

Figure 4 Latent and active hiv infection in macrophages.
2.5 The Stages of hiv Infection
The progress of HIV infection in adults can be divided into three clinical phases (Figure 5):
Phase I. The number of viral RNA molecules per milliliter of blood plasma may reach more than 10 million in the first week or so. Billions of CD4 + T cells may be infected within a couple of weeks. Immune responses and fewer uninfected cells to target deplete viral numbers in blood plasma sharply within a few weeks. The infection may be asymptomatic or cause lymphadenopathy (swollen lymph nodes).
Phase 2. The numbers of CD4 + T cells decline steadily. HIV replication continues but at a relatively low level, probably controlled by CD8+ T cells and occurs mainly in lymphatic tissue. Only a relatively few infected cells release HIV, although many may contain viruses in latent or proviral form. There are few serious disease symptoms, but a decline in immune response may become apparent by the appearance of persistent infections by the yeast Candida albicans, which can appear in the mouth, throat, or vagina. Other conditions may include fever and persistent diarrhea.
Phase 3. Clinical AIDS emerges, usually within 10 years of infection. CD4 + T cell counts are below 350 cells/µl (200 cells/µl defines AIDS). Important AIDS indicator conditions appear, such as C. albicans infections of bronchi, trachea, or lungs; cytomegalovirus eye infections; tuberculosis; Pneumocystis pneumonia; toxoplasmosis of the brain; and Kaposi's sarcoma.
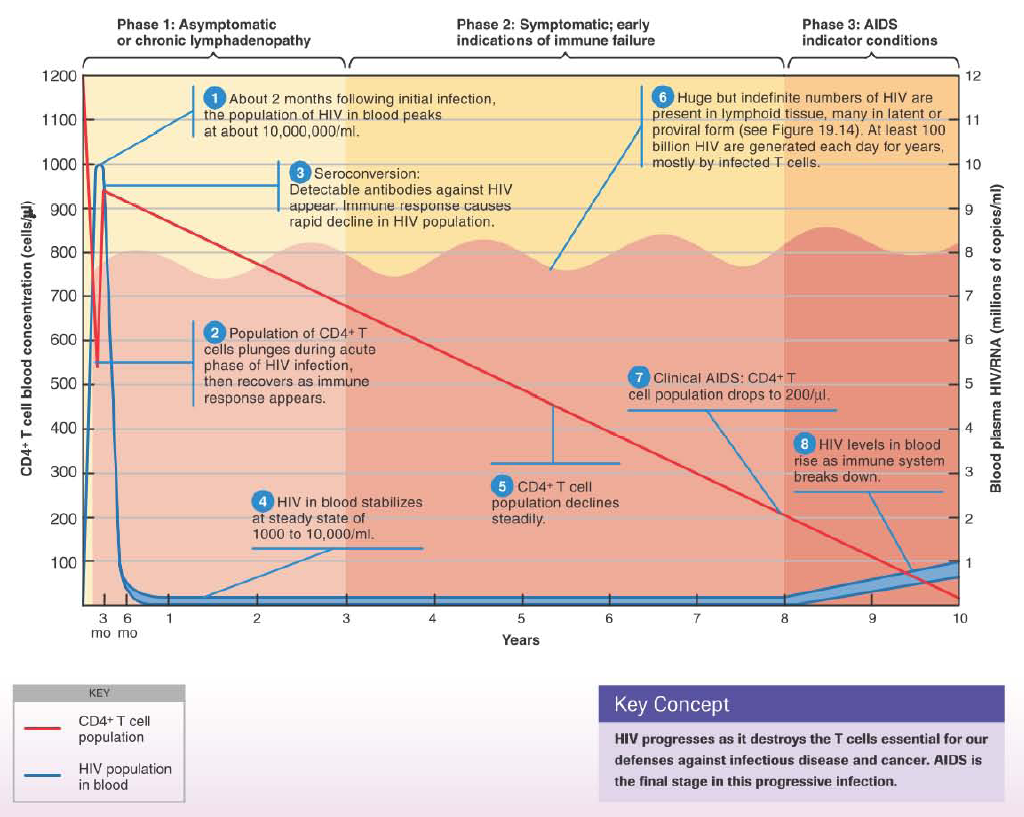
Figure 5. The progression of HIV infection
2.6 Hiv Vaccines
An important consideration for vaccine development is the fact that the immune system has not shown much capability in coping with natural infections. In some 60 million HIV infections worldwide, there is not a single known case in which the immune system has eradicated the virus. Obstacles to developing a vaccine for HIV are formidable, and the landscape is now littered with unsuccessful vaccine trials. The rapid mutation rate of HIV makes it difficult to develop a vaccine that is effective against all mutational variants of the virus that appear during the course of an infection. Furthermore, the virus has developed clades that differ substantially from one geographic area to another, and each would probably require an appropriate vaccine.
Ideally, a vaccine would produce antibodies that would prevent infection. The virus resists antibody binding until a last-second exposure just before attachment and entry into the host cell. For persons already infected, a successful cell-mediated-type vaccine would be necessary to control the progression of the disease. To be considered successful, however, the vaccine would have to stimulate the production of CTLs that are more effective than those produced in response to a natural infection. Cells infected by HIV, it happens, are not very susceptible to attack by CTLs. There is also the problem of a persistent, but immunologically invisible, viral population in the form of proviruses and latent viruses. Finally, a vaccine would have to be affordable in regions of the world where economic subsistence is often marginal. All in all, the development of an HIV vaccine is a formidable task. Some experts believe that no HIV vaccine is possible that will confer nearly complete protection, such as those for smallpox or measles. It is thought that a more practical goal may be to develop a vaccine with more modest goals than "sterilizing immunity." Perhaps a vaccine would
stimulate cell-mediated immunity in already infected persons and help the patient's existing immune system to clear the virus.