

Книги по МРТ КТ на английском языке / Neurosurgery Fundamentals Agarval 1 ed 2019
.pdf9.11 C1 Fractures
Fig. 9.10 Management of isolated C1 fractures. (Reproduced from Jallo J, Vaccaro A, Neurotrauma and Critical Care of the Spine, 1st edition, ©2008, Thieme Publishers, New York.)
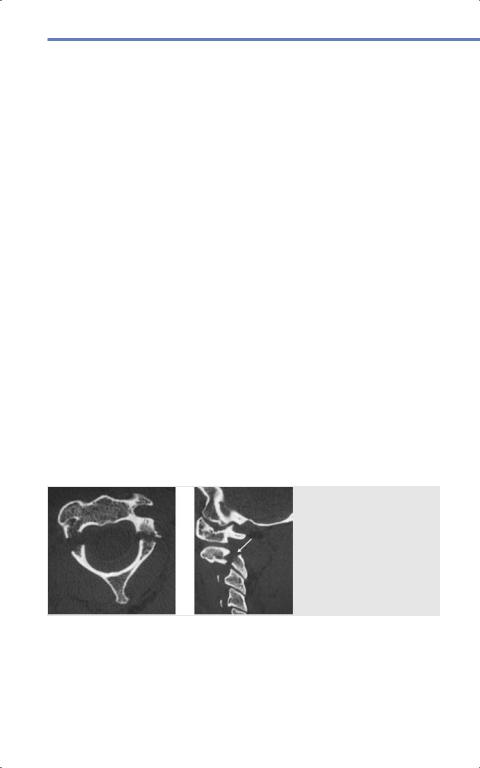
Fig. 9.11 Dens fracture types (a) Type I. (b) Type II.
(c) Type III. (Reproduced from Chapman J, Dettori J,
Norvell D, Spine Classifications and Severity Measures, 1st edition, ©2009, Thieme Publishers, New York.)
159
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.
Spinal Trauma
•Type III fractures go through the vertebral body and are generally stable. Treat with a cervical collar unless there are other injuries rendering the spine unstable.
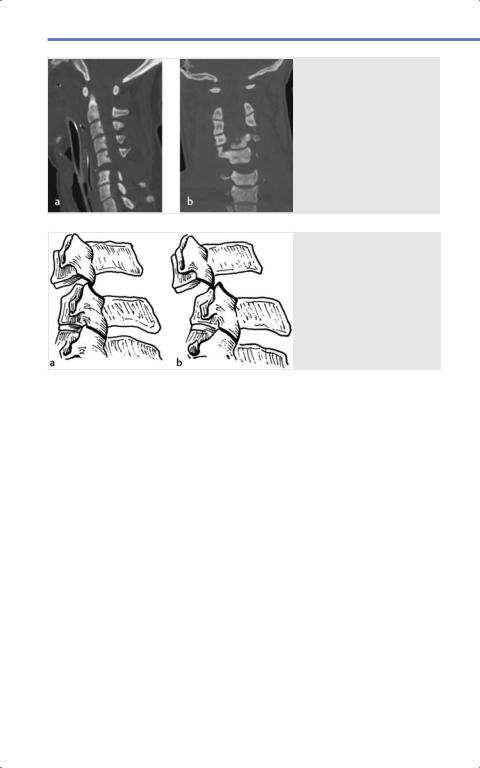
9.11.2 Hangman’s Fractures
•Vertical or oblique fractures through the C2 pars interarticularis, disconnecting the posterior arch from the vertebral body as shown in Fig. 9.12.22
•Usually caused by hyperextension (MVA or diving injury); the posterior C1 ring and C2-C3 disc should also be evaluated for injury.
•Most isolated fractures can be managed with a collar; displaced, isolated fractures can be managed with a halo brace.
•Surgery may be indicated if the C2-C3 facets are locked or the patient has other injuries rending the spine unstable.
9.11.3 Other C2 Fractures
•Isolated, nondisplaced fractures of the C2 lamina, vertebral body, and facets are generally stable and heal in a collar.22
•C2 fractures seen in combination with
C1 fractures require careful evaluation for spinal stability.
9.11.4 Subaxial Cervical
Spine Injuries
•The most commonly injured level is C5-C6.19
•The three kinds of injuries are compression, flexion/extension/ distraction, and rotation ( Table 9.3).
•The table includes bony (fracture) and ligamentous (whiplash) injuries.Fig. 9.13 shows a severe fracturedislocation injury.
9.11.5 Jumped Facets
•Jumped facets can result in severe injury to the spinal cord and nerve roots.19
•The facets may be perched or frankly locked depending on the severity of injury.
•Unilateral injuries can occur when the spine is rotated. Bilateral injuries usually result from flexion or extension that disrupts the posterior ligaments.Fig. 9.14 shows perched and locked facet injuries in the cervical spine.
