

Учебники / Operative Techniques in Laryngology Rosen 2008
.pdf158 |
Endoscopic Excision of Saccular Cyst |
|
Key Points
■Saccular cysts of the larynx in the adult can usually be managed endoscopically.
■Saccular cysts in infants and children are generally approached externally.
■Two anatomic types of saccular cysts occur
■Anterior
■Smaller in size
■Presents as a ventricular mass in the anterior half of the larynx
■Lateral
■Larger
■Presents as a bulge in the FVF/ aryepiglottic fold
■Endoscopic CO2 laser and cold dissection are used to remove the cyst.
■The dissection should include a complete removal of the FVF and underlying ventricle, to reduce the chance of recurrence.
Selected Bibliography
1Danish MN, Meleca RJ, Dworkin JP, Abbarah TR (1998) Laryngeal obstructing saccular cysts: a review of this disease and treatment approach emphasizing complete endoscopic carbon dioxide laser excision. Arch Otolaryngol Head Neck Surg 124:593–596
2DeSanto LW, Devine KD, Weiland LH (1970) Cysts of the larynx: classification. Laryngoscope 80:145–176
3Hogikyan ND, Bastian RW (1997) Endoscopic CO2 laser excision of large or recurrent laryngeal saccular cysts in adults. Laryngoscope 107:260–265
25
Chapter 26
Anterior Glottic Web |
26 |
|
26.1Fundamental and Related Chapters
Please see Chaps. 1, 4, 10, and 13 for further information.
26.2Disease Characteristics and Differential Diagnosis
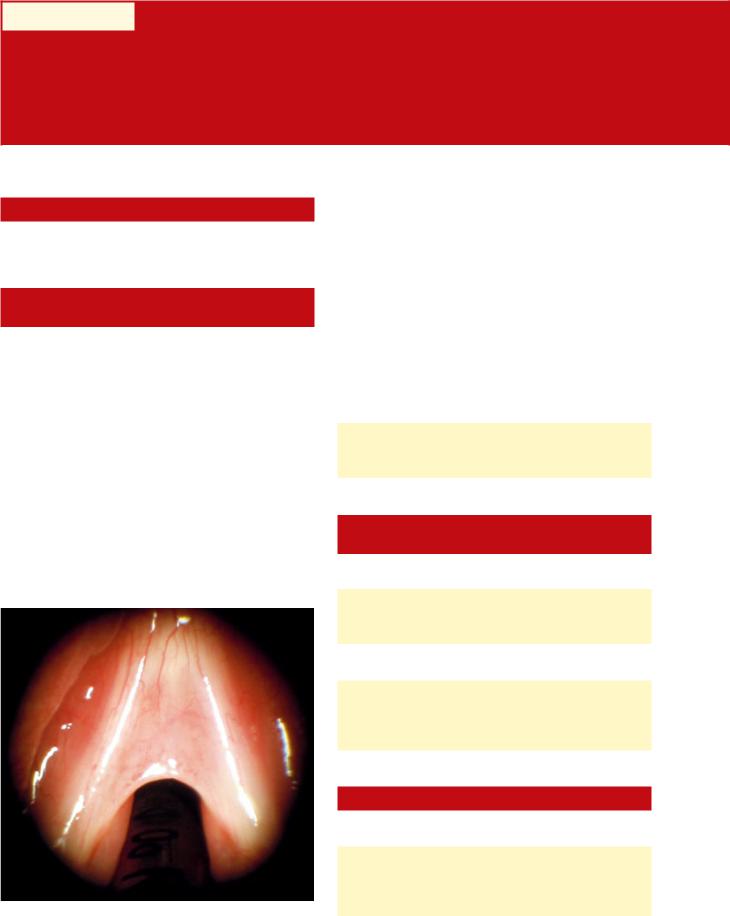
An anterior glottic web formation (Fig. 26.1) can occur from either congenital or acquired causes. A congenital anterior glottic web is quite rare, and the symptoms are usually identified at birth or in a young child if the web is large, causing stridorous breathing. Smaller congenital webs are often identified later in life and are associated with exercise restriction and/or dysphonia. Acquired anterior glottic webs are the most common type of glottic web, and these typically occur from a traumatic injury to the larynx, be it surgical, iatrogenic, external trauma, or intubation related. Anterior glottic webs range in size from being extremely small (a microweb) to encompassing the entire length of the membranous vocal folds. Obviously, the symptoms, severity, and surgical procedures will vary significantly based on the etiology and size of the web.
