

Книги фарма 2 / Bertram G. Katzung-Basic & Clinical Pharmacology(9th Edition)
.pdfThe normal thyroid gland secretes sufficient amounts of the thyroid hormones—triiodothyronine (T3) and tetraiodothyronine (T4, thyroxine)—to normalize growth and development, body temperature, and energy levels. These hormones contain 59% and 65% (respectively) of iodine as an essential part of the molecule. Calcitonin, the second type of thyroid hormone, is important in the regulation of calcium metabolism and is discussed in Chapter 42: Agents That Affect Bone Mineral Homeostasis.
Iodide Metabolism
The recommended daily adult iodide (I–)* intake is 150 g (200 g during pregnancy).
* In this chapter, the term "iodine" denotes all forms of the element; the term "iodide" denotes only the ionic form, I–.
Iodide, ingested from food, water, or medication, is rapidly absorbed and enters an extracellular fluid pool. The thyroid gland removes about 75 
 g a day from this pool for hormone secretion, and the balance is excreted in the urine. If iodide intake is increased, the fractional iodine uptake by the thyroid is diminished.
g a day from this pool for hormone secretion, and the balance is excreted in the urine. If iodide intake is increased, the fractional iodine uptake by the thyroid is diminished.
Biosynthesis of Thyroid Hormones
Once taken up by the thyroid gland, iodide undergoes a series of enzymatic reactions that convert it into active thyroid hormone (Figure 38–1). The first step is the transport of iodide into the thyroid gland by an intrinsic follicle cell basement membrane protein called the sodium/iodide symporter (NIS). This can be inhibited by such anions as SCN–, TcO4–, and ClO4–. Iodide is then oxidized by thyroidal peroxidase to iodine, in which form it rapidly iodinates tyrosine residues within the thyroglobulin molecule to form monoiodotyrosine (MIT) and diiodotyrosine (DIT). This process is called iodide organification. Thyroidal peroxidase is transiently blocked by high levels of intrathyroidal iodide and blocked more persistently by thioamide drugs. Two molecules of DIT combine within the thyroglobulin molecule to form L-thyroxine (T4). One molecule of MIT and one molecule of DIT combine to form T3. In addition to thyroglobulin, other proteins within the gland may be iodinated, but these iodoproteins do not have hormonal activity. Thyroxine, T3, MIT, and DIT are released from thyroglobulin by exocytosis and proteolysis of thyroglobulin at the apical colloid border. The MIT and DIT are deiodinated within the gland, and the iodine is reutilized. This process of proteolysis is also blocked by high levels of intrathyroidal iodide. The ratio of T4 to T3 within thyroglobulin is approximately 5:1, so that most of the hormone released is thyroxine. Most of the T3 circulating in the blood is derived from peripheral metabolism of thyroxine (see below).
Figure 38–1.
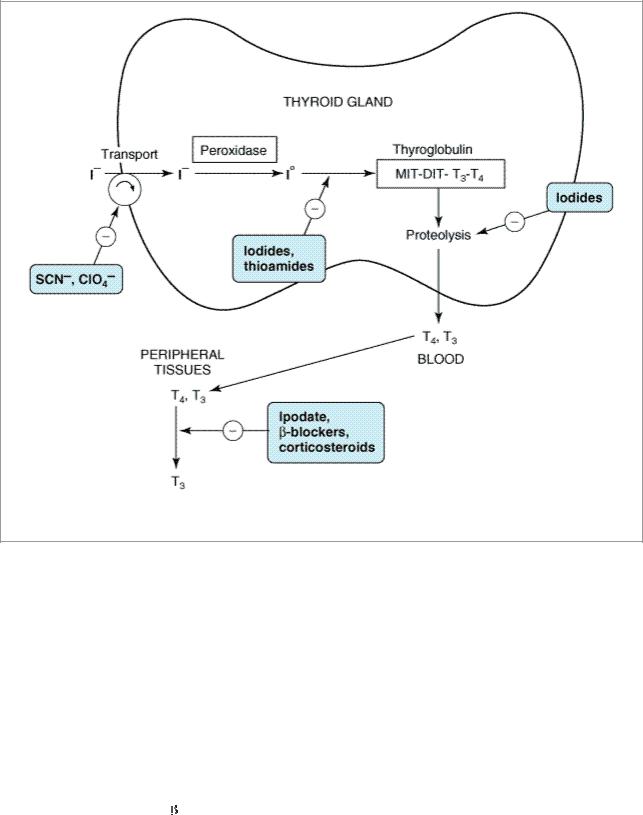
Biosynthesis of thyroid hormones. The sites of action of various drugs that interfere with thyroid hormone biosynthesis are shown.
