


32 Part I – High-Fluid Content Liver Lesions
16 Mucinous Metastasis – Mimicking an Hemangioma
Colorectal mucinous carcinoma is a histopathologic subtype of rectal adenocarcinoma, which is characterized by the production of an abundant amount of extracellular mucin. The incidence of the mucinous carcinomas varies between 10 % and 20 % of the total number of colorectal carcinomas. Mucinous carcinomas are known to be highly infiltrative lesions, which lead to a lower resection rate and a higher postoperative dissemination rate. These factors lead to a poorer prognosis in patients with the mucinous as compared with non-mucinous colorectal carcinomas. Because of higher fluid than solid content with concomitant less vascularity, the liver metastases of colorectal adenocarcinomas may mimic non-solid liver lesions such as cysts and hemangiomas at imaging. Particularly, MR imaging may facilitate the distinction of mucinous liver metastases from benign non-solid liver lesions.
Literature
1.Wu CS, Tung SY, Chen PC, Kuo YC (1996) Clinicopathologic study of colorectal mucinous carcinoma in Taiwan: a multivariate analysis. J Gastroenterol Hepatol 11:77 – 81
2.Ueda K, Matsui O, Nobata K, Takashima T (1996) Mucinous carcinoma of the liver mimicking cavernous hemangioma on preand postcontrast MR imaging [letter]. Am J Roentgenol 166:468 – 469
3.Outwater EK, Tomaszewski JE, Daly JM, Kressel HY (1991) Hepatic colorectal metastases; correlation of MR imaging and pathology. Radiology 180:327 – 332
MR Imaging Findings
Because of the abundant extracellular mucin, liver metastases of mucinous colorectal adenocarcinomas typically show predominantly high to very high signal on T2-weighted MR images. On T1-weighted images, the lesions often have unremarkable low signal intensity. After injection of gadolinium, mucinous liver metastases show enhancement of the intratumoral structures, including septa and vessels, in the arterial as well as delayed phases (Figs. 16.1, 16.2). Particularly at CT the enhancement of intratumoral structures may mimic the peripheral nodular enhancement and, in combination with signs such as a traversing vessel, may suggest a benign lesion such as hemangioma (Fig. 16.3A). In our experience, positron emission tomography (PET) may show no abnormal activity and may wrongfully suggest that CT findings are correct (Fig. 16.3B). In such cases, after MR imaging an US-guided biopsy or a resection of the liver lesion may show conclusive evidence of metastasis.
Pathology
At gross pathology, the lesions appear as solid pink lesions with sharp demarcation to the surrounding liver. At histology, the lesions show large spaces filled with abundant mucin. These spaces are interspersed with large septa containing vessels (Fig. 16.3C, D).
16 Mucinous Metastasis – Mimicking an Hemangioma 33
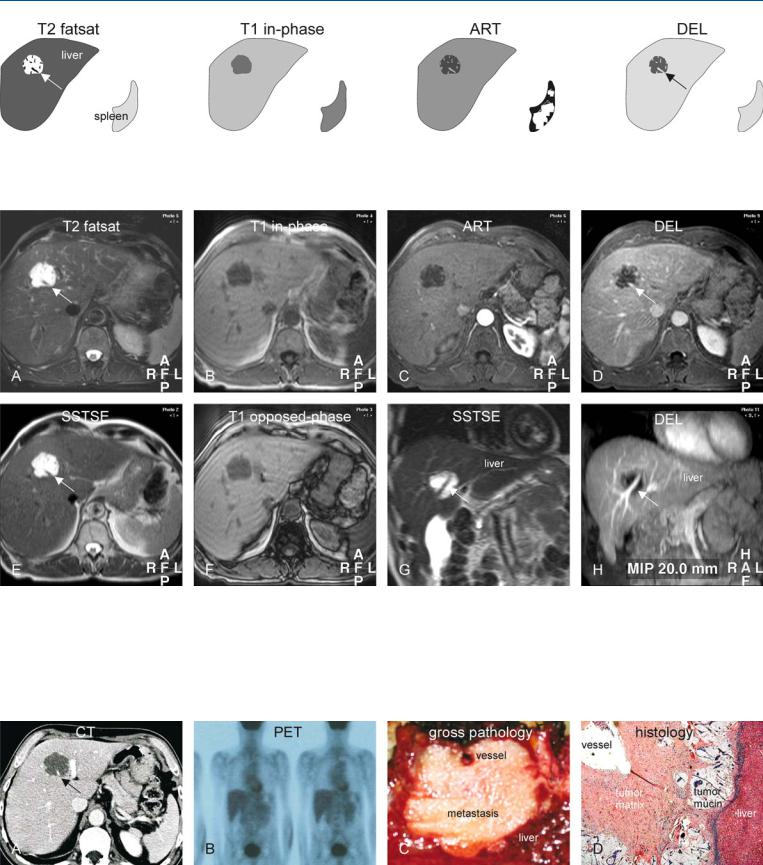
Fig. 16.1. Mucinous colorectal metastasis mimicking hemangioma, drawings.
T2 fatsat: metastasis is very bright containing low intensity structures, including a traversing vessel (arrow); T1 in-phase: metastasis is hypointense
Fig. 16.2. Mucinous colorectal metastasis mimicking hemangioma at CT: MRI findings. A Axial TSE image (T2 fatsat): Lesion is very bright and contains low intensity structures and a traversing vessel (arrow). B Axial in-phase image (T1 in-phase): Metastasis is hypointense to the liver. C Axial arterial phase image (ART): Intratumoral structures, including the vessel, show some enhancement; transversing vessel is often considered a sign of benign lesions. D Axial delayed phase image (DEL): Intratumoral structures and the
to the liver; ART: metastasis shows enhancement of low intensity structures and vessel; DEL: metastasis shows increased enhancement of the intratumoral structures and the vessel (arrow)
traversing vessel (arrow) are more enhanced. E Axial SSTSE image with a TE of 120 ms: metastasis retains its signal, which is a common finding of hemangioma and cysts. F Axial opposed-phase image (T1 opposed-phase) shows no change in the aspect of the liver, nor of the lesion. G Coronal SSTSE (SSTSE) shows metastasis with the traversing vessel (arrow). H Maximum intensity projection (MIP) of the delayed phase (DEL) provides an overview of the traversing liver vein (arrow)
Fig. 16.3. Mucinous colorectal metastasis with inconclusive CT and PET; MR-pa- thology correlation. A CT shows little enhancement, and in combination with the traversing vessel (arrow), the lesion was considered benign. B Positron emission tomography (PET) showed normal uptake in the liver. C Based on
MR imaging, the lesion was biopsied and then resected. Pathology confirmed a metastasis with a traversing vessel. D Photomicrograph shows the metastasis composed of tumor matrix, pools of mucin, and a traversing vessel. H&E stain, × 100

Part II
Solid Liver Lesions II

Part II/IIA
Solid Liver Lesions |
II |
Metastases: Colorectal |
IIA |