

Книги фарма 2 / Bertram G. Katzung-Basic & Clinical Pharmacology(9th Edition)
.pdfthan when the drug is snorted (Figure 32–2). Because the plasma half-life of cocaine is short, effects following a single dose persist only for an hour or so and repeated dosing may occur every 30 minutes. Because tolerance develops quickly, abusers may take monumental doses compared with those used medically, eg, as anorexiants. Total daily amphetamine doses as high as 4000 mg have been reported. After several days of such spree use, subjects may enter a paranoid schizophrenialike state. Typically, delusions that bugs are crawling under their skin develop, which leads to scratching and characteristic discrete excoriations. Finally, the spree is terminated by exhaustion from lack of sleep and lack of food, followed by a withdrawal syndrome. A typical pattern of withdrawal includes a ravenous appetite, exhaustion, and mental depression. This syndrome may last for several days after the drug is withdrawn.
Figure 32–2.
Comparison of blood concentrations achieved when cocaine is administered by different routes. Time to peak is nearly as fast by smoking as by intravenous injection. (Modified and reproduced, with permission, from Jones RT: The pharmacology of cocaine smoking in humans. In: Research Findings on Smoking of Abused Substances. National Institute on Drug Abuse Research Monograph 99. Chiang CN, Hawks RL [editors]. US Government Printing Office, 1990.)
Besides the paranoid psychosis associated with chronic use of amphetamines, a specific lesion associated with chronic amphetamine use is necrotizing arteritis, which may involve many small and medium-sized arteries and lead to fatal brain hemorrhage or renal failure. Overdoses of amphetamines are rarely fatal; they can usually be managed by sedating the patient with benzodiazepines.
Overdoses of cocaine are often rapidly fatal, victims dying within minutes from arrhythmias, seizures, or respiratory depression. Those who survive for 3 hours usually recover fully. Intravenous administration of diazepam, propranolol, or calcium channel-blocking drugs may be the best

treatment. The local anesthetic action of cocaine contributes to the production of seizures. The powerful vasoconstrictive action of cocaine has led to a significant number of patients with severe acute hypertensive episodes resulting in myocardial infarcts and strokes. This vasoconstrictive effect may also contribute to the multiple brain perfusion defects that have been described using single photon emission computed tomography (SPECT) blood flow imaging in cocaine abusers (Kosten, 1998). Finally, an epidemic of "cocaine babies" born to mothers who are using cocaine heavily has posed a major new challenge to health care facilities in the inner cities (Mayes, 1999). There are clear-cut deleterious effects on the pregnancy, with increased fetal morbidity and mortality as well as early childhood impairment in learning and attention.
Treatment
Subjects with residual emotional disorders, either schizophreniform psychosis or mental depression, may require treatment with antipsychotic or antidepressant drugs during weaning from stimulants. Dopamine agonists have been suggested to mitigate withdrawal from cocaine, reduce craving during abstinence, and facilitate abstinence, but neither these nor other agents have shown reliable efficacy. Depression occurs in up to 40% of stimulant-dependent patients, and antidepressants may be helpful for relapse prevention.
Nicotine dependence may respond to replacement therapy with either nicotine gum or transdermal patches, and detoxification from nicotine dependence has been described using clonidine. Bupropion, an antidepressant, also shows efficacy for smoking cessation. The nicotinic receptor blocker mecamylamine, which has good central nervous system access, has been used with limited efficacy. Overall, success rates for smoking abstinence at 1 year are about 20%, with even less success for depressed smokers.
Katzung PHARMACOLOGY, 9e > Section V. Drugs That Act in the Central Nervous System > Chapter 32. Drugs of Abuse >
Hallucinogens
History
Almost every society has found some bark, skin, leaf, vine, berry, fungus, or weed that contains "hallucinogenic" materials, but neither hallucinations nor psychotic states are typically induced by these drugs. The more recent "club drugs" including MDMA have also been considered to be like hallucinogens, but club drugs are better considered as related to either stimulants (MDMA) or sedatives (GHB).
