

4 курс / Дерматовенерология / Дерматоскопия (3)
.pdf© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
220 Non-pigmented (amelanotic) lesions
a consideration of invasive squamous cell carcinoma
(9). Erythema and white circles are also found in lupus erythematosus (10). When sclerosis becomes prominent, lesions of lupus erythematosus show white structureless zones, especially in the center. The polarizing specific “four dot clod” can be found in actinic keratosis and in lupus erythematosus (15).
Nodular non-pigmented lesions
The assessment of non-pigmented nodular lesions is one of the biggest challenges in dermatoscopy. The differential diagnosis to be taken into account is vast. Benign nodular non-pigmented non-melanocytic lesions include seborrheic keratoses (6.29), dermatofibromas (4), warts (22) (including molluscum contagiosum, 6.30 middle), infectious nodules (for example Leishmaniasis (19)), all forms of prurigo (35) (for example picker’s nodule), angioma (including pyogenic granuloma, 6.3), sebaceous gland hyperplasia (12, 13) (6.11), clear cell acanthoma (36) (6.31), common benign neoplasms such as pilomatrixoma (23) (6.15) and rare ones such as eccrine poroma (37, 38) (6.32) or trichoepithelioma (39) (6.33), and all kind of cysts including epidermal cysts or mucoid (myxoid) finger cysts (40) (6.34). Non-melanocytic malignancies include poorly (41) (6.30 top, 6.35 bottom left) and well differentiated squamous cell carcinomas (9) (including keratoacanthoma, 6.35, top left), basal cell carcinoma (33) (6.36), rare cutaneous malignancies like Merkel cell carcinoma (42) (6.37), and cutaneous metastases of any malignancy. In melanocytic lesions the differential diagnoses are limited to Unna or Miescher nevus (6.38), Spitz nevus and melanoma (6.35 bottom right, 6.39).
The principal nodular non-pigmented lesions and their dermatoscopic appearances are listed in table 6.3. Based on the descriptions of individual lesions it becomes clear that the morphology of vessels assists little in diagnosis. Unlike flat lesions, the distinction between monomorphous and polymorphous patterns of vessels has no diagnostic significance for nodules. With the exception of some specific arrangements discussed below, vascular patterns have poor specificity for nodular non-pigmented lesions. Therefore, ulceration, keratin and white clues are given priority over vessel pattern analysis when assessing nodules.
As stated previously, in the absence of a clear and convincing history of trauma, any solitary ulcerated non-pigmented nodule should be submitted for histopathology. In most ulcerated non-pigmented nodules it will not be possible to come to a specific diagnosis by dermatoscopy. Nodular basal cell carcinomas are the commonest nodular malignancy and they are frequently ulcerated, but any other malignant neoplasm like Merkel cell carcinoma and melanoma can also be ulcerated. Benign conditions that may present as ulcerated nodules include pyogenic granulomas, nodular prurigo (picker’s nodule) and some infectious diseases (e.g. leishmaniasis).
