

6 курс / Кардиология / 30_лет_поиска_медикаменты,_ангиопластика_или_хирургия
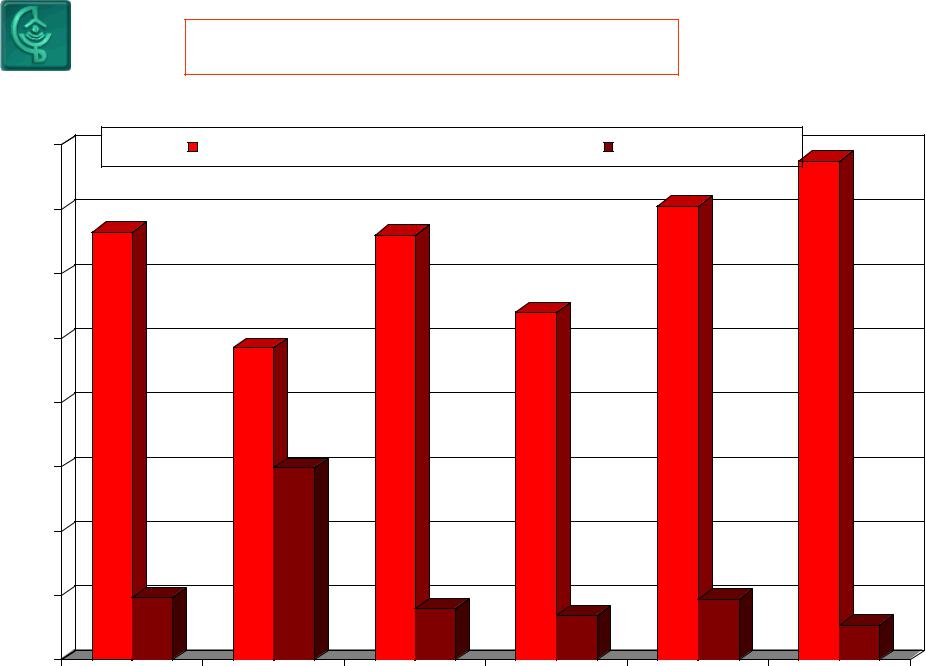
.pdfЧастота направлений на различные типы лечения ИБС
70 |
АКШ |
терапия |
РТСА |
66.5 |
69.6 |
|
|
|
58.4 |
|
|
60 |
|
|
|
|
|
|
50.7 |
51.3 |
|
|
|
50 |
|
|
|
|
|
|
|
|
39.8 |
|
|
40 |
|
|
|
|
36.5 |
|
33.3 |
|
|
|
|
|
|
|
|
|
|
30 |
27.6 |
|
|
|
|
|
|
|
25.2 |
|
|
|
22.7 |
|
|
|
|
20 |
|
15.4 |
12.8 |
|
|
|
|
|
|
|
|
10 |
|
|
|
8.3 |
|
|
|
|
|
4.9 |
0
1999 |
2000 |
2001 |
2002 |
2003 |
|
|
Результаты лечения ИБС |
|
|||
16 |
|
рецидив стенокардии +ПРМ |
|
всего МАСЕ |
15.5 |
|
|
|
|
|
|
14.1 |
|
14 |
13.3 |
|
13.2 |
|
|
|
12 |
|
|
|
10.8 |
|
|
|
|
|
|
|
|
|
10 |
|
9.7 |
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
5.97 |
|
|
|
|
6 |
|
|
|
|
|
|
4 |
|
|
|
|
|
|
2 |
1.95 |
|
1.6 |
1.4 |
1.9 |
|
|
|
|
1.1 |
|||
|
|
|
|
|
|
|
0 |
|
|
|
|
|
|
|
ВСЕГО |
1999 |
2000 |
2001 |
2002 |
2003 |
|
|
|
Рекомендовано к покупке и прочтению разделом по кардиологии сайта https://meduniver.com/ |
|||
|
|
АНГИОПЛАСТИКА vs АКШ |
|
||||||
|
10% |
|
|
|
|
|
|
|
10% |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. одно. и |
|
|
|
|
|
1. |
Диабет |
|
|
двухсосудистые, |
|
|
|
|
|
|||
|
|
|
|
|
|
2. |
Множественные |
||
|
поражения типа А,В |
|
|
|
|
|
|||
|
|
|
80% |
|
|
«недилатабельные» |
|||
|
2. ОИМ, |
|
|
|
|
||||
|
|
|
|
|
поражения, |
||||
|
нестабильная |
|
|
|
|
|
|||
|
|
|
|
|
|
3. |
«Старые» |
||
|
стенокардия |
|
|
|
|
|
|||
|
|
|
|
|
|
Окклюзии |
|||
|
3. окклюзии (культя, |
|
|
|
|
|
|||
|
|
|
|
|
|
4. |
ФИ < 0,5 |
||
|
возраст < 3 мес) |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
Множественные поражения (в том числе |
|
|
типа В и С, с кальцинозом) |
? |
||
3. |
Длинные, диффузные поражения |
||
4. |
Поражения венозных шунтов |
||
5. |
Бифуркационные стенозы |
МЕДИКАМЕНТЫ |
|
6. |
Стенозы ствола ЛКА |
||
|
|||
7. |
Окклюзии (без «мостовых» коллатералей) |
|
|
8. |
Стенозы мелких ветвей и дистального русла |
|
|
|
|
|
|
СООТНОШЕНИЕ ЧКИ/АКШ В США В 2000 ГОДУ