Anterior glottic webs should be evaluated in two specific dimensions: from an anterior–posterior dimension and in a
superior–inferior plane. The latter can often involve web formation from the glottis to the supraglottis and/or web formation from the glottis into the subglottis.
A variety of conditions are associated with anterior glottic webs; specifically, laryngeal framework stenosis should be carefully examined and considered when evaluating a patient with an anterior glottic web. This can involve supraglottic stenosis, thyroid cartilage constriction resulting in glottic stenosis, and subglottic stenosis from cricoid cartilage deformation and loss of normal dimensions, specifically in the anterior–posterior plane.
Vocal fold scar is frequently associated with an anterior glottic web because of the traumatic nature of the etiology of most of these conditions.
Differential diagnosis for an anterior glottic web is:
■Wegner’s granulomatosis
■Sarcoidosis
■Amyloidosis
26.3Surgical Indications and Contraindications
Indications include:
■Airway restriction
■Abnormally elevated phonatory pitch
■Dysphonia
Contraindications include:
■No functional voice limitations and no airway restriction
■Uncontrolled LPR
■Active RRP without any airway restriction
26.4Surgical Equipment
Equipment needed includes:
■Standard phonomicrosurgery set (see Chap 10, Table 10.1)
■Standard laser microlaryngoscopy set (see Chap. 13)
■Silastic sheet and/or premade laryngeal keel
Fig. 26.1 Anterior glottic web
160 |
Anterior Glottic Web |
■Endo-extra laryngeal needle passer (Richard Wolf Medical, Knittingen, Germany) or 18-g angiocatheter/2-cm 18-g needle (Fig 27.7)
■0 Prolene suture
■Silicone surgical button(s)
■Mitomycin C (optional)
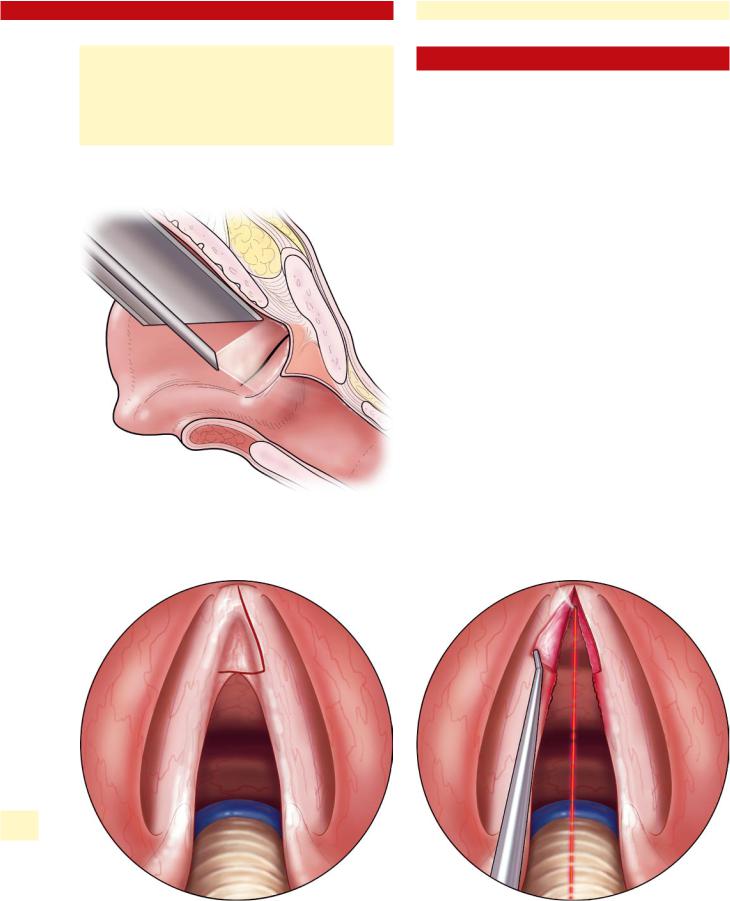
Fig. 26.2 Endoscopic assessment of superior–inferior extent of glottic web
26.5Surgical Procedure
The two approaches most often used for the release and removal of an anterior glottic web are endoscopic flap or endoscopic placement of a keel. The endoscopic flap approach is best used for smaller anterior glottic webs and involves the asymmetric division of the anterior glottic web, with utilization of the web for mucosal coverage on one side of the anterior commissure. This operation involves delicate surgical handling. Elevation and preservation of the anterior glottic web mucosa is performed, and then the flap is sutured over one side of the anterior commissure.