Chemistry & Pharmacology
The LSD-like group of drugs includes lysergic acid diethylamide (LSD), mescaline, psilocybin, and their related compounds. LSD is a synthetic agent related to the ergot alkaloids (see Chapter 16: Histamine, Serotonin, & the Ergot Alkaloids), while mescaline, a phenethylamine derivative, and psilocybin, an indol-ethylamine derivative, are found in nature. Representative structures are shown in Figure 32–3. These drugs also have chemical resemblances to three major neurotransmitters: norepinephrine, dopamine, and serotonin. LSD interacts with several serotonin (5-HT) receptor subtypes in the brain. The drug displays agonist activity at 5-HT1A and 5-HT1C receptors. These actions may be more relevant to LSD's hallucinogenic action than its 5-HT2 receptor antagonism, because a number of other drugs with good antagonist effects at central 5-HT2 receptors are not
hallucinogenic.
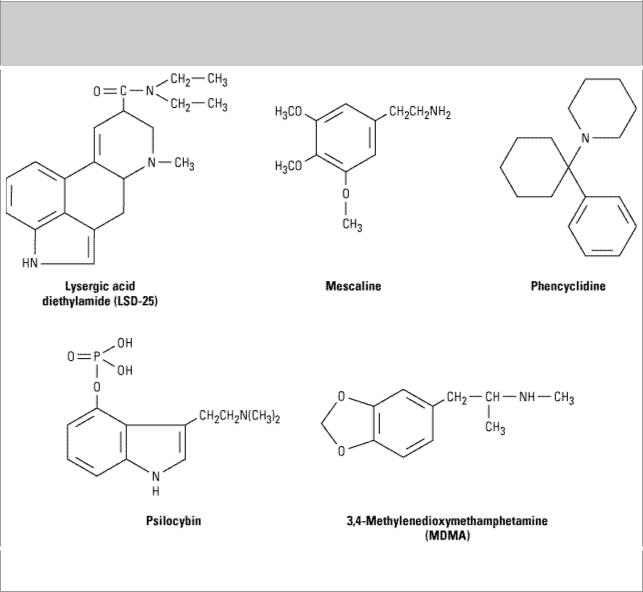
Figure 32–3.
Chemical structures of lysergic acid diethylamide (LSD), mescaline, phencyclidine, psilocybin, and the amphetamine analog MDMA.
Phencyclidine (PCP, "angel dust," many other names) is a synthetic phenylcyclohexylamine derivative originally used as a veterinary anesthetic. Ketamine, an analog, replaced phencyclidine as an anesthetic for use in humans (see Chapter 25: General Anesthetics). It too produces some emergent hallucinogenic effects. Since the 1970s, PCP and more recently ketamine have become widely accepted by drug abusers as desirable hallucinogenic agents. Phencyclidine may be smoked (by mixing the powder with tobacco), "snorted," taken orally, or injected intravenously.
Receptors for PCP have been identified in the brain, and PCP acts as an antagonist on the N-methyl- D-aspartate (NMDA) subtype of glutamate receptors. The drug is unique among hallucinogens in that animals will self-administer it.
The deliriant hallucinogens, exemplified by scopol-amine (see Chapter 8: Cholinoceptor-Blocking Drugs) and some synthetic centrally acting cholinoceptor-blocking agents, are different chemically as well as pharmacologically from the LSD group. Their effects seem to be entirely explainable by blockade of central muscarinic receptors. Similar mental effects may be seen during therapeutic or deliberate overdoses of commonly used medications with antimuscarinic action, such as

anticholinergic antiparkinsonism drugs, tricyclic antidepressants, and antispasmodics. Occasional instances of abuse of these therapeutic agents have occurred.
Clinical Effects
LSD produces a series of somatic, perceptual, and psychological effects that overlap each other. Dizziness, weakness, tremors, nausea, and paresthesias are prominent somatic symptoms. Blurring of vision, distortions of perspective, organized visual illusions or "hallucinations," less discriminant hearing, and a change in sense of time are common perceptual abnormalities. Impaired memory, difficulty in thinking, poor judgment, and altered mood are prominent psychological effects. Physiologically, LSD produces signs of central stimulation and overactivity of the sympathetic nervous system, manifested by dilated pupils, increased heart rate, mild elevation of blood pressure, tremor, and alertness. Virtually identical effects are produced by mescaline and psilocybin when they are given in equivalent doses. The onset of effects is fairly rapid, but the duration varies with the dose and is usually measured in hours. Phenomena may vary considerably from one user to another owing to such factors as the personality and expectations of the user and the circumstances under which the drug is taken, but the above effects occur in almost everyone. Waxing and waning of effects is typical.
