd thoracic vertebral body situated esophagus, sometimes there is air in it|what|. On either sides of the trachea there are peratracheal limphatic nodes with the diameter of 5 mm.
III. The level of aortal arc (60mm) – from breast bone|, separate ribs areas, 4th thoracic vertebrae and the shoulder-blade superior|upper,top| third part. Pulmonary parenchyma| in anterior departments shows itself anterior segments, in middle are back segments of both superior|upper,top| lobes|parts,stakes,portions,shares|; in dorsal| departments are lungs inferior lobe apexes|tops| segments. The lungs vascular pattern nearer to|by| the roots has the appearance of the rounded and linear shades|shadows| which appear due to transversal and slanting to the cut of segmentar and subsegmentar vessels. Arteries and veins on lungs periphery| on this cut look like identical. Behind from the located ascending aorta that adjoins to|by| the anterior wall of trachea, and|but| on the right|it|--- is superior|upper,top| vena cava. Between it|it| and in anterior-right| trachea wall in cellulose there are limphatic nodes. The arc of aorta issituated from anterior |ahead|to back|backwards|, esophagus adjoins to|by| it|it|. The descending aorta is situated near the 4th thoracic vertebra anterior-left| contour.
IV. Level of the trachea bifurcation (70mm). T|he superior|upper,top|lobe lobe anterior segment is adjoins to anterior thoracic wall by the wide basis|foundation|. In right lung it medialy adjoins to|by| the ascending aorta right auricle and superior|upper,top| vena cava, and|but| in left lungs — to|by| the pulmonary trunk|barrel| In the central areas of this cut there are the segments of middle lobe|part,stake,portion,share| of right lungs and uvular segments of superior|upper,top|lobe lobe of left lung; the apexes|tops| of these segments are directed to|by| the proper roots, their wide basis|foundation| adjoins to|by| the anterior-lateral thoracic wall surface. The back departments of this cut occupy|borrows| the superior|upper,top| segments of the lungs lower|bottom| lobes|parts,stakes,portions,shares|. The apexes|tops| of these segments are directed to|by| the roots. The transversal cuts of right and left main|head,leading| bronches visualised| between an ascending aorta and body of the 5ththoracic vertebra. There is ascending aorta at the front of trachea bifurcation; the esophagus- behind and to the left of it|to the left fro.The superior|upper,top| vena cava is traced on the right side of the ascending aorta, on the left|on the left|-left pulmonary artery. The descending aorta is visualized between the left main|head,leading| bronchus back wall and body of the 5th thoracic vertebra. At this level right lungs root superior-lobe| part|portion| (superior-lobe| | right pulmonary artery) is traced on the right|to the right|, and|but| to the left|on the left|- segmentar bronches of the apex|top|, back, anterior and uvular segments.

Fig.14.17 The computer tomography anatomy of the thoracic cavity organs is executed|done,implemented| in the mode|regime| of lungs (A|but|, Б, В, Г, Д, Е, Є). The lungs segments are marked by the proper numbers.
V. The level of pulmonary artery (100mm) - from the sternumbody, 7th, 6th, 5th, ribs and 7th thoracic vertebra. In the lungs - on the right|to the right| is front segment of the right lungs superior|upper,top| lobe|part,stake,portion,share|; dorsally -| middle lobe|part,stake,portion,share| and basis|foundation| of apex|top| segment of the inferior lobe|part,stake,portion,share|; to the left|on the left| - front segment of the superior|upper,top| lobe superior-lingualis| segment|part,stake,portion,share|, to the left|on the left| dorsally|- basis|foundation| of the inferior lobe apex|top| segment|b|part,stake,portion,share|.
At this level large|great,big| vessels are expressly traced: at the front-|ahead|ascending aorta, to the left -a pulmonary trunk|barrel| with its|its| branches.
Between a right pulmonary artery and bulb|onion| of aorta there is superior|upper,top| vena cava. Dorsally| from right and left pulmonary arteries there are main|head,leading| bronches. Length of right bronchus - 2,2 sm; width - 1,53 sm, left accordingly - 5 sm and - 1,3sm. Arterial vessels in lungs accompany bronches and have a general|common| topography.
VI. The heart basis level |foundation| (140 mm) – from its|its| basis|foundation|, 8th, 9th thoracic vertebrae, inferior |bottom| ribs. The front areas of the lungs: on the right|to the right| - the medial and lateral right lung segments of the middle lobe|part,stake,portion,share|, to the left|on the left| - the uvular left lung superior|upper,top| lobe segments |part,stake,portion,share|. The middle areas of both lungs are situated in the inferior lobes anterior basis segments|parts,stakes,portions,shares|. In the back departmentsof the lungs inferior |bottom| lobes lateral and posterior segments are situated|parts,stakes,portions,shares|.
The lung vessels on this level in most cases are oriented horizontally and are traced on the tomography cut from the lungs roots, gradually narrowing to|by| the periphery. The pulmonary veins on either side of the lungs are situated near|by| the left auricle.
VII .The diaphragmal level (160 mm) – from 9th-10th thoracic vertebrae, 7th, 9th, 10th ribs, xiphoid process| or inferior |bottom| segment of the sternumbody and the heart inferior |bottom| departments.
Depending on a patient constitutional feature at this level in the center of the right lungs basis| department tthe right diaphragmal cupula of different|diverse| area is situated|. The parenchyma | of the both lungs is segments, what at previous|preliminary| level.
Between the sternum and the 9th - 10th thoracic vertebrae bodies the heart is situated.
The esophagus is situated at front of|in advance of| the 9th - 10th thoracic vertebrae bodies, more left from its - descending aorta; between the 9th-10th | thoracic vertebrae bodies and esophagus is azugos vein, and|but| between the 9th-10th thoracic vertebrae bodies and aorta is hemyazigos vein.