For larger anterior glottic webs and for patients that do not have adequate tissue for an endoscopic flap, release of the anterior glottic web and endoscopic placement of a keel is required. Patients undergoing this procedure need to be informed of the need for two surgical procedures (placement of keel and removal of keel.) They also need to be prepared for moderate pain and discomfort as well as globus sensation for the 7- to 10-day period that the keel is in position.
1.Endoscopic flap for anterior glottic web
a)Laryngoscopic exposure of the anterior glottic web and the anterior commissure region with suspension laryngoscopy (see Chap. 10, “Principles of Phonomicrosurgery”)
b)Visualize and assess superior and inferior depth of anterior glottic web and plan incision location(s) using angled telescopes (Fig. 26.2).
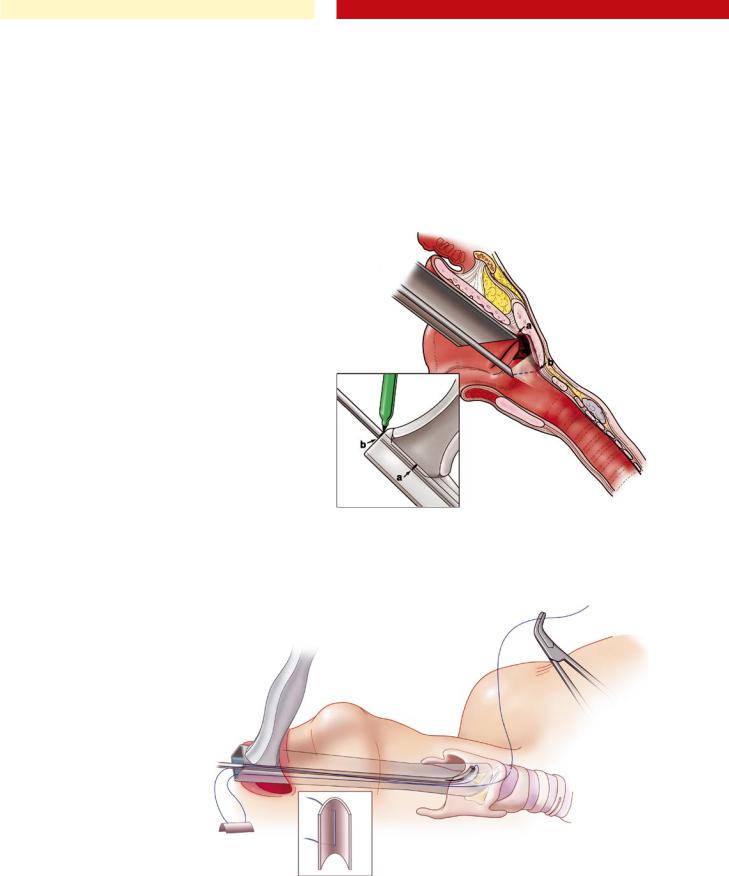
c)Incise the anterior glottic web in an asymmetric fashion at either the free edge of the vocal fold or onto the superior surface of the vocal fold that will then be incorporated into the flap (Fig. 26.3).