If surface keratin is present in an amelanotic nodule, the principal diagnoses are well-differentiated squamous cell carcinoma/keratoacanthoma, warts, and seborrheic keratosis. The presence of keratin helps to distinguish well-differentiated squamous cell carcinomas or keratoacanthomas from other raised non-pigmented neoplastic lesions such as basal cell carcinomas, Merkel cell carcinomas and amelanotic melanomas. Unna or
Table 6.3: Raised non-pigmented lesions
Diagnosis |
Pattern of vessels |
Basal cell carcinoma |
Serpentine, branched vessels |
Keratoacanthoma |
Radially arranged vessels as lines that |
|
may be straight, curved, serpentine, |
|
looped or branched |
Squamous cell carcinoma |
All types of vessels as lines, including |
(well differentiated) |
coiled ones, occasionally also |
|
branched vessels |
Squamous cell carcinoma |
All types of vessels as lines, including |
(poorly differentiated) |
coiled ones, occasionally also |
|
branched vessels, vessels cover more |
|
than 50 % of the lesion |
Dermatoscopic clues and clues beyond dermatoscopy
Dermatoscopic clues: Ulceration, white lines, structureless white
Dermatoscopic clues: Central keratin plug (stronger clue when branched serpentine vessels are adjacent to keratin plug), surface keratin, white structureless areas and white circles
Dermatoscopic clues: Surface keratin, white structureless areas and white circles
Dermatoscopic clues: absence of surface keratin, white structureless areas and white circles

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Diagnosis |
Pattern of vessels |
Clear cell acanthoma |
Coiled or dot vessels in serpiginous |
|
arrangement |
Eccrine poroma |
Coiled, serpentine and branched |
|
vessels, polymorphous vessels |
Hemangiomas and vascular |
Vessels as clods |
malformations (including |
|
pyogenic granuloma) |
|
Prurigo (picker’s nodule) |
Radial vessels (if centrally ulcerated), |
|
serpiginous arrangement of vessels |
|
occasionally |
Viral warts |
Verruca plana: Monomorphous vessels |
|
as dots |
|
Verruca vulgaris: Skin-colored to white |
|
clods, each with a central dot vessel |
|
Verruca plantaris/palmaris: Yellow |
|
structureless zone with red to black |
|
dots and lines (hemorrhage) |
Leishmaniasis |
Polymorphous vascular pattern |
Metastasis |
Polymorphous with linear vessels, |
|
branched vessels |
Molluscum contagiosum |
Radial vessels |
Merkel cell carcinoma |
Branched vessels and other vessels as |
|
lines |
Sebaceous gland hyperplasia |
Radial vessels, usually curved or |
|
serpentine |
Dermatofibroma |
Vessels as dots |
Calcinosis cutis |
Serpentine Vessels |
Pilomatrixoma |
Serpentine Vessels |
Unna or Miescher nevus |
Thick curved vessels in the center of |
|
skin-colored clods, occasionally no |
|
vessels visible |
Spitz nevus |
Vessels as dots |
Melanoma or metastasis of |
Vessels of all types arranged randomly |
melanoma |
|
Non-pigmented (amelanotic) lesions |
221 |
Dermatoscopic clues and clues beyond dermatoscopy
None
Dermatoscopic clues: The linear vessels are thin
Other clues: Anatomic site (most commonly occurs on palms and soles)
Dermatoscopic clues: Discrete vessels as lines or dots usually absent, Pyogenic granuloma: Thick white or skin colored intersecting lines, white or brown margin
Other clues to pyogenic granuloma: Recent history of trauma
Clinical context, distribution of lesions, history, number of lesions
Clinical context, distribution of lesions, history, number of lesions
Dermatoscopic clues: Yellow clods, ulceration Other clues: Clinical context, history, recent travel in endemic area
Clinical context, history, number of lesions
Dermatoscopic clues: Central white or skin-colored or orange clod
None
Dermatoscopic clues: Central white or yellow clods. Vessels do not cross center.