Fig. 9.12 Hangman’s fracture involving the bilateral C2 pars. (Reproduced from
Meyers S, Differential
Diagnosis in Neuroimaging: Spine, 1st edition, ©2016, Thieme Publishers,
New York.)
160
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.
9.11 C1 Fractures
Table 9.3 Classification of cervical injuries
Compression
Flexion/Extension/Distraction
Injury |
Mechanism |
Stability and Treatment |
Anterior com- |
Axial loading |
Stable. |
pression (wedge |
+/- flexion/extension |
Generally heal with external |
fracture) |
|
immobilization |
Comminuted |
Axial loading |
Generally unstable. |
fracture (burst |
+/- flexion |
Treat with fusion, and |
fracture) |
|
decompression if needed |
Teardrop fracture |
Hyperflexion- |
Unstable—evaluate disc space |
|
compression |
and ligaments on MRI. |
|
|
Treat with fusion, decompress |
|
|
if needed |
These injuries below are unstable if the PLL/posterior annulus fails AND there is anterolisthesis, facet malalignment, end plate angulation > 10 degrees, or vertebral segment distraction
Whiplash with |
Flexion/extension |
Stable. |
neurologic injury |
|
Management is controversial |
|
|
and can include collar and |
|
|
physical therapy |
Severe whiplash |
Flexion/extension |
Re-evaluate integrity of poste- |
(sprain) |
|
rior ligaments; treat with collar, |
|
|
physical therapy |
Bilateral facet |
Distraction + flexion/ |
Unstable: Closed or open |
fracture-dislocation |
extension with failure |
reduction and internal fixation/ |
|
of posterior ligamen- |
fusion. |
|
tous complex |
Evaluate for herniated discs |
|
|
with MRI |
Unilateral facet |
Lateral flexion |
Stable if there is no significant |
fracture |
+ rotation |
subluxation, dislocation, or |
|
|
kyphosis. |
|
|
Treat with collar |
Fracture separation |
Extension, |
Evaluate for other injuries to |
of articular pillar |
compression, |
determine if stable. |
|
+ rotation |
Treatments include collar, halo, |
|
|
surgery. |
Unilateral |
Lateral flexion |
A perched facet is unstable. |
dislocation |
+ rotation |
Evaluate for nerve root and |
|
|
cord injury. |
|
|
Treatments include reduction |
|
|
and halo or fusion. |
Abbreviations: PLL, posterior longitudinal ligament.
161
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.
Spinal Trauma
•The bony injury needs to be reduced.
◦Unilateral injuries may be reduced in traction and then a halo or surgical fusion.
◦Closed traction is controversial in bilateral injuries. Generally, patients will need surgery, with either an anterior or posterior approach and intraoperative reduction.
◦Some surgeons prefer to get an MRI before reduction, to evaluate for disc herniations.19
9.12 Additional Principles for Cervical Trauma
•Unless atlanto-occipital dislocation is present (i.e., the transverse ligament is torn in its midportion) most isolated
162
Fig. 9.13 Fracture-dis- location injury at C5–C6. (Reproduced from Fehlings M, Vaccaro A, Boakye M et al, Essentials of Spinal
Cord Injury, Basic Research to Clinical Practice, 1st edition, ©2012, Thieme Publishers, New York.)
Fig. 9.14 (a) Perched.
(b) Locked facets. (Reproduced from Benzel E, Biomechanics of Spine Stabilization, 3rd edition, ©2015, Thieme Publishers, New York.)
ligamentous injuries can be managed with a cervical collar alone. Follow-up in 4–6 weeks and evaluate range of motion and cervical tenderness.
•Patients with rheumatoid arthritis, Down syndrome, ankylosing spondylitis, and other conditions predisposing them to cervical instability require imaging and careful examination following trauma.
•Patients with hardware from previous cervical spine surgery need careful evaluation. X-rays, CT, and CT myelograms are useful imaging options. MRI is necessary to evaluate the spinal cord, but evaluation of the bones may be limited by artifact.
•Plain radiographs will not show the C7-T1 disc space and facets well; if there is concern for a junctional injury CT and/or MRI are necessary.
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.
9.14 Thoracolumbar and Lumbar Spine Injuries
9.13 Thoracic Injuries
•The spinal cord generally ends at L1-L2, with the cauda equina filling the distal canal.
•Significant force is needed to fracture the thoracic vertebrae. However, the canal is narrow and thus the cord vulnerable to injury from retropulsed or dislodged fragments.19
•Lesions above this level can result in complete or incomplete paraplegia and bowel/bladder problems with typical upper motor neuron findings.
•Injuries below may involve different nerve roots and show lower motor neuron findings.
•Conus medullaris syndrome can occur with T12-L1 injury. Damage to the sacral nerve roots results in bowel and bladder problems. Some of the lumbar nerve roots may be intact.
•The three-column approach to evaluating spinal stability is discussed below in the next section and useful for evaluating these injuries.