26
Fig. 26.3 Incision for asymmetric division of anterior glottic web |
Fig. 26.4 Elevation of the anterior glottic web flap and release of web/ |
|
scar up to inner aspect of the thyroid cartilage |
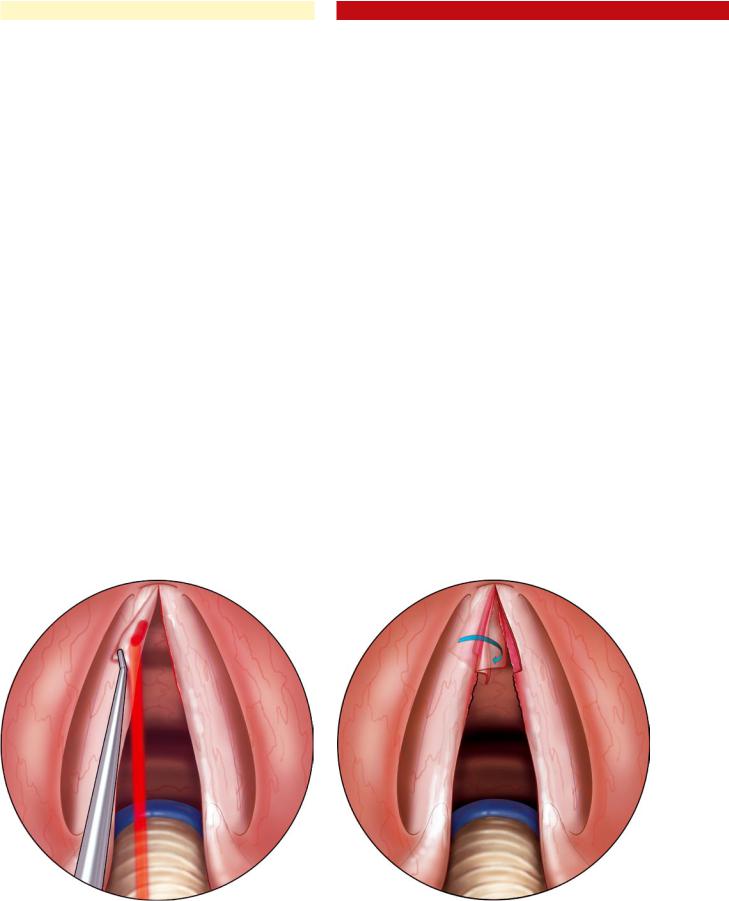
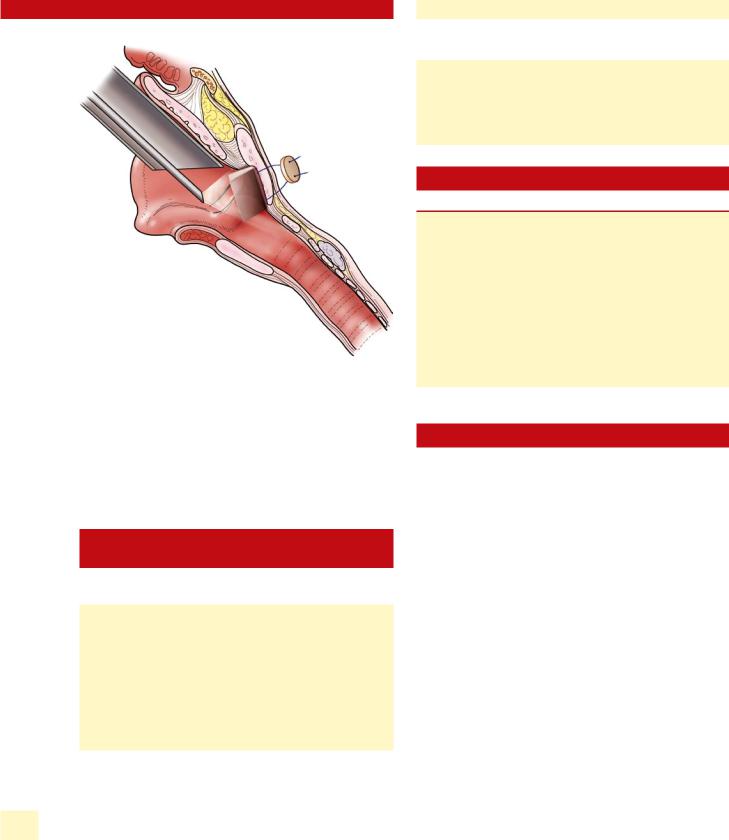
d)Preservation of flap mucosa, complete release of the anterior glottic web all the way up to the anterior commissure/thyroid cartilage is then performed using cold-steel instrumentation or the CO2 laser (Fig 26.4).
e)Often demucosalization of the undersurface of the flap and the subglottis in the region of the anterior commissure and anterior third of the vocal fold is then required.
It can be done with either cold steel or a CO2 laser using a defocused beam on low-power settings (Fig. 26.5).
f)The endoscopic flap can now be draped down into the subglottis and secured in place with a single 5.0 or 6.0 absorbable suture. It is a rare endoscopic flap that does not need suturing to stay in the proper location. Tissue glue has not been adequate, in the authors’ past experience, to secure the endoscopic flap into location (Figs. 26.6. 26.7).
g)The application of mitomycin C onto the contralateral anterior commissure and anterior third of the vocal fold in the demucosalized area is optional (see Chap. 29).