Dermatoscopic clues: Polarizing-specific white lines or reticular white lines or white structureless area in the center Other clues: Firm to the touch, "dimple sign"
Dermatoscopic clues: Structureless white zone Other clues: Firm to the touch (even firmer than dermatofibroma)
Dermatoscopic clues: Structureless white zone, dermal hemorrhage (blue structureless zone)
Other clues: Firm to the touch (even firmer than dermatofibroma)
Dermatoscopic clues: Skin-colored polygonal clods, seborrheic keratosis-like findings like white dots, yellow or orange clods
Other clues: Clinical context (usually multiple similar lesions)
Dermatoscopic clue: White or skin-colored lines Other clues: Classic non-pigmented Spitz nevi most commonly occur on the face
Dermatoscopic clue: White lines. Helical vessels or vessels as pink or red clods
Other clues: in the case of melanoma metastasis: clinical context, history, and number of lesions

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
222 Non-pigmented (amelanotic) lesions
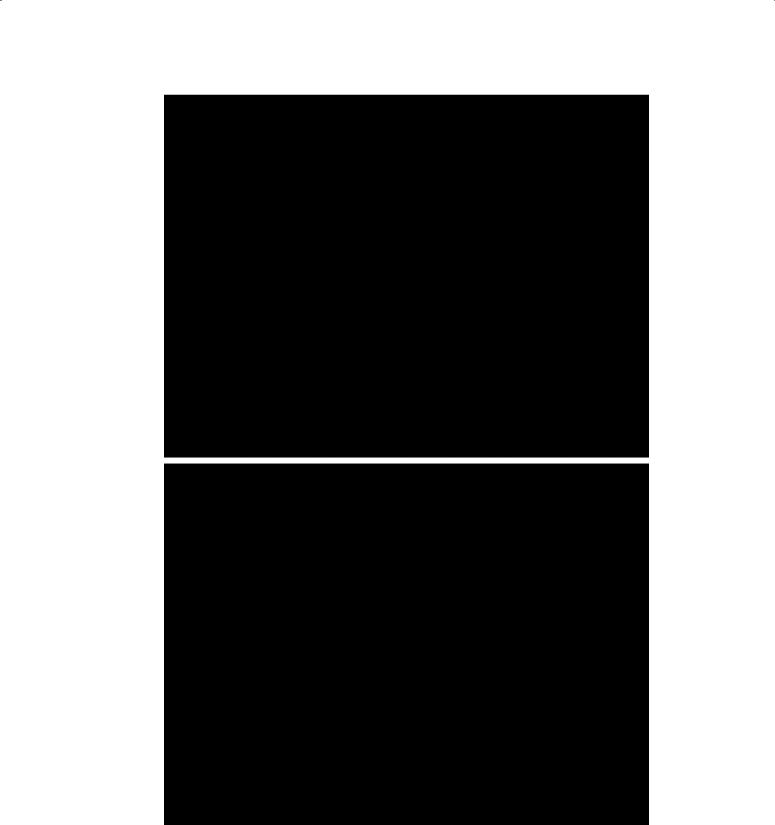
Figure 6.30: Nodular non-pigmented lesions.
Dermatoscopy right column. Top: Polymorphous vessels arranged randomly (looped vessels, coiled vessels, clods) in a squamous cell carcinoma. Middle: Serpentine and loop vessels arranged radially in a molluscum contagiosum. Bottom: Serpentine branched vessels in a melanoma metastasis.
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Non-pigmented (amelanotic) lesions |
223 |
Figure 6.31: Clear cell acanthoma.
Two clear cell acanthomas with the dermatoscopy showing the characteristic serpiginous arrangement of small coiled vessels.

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
224 Non-pigmented (amelanotic) lesions
Figure 6.32: Eccrine poroma. Eccrine poroma typically, but looped and serpentine vessels
not exclusively, occurs on acral sites like the one depicted here. On dermatoscopy (right) one can see the with coiled ends.
Figure 6.33: Trichoepithelioma.
Serpentine branched vessels are not specific for basal cell carcinoma. Trichoepithelioma is a benign neoplasm with follicular differentiation that shows serpentine branched vessels indistinguishable from those in basal cell carcinoma.
Miescher nevus or papillomatous parts of congenital nevi may show surface keratin in the epidermal invaginations. Pilomatrixoma is typified by subsurface keratin, which is characterized by a white structureless zone dermatoscopically. The subsurface keratin of epidermal cysts is hardly ever visible by dermatoscopy. Keratin may also be present in viral warts and angiokeratoma. A single central plug of keratin usually indicates a keratoacanthoma, but it is not possible to reliably distinguish between well-differentiated squamous cell carcinoma and keratoacanthoma dermatoscopically.
Blood spots in keratin are a good clue to the diagnosis of well-differentiated squamous cell carcinomas and keratoacanthomas (6.6).