Usual doses of LSD in humans are approximately 1–2 g/kg, making it one of the most potent pharmacologic agents known. The drug is equally effective parenterally or orally and consequently is almost always taken by mouth. Psilocybin is usually taken in doses of 250  g/kg and mescaline in doses of 5–6 mg/kg. Despite these differences in potency, the effects are virtually indistinguishable.
g/kg and mescaline in doses of 5–6 mg/kg. Despite these differences in potency, the effects are virtually indistinguishable.
PCP and ketamine produce detachment, disorientation, distortions of body image, and loss of proprioception. Somatic symptoms and signs include numbness, nystagmus, sweating, rapid heart rate, and hypertension. Overdosage has been fatal, as contrasted with the absence of known human fatalities directly caused by drugs of the LSD group.
Scopolamine and other antimuscarinic drugs produce delirium with fluctuating levels of awareness, disorientation, marked difficulty in thinking, marked loss of memory, and bizarre delusions. Most subjects, at least under experimental conditions, find these drugs to be unpleasant and have little desire to repeat the experience.
Use of these hallucinogens has not been associated with dependence or physiologic withdrawal symptoms. This is probably because tolerance develops rapidly, so that closely spaced dosing would be necessary to cause dependence; such frequent dosing is unusual.
Treatment
Common adverse psychologic consequences of hallucinogenic drugs include panic reactions ("bad trips") and acute psychotic reactions with PCP. Treatment includes benzodiazepines for sedation and constant monitoring by a nondrugged companion for several hours. Acidification of the urine (see Chapter 59: Management of the Poisoned Patient) may hasten PCP excretion.
Overdoses of the antimuscarinic agents can be treated with infusions of physostigmine, but supportive care is usually preferred.
Katzung PHARMACOLOGY, 9e > Section V. Drugs That Act in the Central Nervous System > Chapter 32. Drugs of Abuse >

Marijuana
History
Use of cannabis has been recorded for thousands of years, and about 200–300 million people use it currently, including 30–40 million persons in the USA. Recent surveys suggest its use is starting at an earlier age (sixth to eighth grade, 11–13 years). Because of proposed medical uses, it has been legalized in several states, although federal law prohibits its distribution for any purpose. Much cannabis is now grown indoors using genetically altered strains with 10-fold higher levels of  9- tetrahydrocannabinol (THC) (see below).
9- tetrahydrocannabinol (THC) (see below).
Chemistry & Pharmacology
With the exception of THC and its analogs, no other cannabinoids have definite psychoactivity, and the content of THC varies considerably among plants. Special genetic plant lines may produce as much as 4–6% THC content.
The preferred route of administration in Western countries is by smoking. The high lipid solubility of the drug leads to extensive sequestration in the lipid compartments of the body, and metabolites may be excreted for as long as a week after a single dose.
A G protein-coupled cannabinoid receptor (CB1) is most numerous in the outflow nuclei of the basal ganglia, the substantia nigra, pars reticulata, globus pallidus, hippocampus, and brainstem. Positron emission tomographic (PET) studies have revealed increases in metabolism following THC in the same areas in which receptors are localized, suggesting that these receptors are closely involved in the clinical actions of the drug.
THC has a variety of pharmacologic effects that resemble those of amphetamines, LSD, alcohol, sedatives, atropine, and morphine. Important opioid interactions include reduction in opioid dependence in CB1 knockout mice lacking the CB1 receptor.
Clinical Effects
The expert smoker of marijuana is usually aware of a drug effect after two or three inhalations. As smoking continues, the effects increase, reaching a maximum about 20 minutes after the smoke has been finished. Most effects of the drug usually have vanished after 3 hours, by which time plasma concentrations are low. Peak effects after oral administration may be delayed until 3–4 hours after

drug ingestion but may last for 6–8 hours.
The early stage is one of being "high" and is characterized by euphoria, uncontrollable laughter, alteration of time sense, depersonalization, and sharpened vision. Later, the user becomes relaxed and experiences introspective and dream-like states if not actual sleep. Thinking or concentrating becomes difficult, though by force of will the subject can attend.
Two characteristic physiologic signs of cannabis intoxication are increased pulse rate and reddening of the conjunctiva. The latter correlates well with the presence of detectable plasma concentrations. Pupil size is not changed. The blood pressure may fall, especially in the upright position. An antiemetic effect may be present. Muscle weakness, tremors, unsteadiness, and increased deep tendon reflexes may also be noted. Virtually any psychologic test shows impairment if the doses are large enough and the test difficult enough. No distinctive biochemical changes have been found in humans.