2.Release of the anterior glottic web with endoscopic keel placement
a)Suspend the laryngoscope with adequate false vocal fold retraction and complete exposure of the anterior glottic web and anterior commissure. It is important to suspend the laryngoscope with adequate space above the anterior commissure for placement of the superior position of the planned keel (approximately 3–4 mm above the level of the glottis).
b)Visualize the anterior glottic web with 30 and 70° telescopes. During this visualization it is important to evaluate the web in a cephalocaudal dimension given that this will determine the minimum length of the planned keel (Fig. 26.2).
Fig. 26.5 Demucosalization of the undersurface of the flap
Chapter 26 |
161 |
c)Release or excision of the anterior glottic web can be
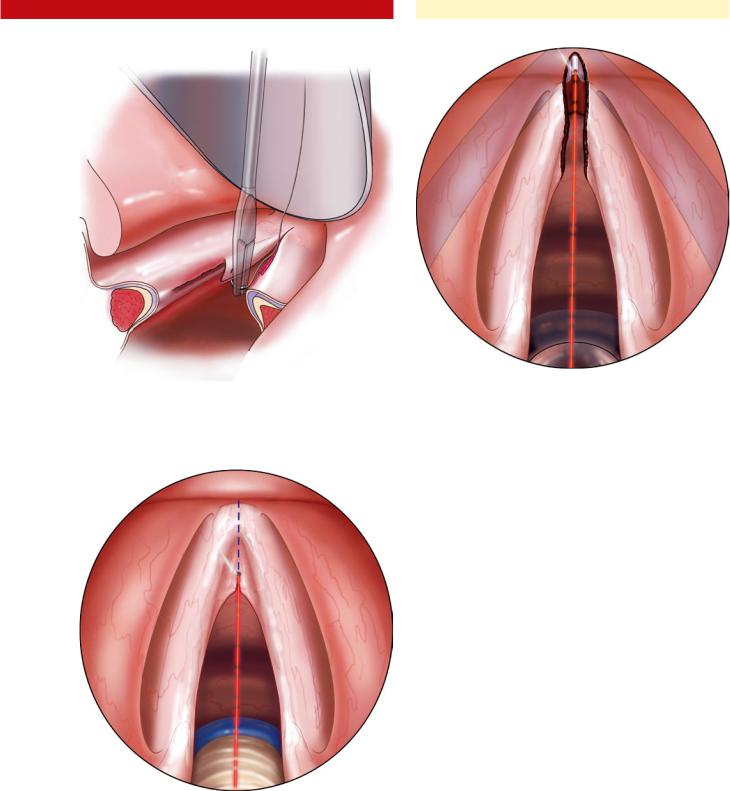
done either with a CO2 laser (smallest spot size and low power) or with straight-up scissors and/or a sickle knife. When incising the anterior glottic web, it is important to put tension on the vocal folds with lateral retraction and stay in the midline between the two vocal folds to minimize any further lamina propria damage. Cold-steel excision is preferable to minimize laser surgery-related scar formation (Fig. 26.8).
d)After excision or release of the anterior glottic web up to
the anterior commissure, the CO2 laser can then be used to make an approximately 1-mm deep groove into the inner aspect of the thyroid cartilage, extending 3–4 mm above the anterior commissure and 4–5 mm below the anterior commissure. This groove will be used for placement of the keel in an anterior-most location (Fig. 26.9).
e)Thirty and 70° telescopes can then be used to visualize the superior and inferior extent of the anterior glottic web release and determine the superior–inferior extent of the intended keel. When visualizing this area with a 30 or 70° telescope, the telescope should be passed to the superior-most location to which the keel will need to be secured, and then the telescope shaft can be marked at the location of the junction of the shaft and the proximal laryngoscope. The 30° telescope is then moved to the inferior limit of the planned keel location. The telescope is held at this position; a mark on the telescope shaft can be placed at the junction of the shaft and the proximal laryngoscope. The distance between the two marks on the telescope shaft is measured and this distance will be used to determine the superior–inferior length of the keel (Fig. 26.10).