Transport of Thyroid Hormones
T4 and T3 in plasma are reversibly bound to protein, primarily thyroxine-binding globulin (TBG). Only about 0.04% of total T4 and 0.4% of T3 exist in the free form. Many physiologic and pathologic states and drugs affect T4, T3, and thyroid transport. However, the actual levels of free hormone generally remain normal, reflecting feedback control.
Peripheral Metabolism of Thyroid Hormones
The primary pathway for the peripheral metabolism of thyroxine is deiodination. Deiodination of T4 may occur by monodeiodination of the outer ring, producing 3,5,3'-triiodothyronine (T3), which is three to four times more potent than T4. Alternatively, deiodination may occur in the inner ring, producing 3,3',5'-triiodothyronine (reverse T3, or rT3), which is metabolically inactive (Figure 38– 2). Drugs such as ipodate, 
 -blockers, and corticosteroids, and severe illness or starvation inhibit the 5'-deiodinase necessary for the conversion of T4 to T3, resulting in low T3 and high rT3 levels in the serum. Normal levels of thyroid hormone in the serum are listed in Table 38–1. The low serum levels of T3 and rT3 in normal individuals are due to the high metabolic clearances of these two compounds.
-blockers, and corticosteroids, and severe illness or starvation inhibit the 5'-deiodinase necessary for the conversion of T4 to T3, resulting in low T3 and high rT3 levels in the serum. Normal levels of thyroid hormone in the serum are listed in Table 38–1. The low serum levels of T3 and rT3 in normal individuals are due to the high metabolic clearances of these two compounds.

Figure 38–2.
Peripheral metabolism of thyroxine. (Modified from Greenspan FS: The Thyroid Gland. In: Greenspan FS, Gardner D [editors]: Basic &Clinical Endocrinology, 6th ed. McGraw-Hill, 2001.)
Table 38–1. Summary of Thyroid Hormone Kinetics.
Variable |
T4 |
T3 |
|
|
|
|
|
|
Volume of distribution |
10 L |
40 L |
|
|
|
Extrathyroidal pool |
800 g |
54 g |
|
|
|
Daily production |
75 g |
25 g |
|
|
|
Fractional turnover per day |
10% |
60% |
|
|
|
Metabolic clearance per day |
1.1 L |
24 L |
|
|
|
Half-life (biologic) |
7 days |
1 day |
|
|
|
Serum levels |
|
|
|
|
|
Total |
5–11 g/dL |
95–190 ng/dL |
|
(64–132 nmol/L) |
(1.5–2.9 nmol/L) |
|
|
|
Free |
0.7–1.86 ng/dL |
0.2–0.52 ng/dL |
|
(9–24 pmol/L) |
(3–8 pmol/L) |
|
|
|
Amount bound |
99.96% |
99.6% |
|
|
|
Biologic potency |
1 |
4 |
|
|
|

Oral absorption |
80% |
95% |
|
|
|
Control of Thyroid Function
The tests used to evaluate thyroid function are listed in Table 38–2.
Table 38–2. Normal Values for Thyroid Function Tests.