Tolerance has been demonstrated in virtually every animal species that has been tested. It is apparent in humans only among heavy long-term users of the drug. Different degrees of tolerance develop for different effects of the drug, with tolerance for the tachycardic effect developing fairly rapidly. A mild withdrawal syndrome has been noted following chronic use at very high doses.
Three epidemiologic studies in developing countries have failed to find definite evidence of impairment among heavy users of cannabis, but field studies may lack sensitivity. Experimental studies in which subjects have smoked heavily for varying periods have shown a lower serum testosterone level in men and airway narrowing. Reports of effects on immune mechanisms, chromosomes, and cell metabolism are often contradictory. Effects on the fetus are still uncertain.
Heavy smokers of marijuana may be subject to some of the same problems of chronic bronchitis, airway obstruction, and squamous cell metaplasia as smokers of tobacco cigarettes. Angina pectoris may be aggravated by the speeding of the heart rate, orthostatic hypotension, and increased carboxyhemoglobin. Driving ability is likely to be impaired but is not easily demonstrated with usual testing. "Amotivational syndrome," in which promising young people with obvious social advantages lose interest in school and career and enter the drug culture, is a real phenomenon, but one cannot be sure whether drug use is the cause of the problem or simply a matter of personal choice. Acute panic reactions, toxic delirium, paranoid states, and frank psychoses are rare. Brain damage has not been confirmed in humans, although some suggestion of ultrastructural damage has been found in animals.
Therapeutic THC is called dronabinol (Marinol) and has been marketed with approval by the Food and Drug Administration to reduce nausea and vomiting in patients undergoing cancer chemotherapy and to stimulate appetite in AIDS patients. It has also been shown to reduce intraocular pressure in glaucoma. Levonantradol, an analog, may be useful as an analgesic.
Few abusers seek treatment, but recent studies have suggested that behavioral treatments can stop abuse and improve cognitive functioning.
Katzung PHARMACOLOGY, 9e > Section V. Drugs That Act in the Central Nervous System > Chapter 32. Drugs of Abuse >
Inhalants

Chemistry
Four types of inhalants are abused: (1) anesthetic gases; (2) industrial solvents, including a variety of hydrocarbons, such as toluene; (3) aerosol propellants, such as various fluorocarbons; and (4) organic nitrites, such as amyl or butyl nitrite. The mode of action of the inhalant anesthetics has been discussed in Chapter 25: General Anesthetics.
Clinical Aspects
Anesthetic gases such as nitrous oxide produce difficulty in concentrating, dreaminess, euphoria, numbness and tingling, unsteadiness, and visual and auditory disturbances. Nitrous oxide is usually taken as 35% N2O mixed with oxygen; administration of 100% nitrous oxide may cause asphyxia and death. Ether and chloroform are readily available, and after an initial period of exhilaration, the person often loses consciousness.
Industrial solvents include gasoline, and various toxins such as toluene, benzene, and trichloroethylene. The clinical effects of industrial solvent inhalation are short, lasting only 5–15 minutes. Rags or "toques" are soaked in the solvent and the fumes inhaled. Aerosol propellants are usually inhaled from a plastic bag. Euphoria and a relaxed "drunk" feeling are followed by disorientation, slow passage of time, and possibly hallucinations.
Organic nitrites (amyl nitrite and isobutyl nitrite) cause dizziness, giddiness, rapid heart rate, lowered blood pressure, "speeding," and flushing of the skin. These effects last only a few minutes and can readily be repeated. The main effect of the drug on sexual performance is probably to enhance or prolong erection through the release of nitric oxide in the corpora cavernosa (see Chapter 19: Nitric Oxide, Donors, & Inhibitors).
Toxicity from chronic use of inhalants can be severe. Industrial solvents have produced liver, kidney, peripheral nerve, and possibly brain damage in animals, bone marrow suppression, and pulmonary disease. In human neuroimaging studies using magnetic resonance imaging, demyelination of white matter has been described in chronic abusers. Fluorocarbon inhalation has resulted in sudden deaths, due either to ventricular arrhythmias or to asphyxiation. Nitrites have been rather safe but might pose hazards (especially arrhythmias) for persons with preexisting cardiovascular problems. Finally, recent data have indicated that nitrate inhalants may reduce lymphocyte counts and natural killer cell activity, thereby acting as a cofactor for AIDS progression.
