

Covid -19: etiology, pathogenesis, pathological anatomy, complications, causes of death.
SARS-CoV-2 is a single-stranded RNA-containing virus belonging to the Coronaviridae family. The genetic sequence of SARS-CoV-2 is 79% similar to SARS-CoV. The pathogenesis of COVID-19 has not yet been sufficiently studied. Two ways of entering the cell are assumed: the receptor for the APF2 enzyme or the transmembrane glycoprotein CD147 can serve as the receptor of the virus. The preferred path of virus penetration into the cell has not been established either. ► APF2. •The S-protein of the crown of viruses mimics angiotensin converting enzyme 2 (APF2) in its structure. Due to this, viral particles successfully bind to APF2 receptors (there are many of them on the surface of lung cells — alveolocytes), after which they inject their RNA into the cell.
•The interaction of the virus with these receptors is carried out through the S2 subunit through
heptad repeats 1 and 2 (HR1 and HR2).
•Affinity to the APF2 receptor of the S-protein of the SARS-CoV-2 virus is 10-20 times greater than
SARS-CoV-1, which causes great contagiousness.
•The molecules that provide invagination of the cell membrane with the virus-receptor complex are not known.
► CD147. •The mechanism of penetration into the cell is the same as when penetrating through APF2. The CD147 receptor belongs to the immunoglobulin family.
•According to in vitro laboratory studies, monoclonal antibodies (mepolizumab) may be effective in blocking the pathway through CD147.
► Once in the cell, the RNA starts the process of virus replication. The virus is assembled in several independent parts, after which the virion-containing bubbles merge with the plasma membrane, and the virus is isolated.
Unlike other pathogenic coronaviruses that cause seasonal acute respiratory viral infections, SARS-CoV-2 replicates in the upper respiratory tract without a pronounced clinical picture.
Complications
- Pulmonary edema.
- ARDS.
- Acute heart failure.
- OPN.
- Infectious and toxic shock.
-Hemorrhagic syndrome on the background of a decrease in blood platelets (DIC).
-Multiple organ failure (dysfunction of many organs and systems).
Morphological changes in COVID-19 depend on the course variant and
stages of the disease, as well as comorbid diseases, which are especially common
they occur in deceased older age groups.
Currently, the diagnosis of the infectious disease COVID-19
it is established only in the presence of laboratory (by PCR) confirmation in
a certified laboratory for the presence of the SARS-CoV-2 virus.
Influenza: etiology, pathogenesis, pathological anatomy, complications, causes of death.
Influenza- ARVI caused by viruses The source of human disease is a sick person. Hybridization of animal and human viruses is possible, which leads to variability of the pathogen and the appearance of pandemic dangerous strains.
Etiology. The pathogens are pneumotropic RNA-containing viruses of three antigenically determined serological variants: A (A1, A2), B and C. Pathogenesis. The infection spreads through the air-
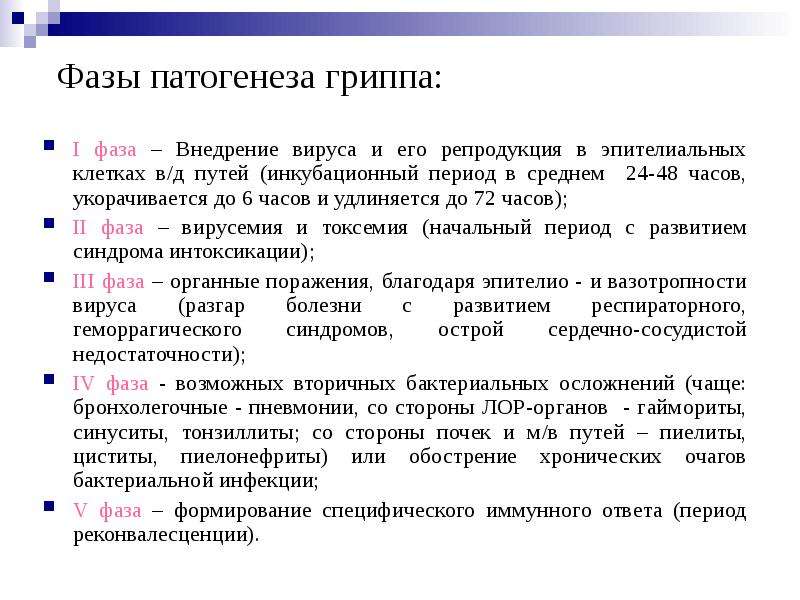
Pathological anatomy. Changes in influenza are different and depend on the severity of its course, which is determined by the type of pathogen (influenza A flows more heavily), on the strength of its effects, the state of the macroorganism and the attachment of a secondary infection. There are mild (outpatient), moderate and severe forms of influenza.