Name of Test |
Normal Value1 |
Results in |
Results in |
|
|
Hypothyroidism |
Hyperthyroidism |
|
|
|
|
Total thyroxine by RIA |
5–12 g/dL (64–154 |
Low |
High |
(T4 [RIA]) |
nmol/L) |
|
|
|
|
|
|
|
|
|
|
Total triiodothyronine |
70–132 ng/dL (1.1–2.0 |
Normal or low |
High |
by RIA (T3 [RIA]) |
nmol/L) |
|
|
|
|
|
|
|
|
|
|
Resin T3 uptake (RT3U) |
25–35% |
Low |
High |
|
|
|
|
|
|
|
|
Free thyroxine index |
1.3–4.2 |
Low |
High |
(FT4I)1 |
|
|
|
|
|
|
|
|
|
|
|
Free T3 index (FT3I) |
17.5–46 |
Normal or low |
High |
|
|
|
|
|
|
|
|
Free FT4 (FT4) |
0.7–1.86 (9–24 pmol/L) |
Low |
High |
|
|
|
|
|
|
|
|
Free T3 (FT3) |
0.2–0.42 ng/dL (3–8 |
Low |
High |
|
pmol/L) |
|
|
|
|
|
|
Thyrotropic hormone |
0.5–5.0 IU/mL (0.5–5.0 |
High2 |
Low |
(TSH) |
mIU/L) |
|
|
|
|
|
|
123I uptake at 24 hours |
5–35% |
Low |
High |
|
|
|
|
|
|
|
|
Thyroglobulin |
< 1 IU/mL |
Often present |
Usually present |
autoantibodies (Tg-ab) |
|
|
|
|
|
|
|
Thyroid peroxidase |
< 1 IU/mL |
Often present |
Usually present |
antibodies (TPA) |
|
|
|
|
|
|
|
Isotope scan with 123I or |
Normal pattern |
Test not indicated |
Diffusely enlarged |
99mTcO4 |
|
|
gland |
|
|
|
|
|
|
|
|
Fine-needle aspiration |
Normal pattern |
Test not indicated |
Test not indicated |
biopsy (FNA) |
|
|
|
|
|
|
|
Serum thyroglobulin |
< 40 ng/mL |
Test not indicated |
Test not indicated |
|
|
|
|
Serum calcitonin |
Male: < 8 ng/L (< 2.3 |
Test not indicated |
Test not indicated |
|
|
|
|

pmol/L); female: < 4 ng/L (< 1.17 pmol/L)
1Results may vary with different laboratories.
2Exception is central hypothyroidism
Thyroid-Pituitary Relationships
Control of thyroid function via thyroid-pituitary feedback is also discussed in Chapter 37: Hypothalamic & Pituitary Hormones. Briefly, hypothalamic cells secrete thyrotropin-releasing hormone (TRH) (Figure 38–3). TRH is secreted into capillaries of the pituitary portal venous system, and in the pituitary gland, TRH stimulates the synthesis and release of thyroid-stimulating hormone (TSH). TSH in turn stimulates an adenylyl cyclase–mediated mechanism in the thyroid cell to increase the synthesis and release of T4 and T3. These thyroid hormones act in a negative feedback fashion in the pituitary to block the action of TRH and in the hypothalamus to inhibit the synthesis and secretion of TRH. Other hormones or drugs may also affect the release of TRH or TSH.
Figure 38–3.

The hypothalamic-pituitary-thyroid axis. Acute psychosis or prolonged exposure to cold may activate the axis. Hypothalamic TRH stimulates pituitary TSH release, while somatostatin and dopamine inhibit it. TSH stimulates T4 and T3 synthesis and release from the thyroid, and they in turn inhibit both TRH and TSH synthesis and release. Small amounts of iodide are necessary for hormone production, but large amounts inhibit T3 and T4 production and release. (Solid arrows, stimulatory influence; dashed arrows, inhibitory influence. H, hypothalamus, HP, anterior pituitary.)
Autoregulation of the Thyroid Gland
The thyroid gland also regulates its uptake of iodide and thyroid hormone synthesis by intrathyroidal mechanisms that are independent of TSH. These mechanisms are primarily related to the level of iodine in the blood. Large doses of iodine inhibit iodide organification (Figure 38–1). In certain disease states (eg, Hashimoto's thyroiditis), this can result in inhibition of thyroid hormone synthesis and hypothyroidism.
Abnormal Thyroid Stimulators
In Graves' disease (see below), lymphocytes secrete a TSH receptor-stimulating antibody (TSH-R Ab [stim]), also known as thyroid-stimulating immunoglobulin (TSI). This immunoglobulin binds to the TSH receptor and turns on the gland in the same fashion as TSH itself. The duration of its effect, however, is much longer than that of TSH. TSH receptors are also found in orbital fibrocytes, which may be stimulated by high levels of TSH-R Ab [stim].