While keratin is a good clue to well differentiated squamous cell carcinomas, poorly differentiated squamous cell carcinomas usually do not produce keratin.
Occasionally dermatoscopy does not permit a clear distinction between a central keratin plug and a central ulcer, particularly when a keratin plug contains bloods spots. This is an important distinction because radially arranged vessels may be found around an

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Non-pigmented (amelanotic) lesions |
225 |
Figure 6.34: Digital mucoid (myxoid) cyst.
Mucoid finger cysts may also show serpentine branched vessels on dermatoscopy (right). Any tumor underneath the superficial vascular plexus including cysts can present with serpentine branched vessels.
ulcer, regardless of the lesion’s etiology. For example, ulcerated basal cell carcinomas may show radial vessels
(6.35 top, right).
Polarizing specific white lines and white clods can be found in malignant neoplasms (e.g. basal cell carcinoma, melanoma) and in some benign conditions (e.g. dermatofibroma, Spitz nevus, pyogenic granuloma). Reticular white lines may be present in melanoma or Spitz nevi and in some dermatofibromas. As a general rule, non-pigmented nodules with white lines should be biopsied or excised unless an unequivocal benign diagnosis can be made based on clues beyond dermatoscopy.
White circles in a nodular lesion point to keratoacan- thoma/well-differentiated squamous cell carcinoma. Rarely, other lesions may show white circles, for example some basal cell carcinomas.
If ulceration, keratin and white clues are absent the specific diagnosis of nodular lesions becomes even more challenging.
In some cases, a specific vascular arrangement will help to narrow down the differential diagnosis. Three arrangements have high specificity for benign conditions, allowing these lesions to be excluded from further assessment.
The serpiginous arrangement of coiled vessels is so specific for clear cell acanthoma that no other diagnosis needs to be considered.
Linear vessels seen in the center of polygonal skin-col- ored clods is termed a centered arrangement. These vessels may be polymorphous. When this includes thick curved vessels, this is indicative of an Unna nevus or a
Miescher nevus. Centered vessels may also be found in seborrheic keratoses. The clods only pattern is specific for hemangioma. It is crucial that no vessels as lines are present as this can be a clue to malignancy.
The differential diagnoses of the other specific vessel arrangements include both benign and malignant tumors. Radially arranged vessels are found in sebaceous gland hyperplasia (additional clue: several white or yellow clods in central location), in molluscum contagiosum (additional clue: singular skin-colored or orange clod in central location) and in keratoacanthoma (additional clue: a keratin plug in central location, which may be white, yellow or orange). The radially arranged vessels in keratoacanthoma may be looped, linear, curved or branched-serpentine. The specificity of branched serpentine vessels for basal cell carcinoma is frequently overestimated. Of course basal cell carcinoma is the most common diagnosis in cases of non-pigmented nodular lesions with branched vessels, but in principle any invasive tumor in the dermis lying below the superficial vascular plexus may have this pattern of vessels. This is true for cysts, benign adnexal tumors (e.g. trichoblastoma or poroma), keratoacanthoma/ well differentiated squamous cell carcinoma and other types of neoplasms. It is true for the rare Merkel cell carcinoma, and cutaneous metastases regardless of the origin of the primary malignancy. In the absence of a confident specific benign diagnosis, non-pigmented nodules with branched serpentine vessels should be submitted for histopathology.