(Smith et al. JACC, 2001, vol. 37, No. 8; pp. 1-66)
|
ЧКИ |
38% |
АКШ |
|
62%
Рекомендовано к покупке и прочтению разделом по кардиологии сайта https://meduniver.com/
ИНВАЗИВНЫЕ ПРОЦЕДУРЫ В США (2005г.)
Кол-во, тыс.
1600 |
|
1400 |
|
1200 |
1450 |
|
|
1000 |
|
800 |
|
600 |
|
400 |
|
200 |
|
0 |
|
катетеризации
1100
1085
340
93,2%
ЧТКА |
АКШ |
-Общее количество процедур
-количество стентирований
Источник: Heart disease & stroke statistics-2005,Update, AHA

Nonoperative dilatation of coronary-artery stenosis: percutaneous transluminal coronary angioplasty.
Grüntzig AR, Senning A, Siegenthaler WE.
N Engl J Med Jul 1979; 301(2):61-8
Abstract
In percutaneous transluminal coronary angioplasty, a catheter system is introduced through a systemic artery under local anesthesia to dilate a stenotic artery by controlled inflation of a distensible balloon. Over the past 18 months, we have used this technic in 50 patients. The technic was successful in 32 patients, reducing the stenosis from a mean of 84 to 34 per cent (P less than 0.001) and the coronary-pressure gradient from a mean of 58 to 19 mm Hg (P less than 0.001). Twenty-nine patients showed improvement in cardiac function during follow-up examination. Because of acute deterioration in clinical status, emergency bypass was later
necessary in five patients; three showed electrocardiographic evidence of infarcts. Patients with single-vessel
disease appear to be most suitable for the procedure, and a short history of pain indicates the presence of a soft (distensible) atheroma likely to respond to dilatation. We estimate that only about 10 to 15 per cent of candidates for bypass surgery have lesions suitable for this procedure. A
prospective randomized trial will be necessary to evaluate its usefulness in comparison with surgical and medical management.
Рекомендовано к покупке и прочтению разделом по кардиологии сайта https://meduniver.com/

Indications of coronary angioplasty and stenting in 2003: what is left to surgery?
Poyen V, Silvestri M, Labrunie P, Valeix B.