Fig. 26.6 Inferior reflection of flap to cover one side of the anterior commissure
162 |
Anterior Glottic Web |
Fig. 26.7 Securing the endoscopic flap with suture placement
26 |
Fig. 26.8 Midline division of the anterior glottic web down to inner |
|
aspect of the thyroid cartilage |
|
Fig. 26.9 CO2 laser vaporization of a 1-mm thyroid cartilage groove at the anterior commissure
f)After trimming the keel to the required superior–infe- rior dimension as well as the anterior–posterior dimension, the keel can be placed with a heavy cup forceps into the larynx to evaluate the appropriate size and fit.
g)A 0 Prolene suture can then be passed from the subglottis to the anterior neck with the Lichtenberger endo-ex- tralaryngeal needle passer. This can be done with microlaryngoscopy or endoscopically with a 30° telescope. A clamp should be placed on the free end of the suture that comes out of the anterior neck (Fig. 26.11).
Alternative Method
i.Have an assistant pass an 18-g angiocatheter or 2.5- cm needle from the anterior neck to the desired location in the anterior subglottis during simultaneous microlaryngoscopy or telescopic visualization of the larynx. Once the needle is in the proper location into the subglottis, then a 0 Prolene suture can be passed in through the tip of needle and out through the neck where it is secured with a clamp.
h)Pass the free end of the suture through the laryngoscope. Secure the keel at two locations along the spine of the keel with the suture. The placement of the suture through the keel will ultimately determine the exact location of the keel in the larynx. Thus, it is helpful to place the keel into the appropriate location and obtain endoscopic visualization with the 70° telescope of where the fixation sutures should be placed onto the keel.
i)Load the suture coming from the keel into the endo-ex- tra laryngeal needle passer and place down the laryngoscope to pass the suture from the region superior to the anterior commissure to the anterior neck (Fig. 26.11).
|
Chapter 26 |
163 |
Alternative Method
i.After passing the suture through the keel, place the 18-g angiocatheter or 2.5-cm needle through the anterior neck into a location above the anterior commissure with simultaneous microlaryngoscopy or telescopic visualization.
ii.Pass a 0 Prolene suture into the shaft of the angiocatheter/needle until an assistant can see the suture emerging from the angiocatheter. The assistant can then remove the angiocatheter or needle and clamp the suture that has been passed from the larynx to the anterior neck.
superior portion of the keel. A large cup forceps is then used to grasp the keel. Once the endoscopist is confident that he has a firm grasp of the keel, the anterior neck sutures can be cut and the keel can then be removed via the laryngoscope.
c)After adequate mask ventilation of the patient, a repeat direct laryngoscopy and endoscopic visualization of the operative site is performed. If there is severe granulation tissue or a reformation of the anterior glottic web, then the endoscopic glottic web procedure can be repeated.
j)Guide the keel into position in the endolarynx as an assistant applies equal tension to the sutures coming out of the anterior neck.
k)Place a moderate and equal amount of tension on the two sutures coming out of the anterior neck and confirm the proper location of the keel using 30 and 70° telescopic visualization.
l)If the keel is not in the proper location from either a superior, inferior, or lateral perspective, then the passing of the sutures and placement of the sutures through the keel should be repeated.
m)Secure the endoscopic keel in place by tying the sutures coming out of the anterior neck over surgical buttons with a simultaneous visualization of the keel during the suture tying procedure (Fig. 26.12).
3.Keel removal (10–14 days post-placement)
a)Apneic anesthesia is the preferred method of anesthesia for this procedure, given that endotracheal intubation can complicate the endoscopic keel removal and injure the operative site.
b)Direct laryngoscopy is then performed, and a 0° tele- Fig. 26.10 30° telescope is used to measure the length of the keel from
scope is used to visualize the endolarynx, specifically the |
superior to inferior |
Fig. 26.11 Passing inferior fixation suture from endolarynx through the anterior neck and placement of suture through keel
164 |
Anterior Glottic Web |
Fig. 26.12 Visualization of proper placement of the keel with 30 and 70° telescopes, with keel secured together over button on the neck
Also at this juncture, if indicated, mitomycin C can be applied at the operative site. These decisions are made based on the amount of mucosalization that has occurred at the anterior glottis.
26.6Postoperative Care and Complications
Postoperative care includes:
■Intravenous antibiotics (perioperatively only)
■Intravenous steroids perioperatively
■Laryngopharyngeal reflux disease treatment
■Pain medicine as needed
■Overnight observation in the hospital
■Reevaluation of the patient in approximately 8–10 days in the office with flexible laryngoscopy or indirect laryngoscopy to determine the amount of mucosalization that has occurred underneath the keel
Complications comprise:
■Anterior glottic web reformation
■Dislodgement of keel
■Scar or erosion of the vocal fold from malposition of the keel
■Granulation at the keel suture location
Key Points
■Anterior glottic web most commonly is an acquired condition from surgical trauma.