Eccrine poroma is characterized by a combination of coiled, serpentine and branched vessels. The peculiar
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
226 Non-pigmented (amelanotic) lesions
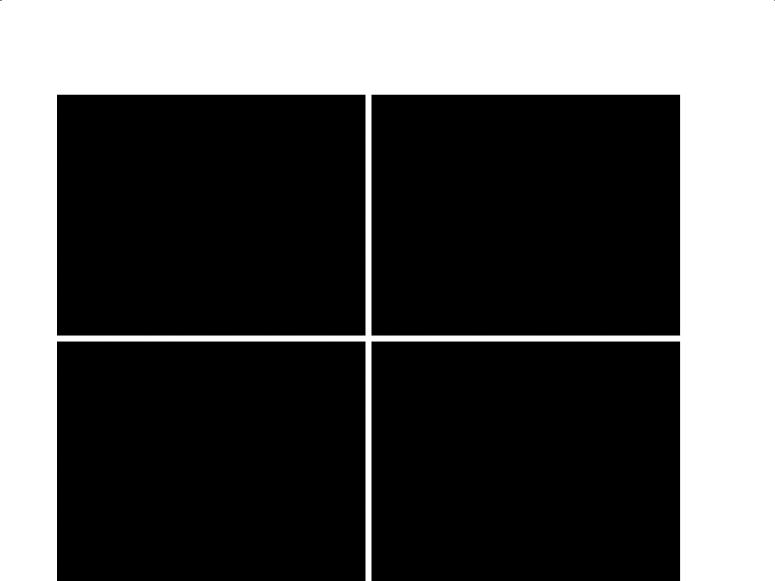
Figure 6.35: Nodular amelanotic lesions.
Top left: Keratoacanthoma with central keratin plug (with blood spots) and radial vessels. Top right: Basal cell carcinoma with radial vessels and serpentine branched vessels. The radial vessels in this basal cell carcinoma are unusual and due to ulceration. Bottom left: Polymorphous vessels without a specific arrangement in a poorly differentiated squamous cell carcinoma (note ulceration and adherent fibers). Bottom right: Polymorphous vessels without a specific arrangement in a melanoma (invasion thickness: > 1 mm). Note the presence of helical vessels.
combination of coiled and serpentine vessels evoked the metaphor of “cherry blossom” vessels (figure 6.32), which is of course dispensable.
When a melanoma occurs as a non-pigmented nodule, the vessels are usually polymorphous and randomly arranged (6.35 bottom right, 6.39 bottom, 6.40 bottom). According to Menzies (43), vessels in amelanotic nodular melanoma are often arranged in the center of the lesion. Helical vessels are not common, but when seen are quite specific for melanoma, usually primary but sometimes metastatic (6.35 bottom right). Pink or red clods, and white lines also should be viewed with caution when seen in conjunction with vessels as dots or lines.
Summary
In summary, the investigator is confronted with the limits of dermatoscopy when trying to assess non-pigmented lesions. Nevertheless, in some cases dermatoscopy may yield clues that point in the right direction – clues that may remain hidden to observation by the naked eye. Because diagnostic uncertainty is greater for non-pig- mented lesions than in pigmented ones, histopathology will be required more often to establish an accurate diagnosis. Importantly, the investigator must recognize this greater uncertainty, and avoid making decisions that exceed the limitations of the method.
We can, however, apply some simple general rules, which can be summarized into a very rudimentary
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Non-pigmented (amelanotic) lesions |
227 |
Figure 6.36: Basal cell carcinoma.
Serpentine branched vessels in a basal cell carcinoma.
Figure 6.37: Merkel cell carcinoma.
A Merkel cell carcinoma presenting as non-pigmented ulcerated nodule with serpentine branched vessels on dermatoscopy (right). Images courtesy of Jean-Yves Gourhant.
short algorithm (44). Any non-pigmented lesion that is ulcerated or has white clues (white lines in any lesion and in raised lesions, keratin, white circles or white structureless areas) should be biopsied or excised to rule out malignancy. If ulceration and white clues are absent one should try to make a specific diagnosis based on other clues (e.g. keratin, scale, yellow color, white dots etc.) and vascular patterns. If a specific benign diagnosis cannot be made with confidence the lesion should be biopsied or excised to rule out malignancy. Some examples to demonstrate the usefulness of this rule are given in figures 6.40 to 6.42.