J Cardiovasc Surg (Torino) Jun 2003; 44(3):307-12
Affiliation
Cardiovascular Unit, U.C.V. Marseille, France. vpoyen@ucvnet.com
Abstract
For many years, coronary artery by-pass graft (CABG) remained the only effective treatment of multivessel disease compared to medical treatment. The first technical revolution was in 1977 when Gruentzig introduced balloon percutaneous transluminal coronary angioplasty (PTCA), the 2nd in the 90's with the developments of stents and
In the 90's, interventional cardiology played a predominant role in revascularization as the number of CABG decreased at the same time, and emergency CABG for bail out almost disappeared (0% to 0.5%). Systematic stenting decreased the need
for repeat revascularization to about 18-20% nowadays in the majority of centers, except in diabetic patients. Despite this fact restenosis remains the pitfall of angioplasty, mostly in diabetic patients presenting multivessel disease in which surgery with "all arterial grafts" gives good long term RESULTS: The first studies
comparing PTCA and CABG are favourable to surgery (BARI), then late ones using stents (ARTS, ERACI 2) showed that stenting was at least equivalent to CABG, in terms of mortality or serious complications (major acute coronary events, MACE),
same results are observed by stenting a high risk lesion as the unprotected left main stenosis can be, until then treated surgically. However, high volume centers studies treating by PTCA+stent the unprotected left main artery (LMA) shows that the 1 year survival rate is similar to surgery, but always related to a restenosis rate of 20% at 6 months in the stent group, which represents the only significant difference in terms of MACE; the new drug eluting stents lead us to expect,
according to SIRIUS and TAXUS II studies, to reduce the restenosis rate, and by the way, the MACE
could be dramatically lowered from 50% to 60%. Randomised studies would be necessary, but the extrapolation of the actual data, more particularly results of subgroups with a high risk of restenosis, diabetic patients and small vessels, lead us to think that stenting could come in first intention before surgery if TVR is significantly reduced. A complex anatomy, failed attempted chronic occlusion, several lesions on tortuous vessels, would remain the last surgical indication if CABG provides a more complete revascularization. The impact of these new drugs seems promising. However, we should await early results of studies in diabetic patients and bifurcations. But in high volume experienced centers, CABG indications would be reduced in the future to the technical pitfalls of stenting (complex or tortuous anatomy, chronic occlusions) or to the adverse additional cost of this device, unless reduction of restenosis or TVR could also cancel this extra cost. We expect randomised studies CABG versus stented angioplasty using drug eluting stents to confirm these preliminary data.
Fewer cardiac surgeon jobs available
Posted 2/13/2007 1:52 AM ET
| Subscribe to stories like this 
Cardiac surgeon Mike Bauer, right, and his team repair one heart valve and replace another for Troy Sanders at St. Vincent Infirmary Medical Center in Little Rock, Ark.
By Julie Appleby, USA TODAY
It was almost a given: Go to medical school, spend an additional 10 years to become a
heart surgeon, then you've got it made. But new ways of treating heart disease have changed that outlook: Cardiac surgeons are having a tougher time finding work.
The use of artery-opening stents has helped lead to a sharp drop in the number of patients having cardiac bypass surgery and contributed to a tight job market for cardiac surgeons and
falling interest in the specialty by medical school graduates.
"If you look at the market right now, it's like everyone is at a big fancy ball, but the cardiac surgeons are the ones not getting asked to dance," says Kurt Mosley, a vice president at Merritt Hawkins & Associates, a health care staffing firm. "Ten years ago, they were right up there."
A survey of 88 cardiothoracic residents finishing their training
found that 12% received no job offers in 2004, according to a 2006 article in the Annals of Thoracic Surgery. At the same time, the number of applicants choosing to pursue one of the 140 training spots each year has also declined. In 2005, there were only 104 applicants filling 100 of the 139 available spots, according to the article.