■Anterior glottic web surgery is indicated for airway restriction or symptomatic dysphonia.
■Endoscopic flap release of anterior glottic web can be done successfully with good laryngeal exposure and a small glottic web.
■Release of anterior glottic web and placement of endoscopic keel requires skill from the surgeon and can be successfully performed if attention to technical details are observed.
Selected Bibliography
1Benninger MS, Jacobson B. Vocal nodules, microwebs and surgery (1997) J Voice 11:238–246
2Casiano RR, Lundy DS (1998) Outpatient transoral laser vaporization of anterior glottic webs and keel placement: risks of airway compromise. J Voice 12:536–539
3Dedo HH (1979) Endoscopic Teflon keel for anterior glottic web. Ann Otol Rhinol Laryngol 88(Pt. 1):467–473
4Ford CN, Bless DM, Campos G, Leddy M (1994) Anterior commissure microwebs associated with vocal nodules: detection, prevalence, and significance. Laryngoscope 104(Pt 1.):1369–1375
5HsiaoTY(1999)Combinedendolaryngealandexternalapproaches for iatrogenic glottic web. Laryngoscope 109:1347–1350
6Liyanage SH, Khemani S, Lloyd S, Farrell R (2006) Simple keel fixation technique for endoscopic repair of anterior glottic stenosis. J Laryngol Otol 120:322–324
7Milczuk HA, Smith JD, Everts EC (2000) Congenital laryngeal webs: surgical management and clinical embryology. Int J Pediatr Otorhinolaryngol 52:1–9
8Schweinfurth J (2002) Single-stage, stentless endoscopic repair of anterior glottic webs. Laryngoscope 112:933–935
26
Part B Phonomicrosurgery
for Benign Laryngeal
Pathology
IIILaser Microlaryngeal Surgery (Airway/ Neoplastic Conditions)
Chapter 27
Bilateral Vocal Fold Paralysis |
27 |
|
27.1Fundamental and Related Chapters
Please see Chaps. 3, 5, 9, 10, 13, and 28 for further information.
27.2Disease Characteristics and Differential Diagnosis
Patients with bilateral vocal fold paralysis (BVFP) generally fall into two categories, (1) iatrogenic recurrent laryngeal nerve injury (typically from a thyroidectomy), or (2) progressive neurological disorder (Shy-Drager Syndrome, syringomelia, Guillian-Barré syndrome, etc.). In contrast to unilateral vocal fold paralysis, with which the patient principally complains of voice and swallowing difficulties, bilateral vocal fold paralysis (BVFP) causes airway restriction and not vocal dysfunction. In patients with BVFP, treatment is directed at maximizing the airway, while attempting to limit the negative effects of treatment on vocal function.
It can be difficult to distinguish BVFP from posterior glottic stenosis. In some ways, the distinction is not essential, because posterior transverse cordotomy and/or partial arytenoidectomy are often effective for both conditions. However, a correct diagnosis greatly facilitates patient counseling and appropriate treatment, therefore a careful examination to evaluate cricoarytenoid joint fixation and posterior glottic stenosis should be carried out prior to surgical intervention (see Chap. 28, “Posterior Glottic Stenosis”).
The most reasonable approach to patients with bilateral vocal fold paralysis is a step-wise approach to enlarge the glottic airway. The least aggressive and safest procedures are the posterior transverse cordotomy (PTC) or medial arytenoidectomy (MA). After these procedures, an extended version of either (or a combination) can be performed, or a total arytenoidectomy. Please note the procedure historically called a total arytenoidectomy does not involve complete anatomic removal of the arytenoid cartilage. Its aim is to remove all arytenoid cartilage that effects the airway. Selection of the side to perform surgery for bilateral vocal fold paralysis is based on a variety of factors. The most important factor for selection is presence of any purposeful motion either adductory or abductory. If there is no motion of either vocal fold, then laryngeal electromyography can assist in determining which side has the worst neuromuscular status and thus is the best location for the surgical procedure. In addition to these methods, palpa-
tion of the cricoarytenoid joint as described below is helpful to determine which cricoarytenoid joint has the worst range of motion and mobility and would then be best choice for surgical procedure to widen the posterior glottic airway.