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
228 Non-pigmented (amelanotic) lesions
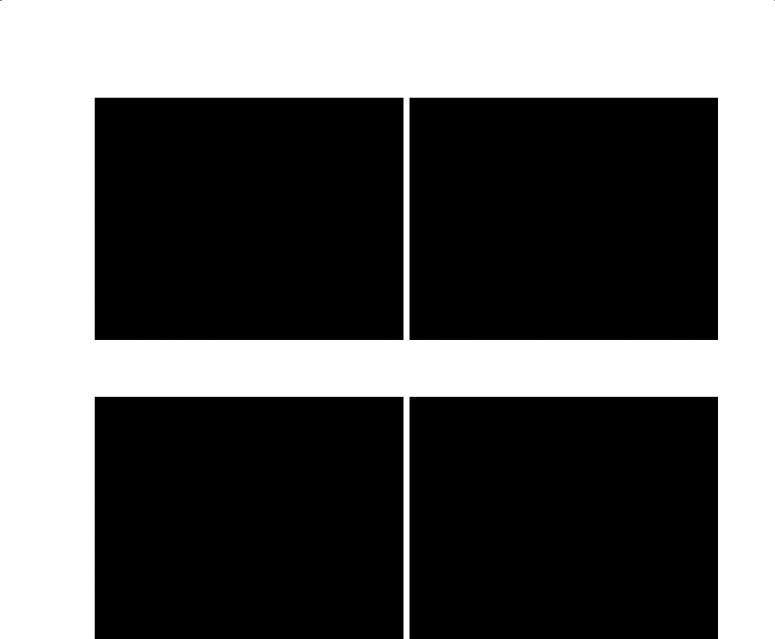
Figure 6.38: Unna nevi (“dermal nevi”).
Unna nevi often are amelanotic nodules. On dermatoscopy (top and bottom right) one can see skin colored clods. The top case shows the typical specific arrangement of linear vessels in the center of the clods.
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Non-pigmented (amelanotic) lesions |
229 |
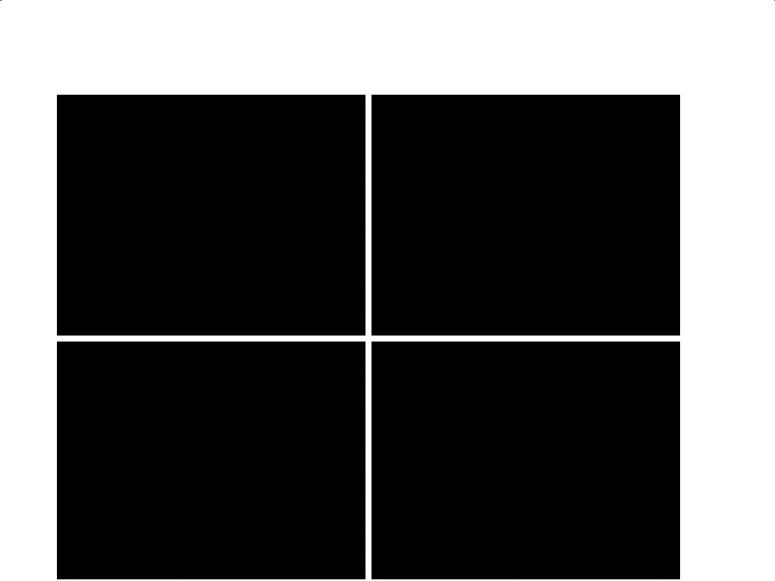
Figure 6.39: Amelanotic melanomas.
Top: This melanoma (> 1 mm) consists of a nodular and a flat portion. The nodular portion is marked by polymorphous vessels arranged randomly. The flat portion shows vessels as dots, which confirms the diagnosis of melanoma. Bottom: A nodular lesion that primarily shows vessels as dots on dermatoscopy, but also other types of vessels which do not follow any special arrangement. The hemorrhagic crust due to ulceration (seen as a single black clod) is a clue to malignancy in the absence of trauma. A further clue to melanoma is the presence of white lines. Diagnosis: Melanoma (> 1 mm).