- The mild form is characterized by a lesion with VDP, where acute catarrhal rhinolaryngotracheobronchitis develops. The skin is swollen, hyperemic, with excessive serous-mucous discharge. Microscopically, hydropic dystrophy of the cells of the ciliated epithelium, loss of cilia are noted; secretory activity of goblet cells and serous-mucous glands is enhanced, many epithelial cells are desquamated. The presence of basophilic and oxyphilic inclusions in the cytoplasm of epithelial cells is characteristic.
-Moderate severity occurs with the involvement of small bronchi, bronchioles and pulmonary parenchyma. Serous hemorrhagic inflammation develops in the trachea and bronchi, sometimes with foci of mucosal necrosis - necrotic tracheitis. Epithelial cells are fused for a considerable length in the form of layers, fill the lumen of the bronchi, which leads to focal atelectasis and acute emphysema of the lungs. Against the background of fullness of blood, areas of atelectasis and acute emphysema, foci of influenza pneumonia appear. The course is favorable: recovery occurs after 3-4 weeks. In weakened people, the elderly, children and patients with CC diseases, pneumonia acquires a prolonged course, leading to cardiopulmonary failure and death.
- The severe form has two varieties: 1- due to severe general intoxication, 2- pulmonary complications due to secondary infection. In severe influenza with severe general intoxication, the cyto- and vasopathic effects of the virus are in the first place. Serous hemorrhagic inflammation and necrosis occur in the trachea and bronchi. There are many small foci of serous hemorrhagic pneumonia in the lungs, alternating with foci of acute emphysema and atelectasis.
Complications. Exudate carnification, obliterating bronchitis and bronchiolitis, bronchial wall sclerosis lead to bronchiectasis, pneumofibrosis, chronic obstructive emphysema, chronic pneumonia, pulmonary heart failure. Encephalitis, arachnoiditis, neuritis), lead to disability of patients. Death occurs from intoxication, cerebral hemorrhages, pulmonary complications (pneumonia, pleural empyema), cardiac or cardiopulmonary insufficiency.
Acute respiratory infections: etiology, pathogenesis, pathological anatomy, complications. outcomes.
Influenza- ARVI caused by viruses The source of human disease is a sick person. Hybridization of animal and human viruses is possible, which leads to variability of the pathogen and the appearance of pandemic dangerous strains.
Etiology. The pathogens are pneumotropic RNA-containing viruses of three antigenically determined serological variants: A (A1, A2), B and C. Pathogenesis. The infection is spread by airborne droplets. Latent (asymptomatic) and chronic forms are possible
Pathological anatomy. Changes in influenza are different and depend on the severity of its course, which is determined by the type of pathogen (influenza A flows more heavily), on the strength of its effects, the state of the macroorganism and the attachment of a secondary infection. There are mild (outpatient), moderate and severe forms of influenza.
- The mild form is characterized by a lesion with VDP, where acute catarrhal rhinolaryngotracheobronchitis develops. The skin is swollen, hyperemic, with excessive serous-mucous discharge. Microscopically, hydropic dystrophy of the cells of the ciliated epithelium, loss of cilia are noted; secretory activity of goblet cells and serous-mucous glands is enhanced, many epithelial cells are desquamated. The presence of basophilic and oxyphilic inclusions in the cytoplasm of epithelial cells is characteristic.
-Moderate severity occurs with the involvement of small bronchi, bronchioles and pulmonary parenchyma. Serous hemorrhagic inflammation develops in the trachea and bronchi, sometimes with foci of mucosal necrosis - necrotic tracheitis. Epithelial cells are fused for a considerable length in the form of layers, fill the lumen of the bronchi, which leads to focal atelectasis and acute emphysema of the lungs. Against the background of fullness of blood, areas of atelectasis and acute emphysema, foci of influenza pneumonia appear. The course is favorable: recovery occurs after 3-4 weeks. In weakened people, the elderly, children and patients with CC diseases, pneumonia acquires a prolonged course, leading to cardiopulmonary failure and death.
- The severe form has two varieties: 1- due to severe general intoxication, 2- pulmonary complications due to secondary infection. In severe influenza with severe general intoxication, the cyto- and vasopathic effects of the virus are in the first place. Serous hemorrhagic inflammation and necrosis occur in the trachea and bronchi. There are many small foci of serous hemorrhagic pneumonia in the lungs, alternating with foci of acute emphysema and atelectasis.
Complications. Exudate carnification, obliterating bronchitis and bronchiolitis, bronchial wall sclerosis lead to bronchiectasis, pneumofibrosis, chronic obstructive emphysema, chronic pneumonia, pulmonary heart failure. Encephalitis, arachnoiditis, neuritis), lead to disability of patients. Death occurs from intoxication, cerebral hemorrhages, pulmonary complications (pneumonia, pleural empyema), cardiac or cardiopulmonary insufficiency.