"In general, graduating residents were extremely disappointed with job opportunities," says co-author Richard Lee, assistant director of residency programs at St. Louis
Рекомендовано к покупке и прочтению разделом по кардиологии сайта https://meduniver.com/
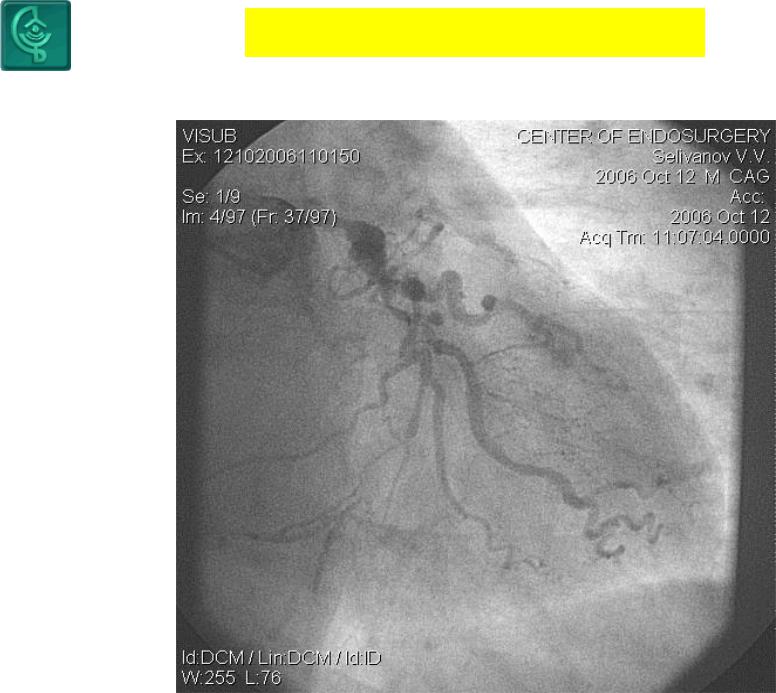
АКШ БОЛЬШЕ НЕ НУЖНА?
ИЛИ КТО ВОЗМЕТСЯ СТЕНТИРОВАТЬ ЭТУ АРТЕРИЮ?
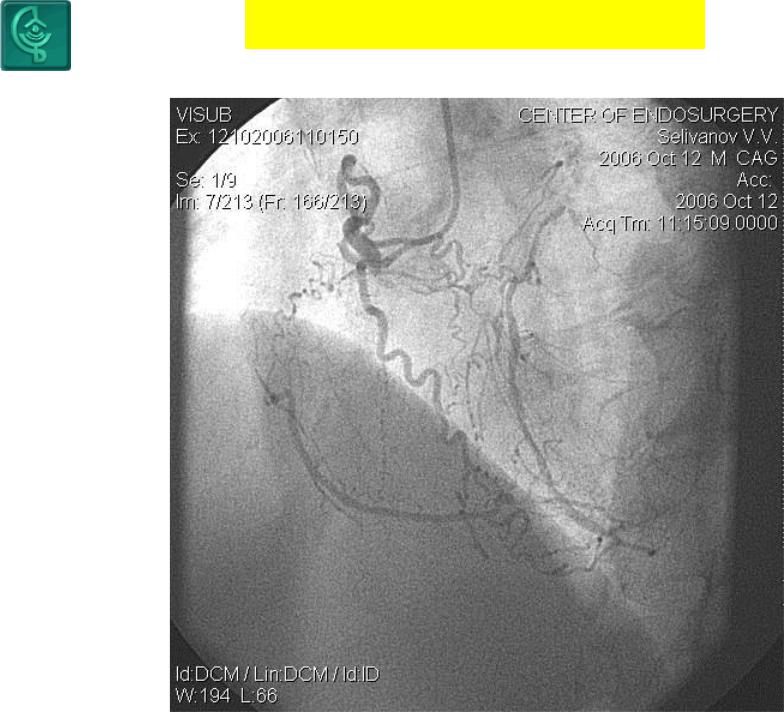
АКШ БОЛЬШЕ НЕ НУЖНА?
ИЛИ КТО ВОЗМЕТСЯ СТЕНТИРОВАТЬ ЭТУ АРТЕРИЮ?
Рекомендовано к покупке и прочтению разделом по кардиологии сайта https://meduniver.com/