27.3Surgical Indication and Contraindications
An indication for surgery is symptomatic airway obstruction. Contraindications to treatment of BVFP include:
■Rapidly progressive neurologic disorder
■Unrealistic patient expectations (improvement in both airway and voice)
Relative contraindications to treatment include:
■Presence of aspiration
■Compromised pulmonary status
■Diabetes (more true for open procedures than endoscopic)
■Previous radiation therapy to the neck/larynx
Treatment options for BVFP include:
■Tracheotomy
■Microlaryngoscopy with laser posterior transverse cordotomy
■Microlaryngoscopy with laser medial arytenoidectomy
■Microlaryngoscopy with laser total arytenoidectomy
■Endoscopic suture lateralization
■Open arytenoidectomy
In general, rapidly progressive neurologic disorders (such as Shy–Drager) tend to be treated with tracheotomy, due to comorbid conditions. However, most other causes of BVFP can be treated more conservatively with endoscopic techniques. Posterior transverse cordotomy or medial arytenoidectomy are generally the ideal endoscopic treatment options, because voice results tend to be better, and aspiration is less likely, as compared with total arytenoidectomy. Endoscopic suture lateralization is useful if temporary treatment is warranted. Open arytenoidectomy is reserved for cases where endoscopic techniques have failed or are impossible due to anatomic limitations, and thus is rarely required.

168 |
Bilateral Vocal Fold Paralysis |
27.4Surgical Equipment
Equipment includes:
■Laser microlaryngoscopy equipment (Chap. 13)
■Laryngeal bipolar/monopolar cautery (not essential)
■Mitomycin C (0.4 mg/ml)
■Also for suture lateralization only:
■Endo-extralarnygeal needle carrier by Lichtenberger (Richard Wolf Medical, Knittingen, Germany)
■Silicone buttons
■0 or 2.0 Prolene sutures
27.5Surgical Procedure
1.Palpation of cricoarytenoid joint
Direct laryngoscopy should be performed. It is best to perform cricoarytenoid joint palpation without an endotracheal tube in place. Anesthesia should induce complete muscle paralysis and the posterior larynx is viewed with microlaryngoscopy or a 0° endoscope. Care should be taken to ensure that suspended laryngoscope is positioned cephalad in the larynx to avoid the laryngoscope limiting the range of motion of the arytenoid cartilages. Palpation of the cricoarytenoid joint is performed by using a sturdy instrument such as a large cup forceps and placing it adjacent to the vocal process and pushing the vocal process laterally swiftly. With this maneuver, the surgeon can gauge the degree of effort required to displace laterally the vocal process as well as the speed of the recoil of the tissue in a medial direction
(Figs. 27.1, 27.2). During this maneuver, careful evaluation of the posterior commissure should be done. If the entire posterior commissure moves with lateralization of the vocal process, then this suggests that posterior glottic stenosis may be present. This same procedure should be done on the contralateral side and used to compare the degree of stiffness and range of motion of both cricoarytenoid joints. This maneuver can be helpful in selecting which side is optimal for surgery to improve the posterior glottic airway. One should select the arytenoid with the worst cricoarytenoid joint mechanics to operate on.
2.Posterior transverse cordotomy
a)Intubation with 5.0 or 5.5 laser safe endotracheal tube (ETT)
Alternately, a subglottic jet catheter (Hunsaker tube, Medtronic Xomed, Jacksonville, Fla.) can be used.
b)Expose larynx with laryngoscope and place into suspension.
i.Ensure that the ETT is in posterior commissure, and that there is still good vocal process visualization with the ETT in a posterior position. If the ETT obstructs the surgical site, then the EET can be moved anteriorly with the laryngoscope securing the ETT anteriorly (see Chap. 19, “Vocal Fold Granuloma”).
ii.It is often helpful to angle the laryngoscope toward the side where the cordotomy is being performed to maximize the exposure of the lateral aspect of the true vocal fold/false vocal fold (see Chap. 19, Fig. 19.2).
c)Laser precautions are implemented (see Chap. 13, “Principles of Laser Microlaryngoscopy”).
d)Laser incision
27
Fig. 27.1 Palpation of a mobile (nonfixed) cricoarytenoid joint: lateral displacement of arytenoid with blunt instrument
Fig. 27.2 Release of arytenoid, resulting in recoil of arytenoid medially. This would be observed in a patient with BVFP