

•Infants generally show little sign of residual disease after the age of 1 year.
Management
•The skin lesions of neonatal LE require no treatment, but sun protection is essential.
•Up to 50% of infants with cardiac involvement will require a pacemaker.
•Treatment with high dose systemic steroids may be indicated for fetal bradycardia where there are signs of heart failure.
104
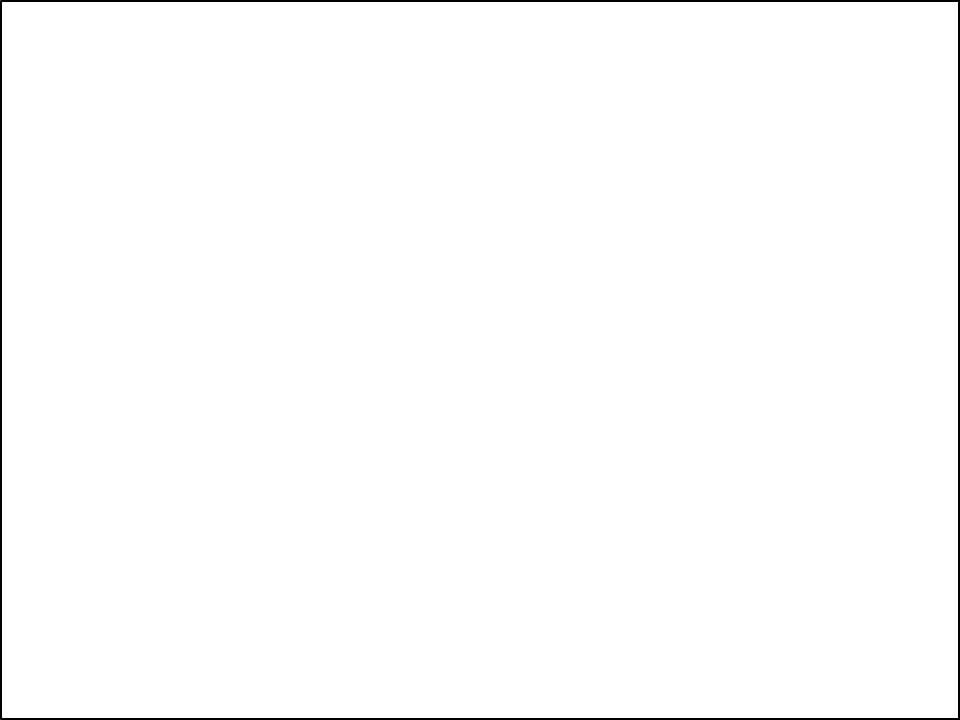
GENODERMATOSIS
•They are inherited skin conditions,majority are lifelong
•A/W- high morbidity due to incurable nature
•Patterns of inheritance-AD,AR,XLD,XLR
•Management- symptomatic
105
SOURCE-IADVL |
106 |
MISCELLANEOUS DISORDERS
• Colloidion baby
107
COLLODION BABY
•Highly characteristic clinical entity present at birth where a child is born with an ‘extra’ skin resembling a shiny membrane or collodion.
•The severely affected infant is bright red and encased in a taut, glistening, yellowish, translucent covering resembling collodion.
108
•Almost 90% of collodion babies will go on to develop a severe form of autosomal recessive ichthyosis in the first few weeks of life:
-lamellar ichthyosis
-non bullous ichthyosiform erythroderma (syn. congenital ichthyosiform erythroderma)
109

•Within hours, this membrane
dries and cracks, and bleeding may occur Within 1 or 2 days, it starts to peel off
The shedding will more or less complete within 4 weeks Subsequently, the typical features of one of several varieties of ichthyosis gradually emerge over a period of weeks or months.
110
MANAGEMENT
•Incubation in a high humidity atmosphere, with careful monitoring of body temperature.
•Fluid and electrolyte balance.
•Fluid loss is significantly reduced by frequent applications of lipid, a mixture of white soft paraffin and liquid paraffin is ideal.
•Frequent oiling.
111
REFERENCES
•ROOK’S TEXTBOOK OF DERMATOLOGY
•HARPER’S TEXTBOOK OF PAEDIATRIC DEMATOLOGY
•IADVL TEXTBOOK OF DERMATOLOGY 4th edition
•Neonatal Dermatoses and knowledge, attitude, practice of postnatal mothers from South India(Neha Sharma, Jayadev Betkerur, LSS Manickam)
112