Katzung PHARMACOLOGY, 9e > Section VII. Endocrine Drugs > Chapter 38. Thyroid & Antithyroid Drugs >
Basic Pharmacology of Thyroid & Antithyroid Drugs
Thyroid Hormones
Chemistry
The structural formulas of thyroxine and triiodothyronine as well as reverse triiodothyronine (rT3) are shown in Figure 38–2. All of these naturally occurring molecules are levo (L) isomers. The synthetic dextro (D) isomer of thyroxine, dextrothyroxine, has approximately 4% of the biologic activity of the L isomer as evidenced by its lesser ability to suppress TSH secretion and correct hypothyroidism.
Pharmacokinetics
Thyroxine is absorbed best in the duodenum and ileum; absorption is modified by intraluminal factors such as food, drugs, and intestinal flora. Oral bioavailability of current preparations of L- thyroxine averages 80% (Table 38–1). In contrast, T3 is almost completely absorbed (95%). T4 and T3 absorption appears not to be affected by mild hypothyroidism but may be impaired in severe myxedema with ileus. These factors are important in switching from oral to parenteral therapy. For parenteral use, the intravenous route is preferred for both hormones.
In patients with hyperthyroidism, the metabolic clearances of T4 and T3 are increased and the halflives decreased; the opposite is true in patients with hypothyroidism. Drugs that induce hepatic

microsomal enzymes (eg, rifampin, phenobarbital, carbamazepine, phenytoin) increase the metabolism of both T4 and T3 (Table 38–3). Despite this change in clearance, the normal hormone concentration is maintained in euthyroid patients as a result of compensatory hyperfunction of the thyroid. However, patients receiving T4 replacement medication may require increased dosages to maintain clinical effectiveness. A similar compensation occurs if binding sites are altered. If TBG sites are increased by pregnancy, estrogens, or oral contraceptives, there is an initial shift of hormone from the free to the bound state and a decrease in its rate of elimination until the normal hormone concentration is restored. Thus, the concentration of total and bound hormone will increase, but the concentration of free hormone and the steady state elimination will remain normal. The reverse occurs when thyroid binding sites are decreased.
Table 38–3. Drug Effects and Thyroid Function.
Drug Effect |
Drugs |
|
|
Change in thyroid hormone synthesis |
|
|
|
Inhibition of TRH or TSH secretion without |
Dopamine, levodopa, corticosteroids, |
induction of hypothyroidism |
somatostatin |
|
|
Inhibition of thyroid hormone synthesis or |
Iodides (including amiodarone), lithium, |
release with the induction of hypothyroidism (or |
aminoglutethimide |
occasionally hyperthyroidism) |
|
|
|
Alteration of thyroid hormone transport and |
|
serum total T3 and T4 levels, but usually no |
|
modification of FT4 or TSH |
|
|
|
|
|
Increased TBG |
Estrogens, tamoxifen, heroin, methadone, |
|
mitotane |
|
|
Decreased TBG |
Androgens, glucocorticoids |
|
|
Displacement of T3 and T4 from TBG with |
Salicylates, fenclofenac, mefenamic acid, |
transient hyperthyroxinemia |
furosemide |
|
|
|
|
Alteration of T4 and T3 metabolism with |
|
modified serum T3 and T4 levels but not FT4 |
|
or TSH levels |
|
|
|
|
|
Induction of increased hepatic enzyme activity |
Phenytoin, carbamazepine, phenobarbital, |
|
rifampin, rifabutin |
|
|
Inhibition of 5'-deiodinase with decreased T3, |
Iopanoic acid, ipodate, amiodarone, -blockers, |
increased rT3 |
corticosteroids, propylthiouracil |
|
|
|
|
Other interactions |
|
|
|
Interference with T4 absorption |
Cholestyramine, colestipol, aluminum |
|
hydroxide, sucralfate, reloxifene, ferrous |
|
sulfate, some calcium preparations, bran |
|
|
Induction of autoimmune thyroid disease with |
Interferon- , interleukin-2 |
hypothyroidism or hyperthyroidism |
|
|
|

Mechanism of Action
A model of thyroid hormone action is depicted in Figure 38–4, which shows the free forms of thyroid hormones, T4 and T3, dissociated from thyroid-binding proteins, entering the cell by diffusion or possibly by active transport. Within the cell, T4 is converted to T3 by 5'-deiodinase, and the T3 enters the nucleus, where T3 binds to a specific T3 receptor protein, a member of the c-erb oncogene family, which also includes the steroid hormone receptors and receptors for vitamins A and D. The T3 receptor exists in two forms, 
 and
and 
 . Differing concentrations of receptor forms in different tissues may account for variations in T3 effect on different tissues.