Katzung PHARMACOLOGY, 9e > Section V. Drugs That Act in the Central Nervous System > Chapter 32. Drugs of Abuse >
Steroids
History
Anabolic steroids were first used in competitive sports during the 1940s, and by the late 1980s, use was widespread in adolescents with distribution points in gymnasiums and physical fitness centers. However, the first urine testing for anabolic steroids did not occur until 1976 at the Olympic Games because of the fairly difficult assay methods needed for detection. These drugs are discussed in Chapter 40: The Gonadal Hormones & Inhibitors.
Clinical Use & Effects
Oral and injectable formulations of different steroids are often "stacked," ie, used simultaneously. Because detection of these different steroids is difficult and expensive, the history from the patient rather than urine toxicology is more generally useful for detecting anabolic steroid abuse. Anabolic steroids were added to Schedule III of the Controlled Substances Act in 1990.
Anabolic steroids are typically abused in a cyclic fashion, with a cycle of 4–18 weeks on steroids and 1 month to 1 year off. Abuse of other psychoactive drugs may occur in up to a third of these patients, but this is low compared with other substance abusers because of concerns about health and appearance by steroid abusers. The primary effects sought by abusers are increased muscle mass and strength, not euphoria. In the context of an adequate diet and sufficient physical activity, a significant increase in muscle mass and strength can be produced by these steroids.
Among the behavioral manifestations of heavy use are increases in aggression, changes in libido and sexual functions, and mood changes with occasional psychotic features. In studies comparing doses of 40–240 mg/d of methyltestosterone in a double-blind inpatient trial, irritability, mood swings, violent feelings, and hostility were greater during the high-dose period than at baseline. This clear ability of androgenic steroids to provoke aggression and irritability has aroused concerns about violence toward family members by abusers. In two prospective controlled trials using blinded administration, mood disturbances were reported in more than 50% of bodybuilders using anabolic steroids. Both increases and decreases in libido have been reported in studies comparing anabolic steroid abusers with nonusing athletes. Cognitive impairment, including distractibility, forgetfulness, and confusion, has also been demonstrated in controlled trials. A withdrawal syndrome has been described, with common symptoms being fatigue, depressed mood, and a craving for steroids.
Clinical findings may include hypertrophied muscles, acne, oily skin, hirsutism in females, gynecomastia in males, and needle punctures. Edema and jaundice may develop in heavy users. Common laboratory abnormalities include elevated hemoglobin and hematocrit measurements, elevated low-density lipoprotein cholesterol and depressed high-density lipoprotein cholesterol levels. Liver function test results may be elevated, and luteinizing hormone levels are usually depressed.
Treatment
Controlled trials of psychosocial treatments for anabolic steroid dependence have not been reported, and these individuals rarely present to substance abuse treatment programs. Patients may come to the attention of mental health professionals as a result of excessive aggression, sexual dysfunction, or mood disturbances. Peer counseling by former bodybuilders and group support may be of particular value for these users. Nutritional counseling and consultation with a fitness expert may also be helpful. Since gymnasiums are a frequent site for acquisition of steroids, abusers need to avoid these places until recovery is firmly established.

Section VI. Drugs Used to Treat Disease of the Blood, Inflammation, & Gout
Chapter 33. Agents Used in Anemias; Hematopoietic Growth
Factors
Katzung PHARMACOLOGY, 9e > Section VI. Drugs Used to Treat Disease of the Blood, Inflammation, & Gout > Chapter 33. Agents Used in Anemias; Hematopoietic Growth Factors >
Agents Used in Anemias; Hematopoietic Growth Factors: Introduction
Hematopoiesis, the production from undifferentiated stem cells of circulating erythrocytes, platelets, and leukocytes, is a remarkable process that produces over 200 billion new cells per day in the normal person and even greater numbers of blood cells in people with conditions that cause loss or destruction of blood cells. The hematopoietic machinery resides primarily in the bone marrow in adults and requires a constant supply of three essential nutrients—iron, vitamin B12, and folic acid—as well as the presence of hematopoietic growth factors, proteins that regulate the proliferation and differentiation of hematopoietic cells. Inadequate supplies of either the essential nutrients or the growth factors result in deficiency of functional blood cells. Anemia, a deficiency in oxygen-carrying erythrocytes, is the most common and easily treated of these conditions, but thrombocytopenia and neutropenia are not rare and in some forms are amenable to drug therapy. In this chapter, we first consider treatment of anemia due to deficiency of iron, vitamin B12, or folic acid and then turn to the medical use of hematopoietic growth factors to combat anemia, thrombocytopenia, and neutropenia.
