


MILIARIA
•Disorder due to blockage of eccrine sweat ducts .
•Subdivided into three subtypes dependent on the level of blockage:
-Miliaria crystallina (stratum corneum),
-Miliaria rubra (deeper within the spinous layer)
-Miliaria profunda (dermal–epidermal junction)
54
•Miliaria rubra and miliaria crystallina-common in neonates.
•Predisposing factors : Immature sweat ducts are an important factor in neonates.
•Environmental factors : Heat, humidity, occlusive clothes and plastic sheets.
55
MILIARIA CRYSTALLINA
•CAUSE- obstruction of the eccrine sweat duct as it courses through the stratum corneum.
•Sweat collects beneath the stratum corneum, causing clear, small, flaccid vesicles
•Often likened to “dew drops” & presents as crops of clear, thin walled, superficial vesicles 1–2 mm in
diameter, without associated erythema. |
56 |
|

•Delicate and generally rupture within 24 hr, and are followed by bran-like desquamation.
•Lesions are asymptomatic.
•They arise most frequently during the first 2 weeks of life
•Likely to be seen on the forehead, scalp, neck and upper trunk.
The tiny, superficial vesicles on the back and neck of newborn .
57

MILIARIA RUBRA (‘PRICKLY HEAT’)
•Usually seen after the first week of life
•Also caused by a blockage of the sweat ducts, but
deeper within the spinous layer.
•Obstructed flow leads to leakage of fluid into the lower epidermis and upper dermis, resulting in an inflammatory response producing small erythematous papules, papulo-vesicles, and pustules.
58
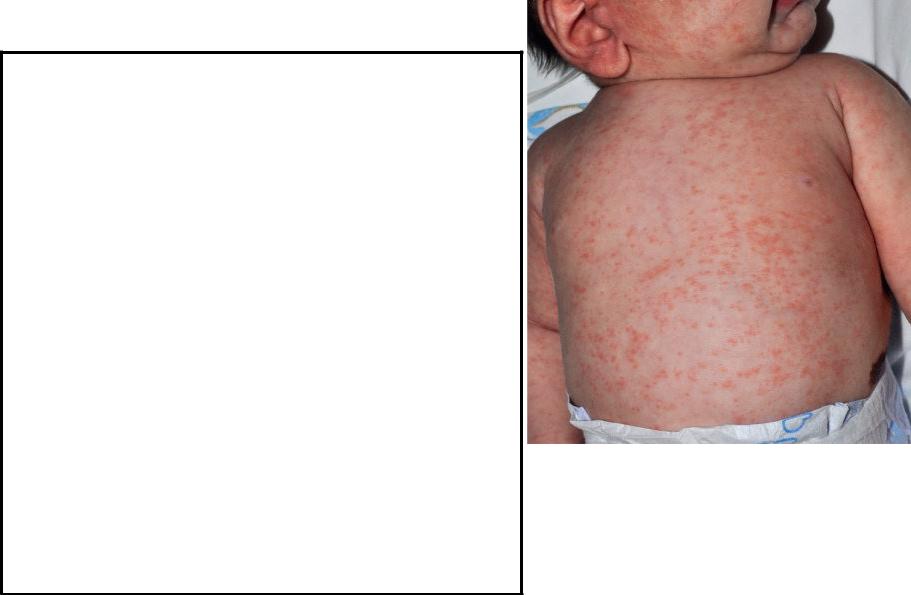
•Lesions occur in -flexural areas, especially around the neck and in the groins and axillae.
•Lesions can be itchy or sore.
•Each crop of lesions will subside within 2–3 days, but recurrences are common unless the provocative environmental conditions are
modified.
59

•Frequently, some lesions are pustular (miliaria pustulosa), but this does not necessarily indicate secondary infection.
MILIARIA PUSTULOSA
60
Management
•Milaria crystallina spontaneously improves without therapy over a few weeks as the sweat ducts mature.
•Miliaria rubra will improve in a few weeks without medical treatment if the child is removed from conditions of high heat/humidity and any occlusive clothing or bedding is removed.
•Topically, a soothing agent like calamine lotion is useful. Antibiotics may be needed
61
DIAPER DERMATITIS (NAPKIN DERMATITIS OR
NAPPY RASH)
•Diaper dermatitis-one of the most common skin problems in the newborn.
•Term “diaper dermatitis” mean any skin disease in the diaper area.
•Neonatal skin is irritated with contact from urine, feces, and occlusive condition.
62
Three common types of diaper dermatitis are are -
1)Frictional dermatitis : friction with skin and fabric leads to a breach in stratum corneum, sp. Over perineal area, buttock, and waistlines.
2)Irritant contact dermatitis : due to contact with proteolytic enzyme in stool ,chemical like soap, detergents. It involves convex surface of buttock, vulva, perineal area, lower abdomen, and proximal thigh sparing intertriginous area.
3)Diaper candidiasis
63