. Differing concentrations of receptor forms in different tissues may account for variations in T3 effect on different tissues.
Figure 38–4.
Regulation of transcription by thyroid hormones. T3 and T4 are triiodothyronine and thyroxine, respectively. PB, plasma binding protein; F, transcription factor; R, receptor; PP, proteins that bind at the proximal promoter. (Reproduced, with permission, from Baxter JD: General concepts of endocrinology. In: Greenspan FS, Baxter JD (editors). Basic & Clinical Endocrinology, 4th ed. Originally published by Appleton & Lange. Copyright © 1994 by The McGraw-Hill Companies, Inc.)
Most of the effects of thyroid on metabolic processes appear to be mediated by activation of nuclear receptors that lead to increased formation of RNA and subsequent protein synthesis, eg, increased formation of Na+/K+ ATPase. This is consistent with the observation that the action of thyroid is manifested in vivo with a time lag of hours or days after its administration.
Large numbers of thyroid hormone receptors are found in the most hormone-responsive tissues

(pituitary, liver, kidney, heart, skeletal muscle, lung, and intestine), while few receptor sites occur in hormone-unresponsive tissues (spleen, testes). The brain, which lacks an anabolic response to T3, contains an intermediate number of receptors. In congruence with their biologic potencies, the affinity of the receptor site for T4 is about ten times lower than that for T3. The number of nuclear receptors may be altered to preserve body homeostasis. For example, starvation lowers both circulating T3 hormone and cellular T3 receptors.
Effects of Thyroid Hormones
The thyroid hormones are responsible for optimal growth, development, function, and maintenance of all body tissues. Excess or inadequate amounts result in the signs and symptoms of thyrotoxicosis or hypothyroidism (Table 38–4). Since T3 and T4 are qualitatively similar, they may be considered as one hormone in the discussion that follows.
Table 38–4. Manifestations of Thyrotoxicosis and Hypothyroidism.
System |
Thyrotoxicosis |
Hypothyroidism |
|
|
|
Skin and |
Warm, moist skin; sweating; heat |
Pale, cool, puffy skin; dry and brittle |
appendages |
intolerance; fine, thin hair; Plummer's |
hair; brittle nails |
|
nails; pretibial dermopathy (Graves' |
|
|
disease) |
|
|
|
|
Eyes, face |
Retraction of upper lid with wide |
Drooping of eyelids; periorbital edema; |
|
stare; periorbital edema; |
loss of temporal aspects of eyebrows; |
|
exophthalmos; diplopia (Graves' |
puffy, nonpitting facies; large tongue |
|
disease) |
|
|
|
|
Cardiovascular |
Decreased peripheral vascular |
Increased peripheral vascular resistance; |
system |
resistance, increased heart rate, stroke |
decreased heart rate, stroke volume, |
|
volume, cardiac output, pulse |
cardiac output, pulse pressure; low- |
|
pressure; high-output heart failure; |
output heart failure; ECG: bradycardia, |
|
increased inotropic and chronotropic |
prolonged PR interval, flat T wave, low |
|
effects; arrhythmias; angina |
voltage; pericardial effusion |
|
|
|
Respiratory |
Dyspnea; decreased vital capacity |
Pleural effusions; hypoventilation and |
system |
|
CO2 retention |
|
|
|
|
|
|
Gastrointestinal |
Increased appetite; increased |
Decreased appetite; decreased frequency |
system |
frequency of bowel movements; |
of bowel movements; ascites |
|
hypoproteinemia |
|
|
|
|
Central nervous |
Nervousness; hyperkinesia; emotional |
Lethargy; general slowing of mental |
system |
lability |
processes; neuropathies |
|
|
|
Musculoskeletal |
Weakness and muscle fatigue; |
Stiffness and muscle fatigue; decreased |
system |
increased deep tendon reflexes; |
deep tendon reflexes; increased alkaline |
|
hypercalcemia; osteoporosis |
phosphatase, LDH, AST |
|
|
|
Renal system |
Mild polyuria; increased renal blood |
Impaired water excretion; decreased |
|
flow; increased glomerular filtration |