Katzung PHARMACOLOGY, 9e > Section VI. Drugs Used to Treat Disease of the Blood, Inflammation, & Gout > Chapter 33. Agents Used in Anemias; Hematopoietic Growth Factors >
Agents Used in Anemias
Iron
Basic Pharmacology
Iron deficiency is the most common cause of chronic anemia—anemia that develops over time. Like other forms of chronic anemia, iron deficiency anemia leads to pallor, fatigue, dizziness, exertional dyspnea, and other generalized symptoms of tissue ischemia. The cardiovascular adaptations to chronic anemia—tachycardia, increased cardiac output, vasodilation—can worsen the condition of patients with underlying cardiovascular disease.
Iron forms the nucleus of the iron-porphyrin heme ring, which together with globin chains forms hemoglobin. Hemoglobin reversibly binds oxygen and provides the critical mechanism for oxygen delivery from the lungs to other tissues. In the absence of adequate iron, small erythrocytes with insufficient hemoglobin are formed, giving rise to microcytic hypochromic anemia.
Pharmacokinetics
The body has an elaborate system for maintaining the supply of the iron required for hematopoiesis.

It involves specialized transport and storage proteins whose concentrations are regulated by the body's demand for hemoglobin synthesis and adequate iron stores (Table 33–1). The vast majority of the iron used to support hematopoiesis is reclaimed from catalysis of the hemoglobin in old erythrocytes. Normally, only a small amount of iron is lost from the body each day, so dietary requirements are small and easily fulfilled by the iron available in a wide variety of foods. However, in special populations with either increased iron requirements (eg, growing children, pregnant women) or increased losses of iron (eg, menstruating women), iron requirements can exceed normal dietary supplies and iron deficiency can develop.
Table 33–1. Iron Distribution in Normal Adults.1,2
|
|
Iron Content (mg) |
||
|
|
|
|
|
|
|
Men |
|
Women |
|
|
|
|
|
Hemoglobin |
|
3050 |
|
1700 |
|
|
|
|
|
Myoglobin |
|
430 |
|
300 |
|
|
|
|
|
Enzymes |
|
10 |
|
8 |
|
|
|
|
|
Transport (transferrin) |
|
8 |
|
6 |
|
|
|
|
|
Storage (ferritin and other forms) |
|
750 |
|
300 |
|
|
|
|
|
Total |
|
4248 |
|
2314 |
|
|
|
|
|
1Adapted, with permission, from Brown EB: Iron deficiency anemia. In: Cecil Textbook of Medicine, 16th ed. Wyngaarden JB, Smith LH (editors). Saunders, 1982.
2Values are based on data from various sources and assume that "normal" men weigh 80 kg and have a hemoglobin of 16 g/dL and that "normal" women weigh 55 kg and have a hemoglobin of 14 g/dL.
Absorption
Iron is normally absorbed in the duodenum and proximal jejunum, though the more distal small intestine can absorb iron if necessary. The average diet in the USA contains 10–15 mg of elemental iron daily. A normal individual without iron deficiency absorbs 5–10% of this iron, or about 0.5–1 mg daily. Iron absorption increases in response to low iron stores or increased iron requirements. Total iron absorption increases to 1–2 mg/d in normal menstruating women and may be as high as 3–4 mg/d in pregnant women. Infants and adolescents also have increased iron requirements during rapid growth periods.
Iron is available in a wide variety of foods but is especially abundant in meat. The iron in meat protein can be efficiently absorbed, since heme iron in meat hemoglobin and myoglobin can be absorbed intact without first having to be broken down into elemental iron. Iron in other foods, especially vegetables and grains, is often tightly bound to phytates or other complexing agents and may be much less available for absorption. Nonheme iron in foods and iron in inorganic iron salts and complexes must be reduced to ferrous (Fe2+) iron before it can be absorbed by the intestinal mucosal cells. Such absorption is decreased by the presence of chelators or complexing agents in the intestinal lumen and is increased in the presence of hydrochloric acid and vitamin C.