renal blood flow; decreased glomerular |
|
rate |
filtration rate |
|
|
|
Hematopoietic |
Increased erythropoiesis; anemia1 |
Decreased erythropoiesis; anemia1 |
|
|
|

system |
|
|
|
|
|
Reproductive |
Menstrual irregularities; decreased |
Hypermenorrhea; infertility; decreased |
system |
fertility; increased gonadal steroid |
libido; impotence; oligospermia; |
|
metabolism |
decreased gonadal steroid metabolism |
|
|
|
Metabolic |
Increased basal metabolic rate; |
Decreased basal metabolic rate; slight |
system |
negative nitrogen balance; |
positive nitrogen balance; delayed |
|
hyperglycemia; increased free fatty |
degradation of insulin, with increased |
|
acids; decreased cholesterol and |
sensitivity; increased cholesterol and |
|
triglycerides; increased hormone |
triglycerides; decreased hormone |
|
degradation; increased requirements |
degradation; decreased requirements for |
|
for fatand water-soluble vitamins; |
fatand water-soluble vitamins; |
|
increased drug metabolism |
decreased drug metabolism |
|
|
|
1The anemia of hyperthyroidism is usually normochromic and caused by increased red blood cell turnover. The anemia of hypothyroidism may be normochromic, hyperchromic, or hypochromic and may be due to decreased production rate, decreased iron absorption, decreased folic acid absorption, or to autoimmune pernicious anemia.
Thyroid hormone is critical for nervous, skeletal, and reproductive tissues. Its effects depend on protein synthesis as well as potentiation of the secretion and action of growth hormone. Thyroid deprivation in early life results in irreversible mental retardation and dwarfism—symptoms typical of congenital cretinism.
Effects on growth and calorigenesis are accompanied by a pervasive influence on metabolism of drugs as well as carbohydrates, fats, proteins, and vitamins. Many of these changes are dependent upon or modified by activity of other hormones. Conversely, the secretion and degradation rates of virtually all other hormones, including catecholamines, cortisol, estrogens, testosterone, and insulin, are affected by thyroid status.
Many of the manifestations of thyroid hyperactivity resemble sympathetic nervous system overactivity (especially in the cardiovascular system), although catecholamine levels are not increased. Changes in catecholamine-stimulated adenylyl cyclase activity as measured by cAMP are found with changes in thyroid activity. Possible explanations include increased numbers of 
 receptors or enhanced amplification of the
receptors or enhanced amplification of the  receptor signal. Other clinical symptoms reminiscent of excessive epinephrine activity (and partially alleviated by adrenoceptor antagonists) include lid lag and retraction, tremor, excessive sweating, anxiety, and nervousness. The opposite constellation of symptoms is seen in hypothyroidism (Table 38–4).
receptor signal. Other clinical symptoms reminiscent of excessive epinephrine activity (and partially alleviated by adrenoceptor antagonists) include lid lag and retraction, tremor, excessive sweating, anxiety, and nervousness. The opposite constellation of symptoms is seen in hypothyroidism (Table 38–4).
Thyroid Preparations
See the Preparations Available section at the end of this chapter for a list of available preparations. These preparations may be synthetic (levothyroxine, liothyronine, liotrix) or of animal origin (desiccated thyroid).
Synthetic levothyroxine is the preparation of choice for thyroid replacement and suppression therapy because of its stability, content uniformity, low cost, lack of allergenic foreign protein, easy laboratory measurement of serum levels, and long half-life (7 days), which permits once-daily administration. In addition, T4 is converted to T3 intracellularly; thus, administration of T4 produces both hormones. Generic levothyroxine preparations can be used because they provide comparable