9.14 Thoracolumbar and
Lumbar Spine Injuries
Along with his three-column model for determining spinal stability, Denis classified spine injuries into minor injuries— articulating process, transverse process, spinous process, and pars interarticularis fractures, and major injuries—compres- sion, burst, seat-belt type fractures, and fracture-dislocations.12,13,14,15 These terms can be used for thoracic and lumbar spinal injuries, and the major injuries are shown in Fig. 9.5.
•Minor injuries are generally stable, but patients should be evaluated for other injuries.
•Compression fractures and burst fractures may be stable, depending on the integrity of the ligaments.
•Seat-belt type injuries and fracture dislocations are generally unstable.
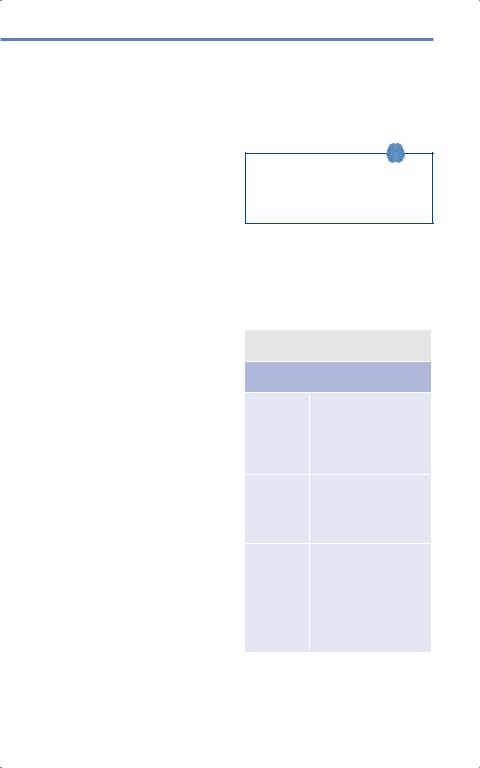
The Spine Trauma Group put forth the Thoracolumbar Injury Classification and Severity Score (TLICS) to help guide treatment. See Table 9.4 below.
Patients with a TLICS score of less than 4 can usually be treated nonoperatively; score equal to 4 may be treated operatively or nonoperatively; a score of greater than 4 usually warrants operative management.23,24
Table 9.4 The Thorocolumbar Injury
Classification and Severity scoring system
Thorocolumbar Injury Classification
and Severity (TLICS) Score
Morphology |
Compression: 1 point |
|
Burst: 2 points |
|
Translation/rotation: 3 |
|
points |
|
Distraction: |
|
4 points |
Posterior |
Intact: 0 point |
ligamentous |
Suspected or |
complex |
indeterminate injury: |
|
2 points |
|
Injured: 3 points |
Neurologic |
Intact: 0 point |
involvement |
Nerve roots: 2 points |
|
Cord/conus medulla- |
|
ris (incomplete): 3 points |
|
Cord/conus (complete): |
|
2 points |
|
Cauda equina: |
|
3 points |
163
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.
Spinal Trauma
9.14.1 Compression
Fractures
•Occur when the anterior column fails.
•The middle column is intact, so it can serve as a hinge.
•The posterior column may fail, depending on the forces involved.
•Injuries involving more than one column may be unstable.
9.14.2 Burst Fractures
Denis also broke thoracolumbar burst fractures into five categories, shown inTable 9.5. Purely bony injuries can be managed conservatively in select cases; however, patients who cannot or will not tolerate a brace may get better results with surgery. In two level injuries, the bone or disc of the middle column is injured. These patients may require surgery.
9.14.3 Seatbelt Type Injuries
•In a seatbelt type injury, the middle and posterior columns fail when the patient is severely flexed.
•Patients usually present as restrained occupants in a MVA. The anterior column acts like a hinge, and may be injured as well.
•The spine is unstable in flexion.
•One level injuries may present as a Chance fracture, which is a fracture through the vertebral body and neural arch, or as a disruption of the disc and PLL.
9.14.4 Fracture Dislocations
•These occur when all three columns fail.
•The mechanism of injury can vary— compression, tension, rotation, or shear.
•Most of these injuries require surgery.23
Table 9.5 Denis classification of burst fractures11,12,13,14
Type |
Elements involved |
Typical cause(s) and site(s) |
A |
Fracture of both endplates without |
Pure axial load; usually lumbar spine |
|
kyphosis. Bone may be retropulsed into |
|
|
the canal |
|
B |
Fracture of superior endplate |
Axial load and flexion; usually thora- |
|
Most common |
columbar junction |
C |
Fracture of the inferior endplate |
Axial load and flexion; no particular |
|
|
sites commonly involved |
D |
Burst rotation fracture with comminution |
Axial load and rotation; mid-lumbar |
|
of the vertebral body, possible laminar |
spine |
|
fractures, and bone retropulsed into canal |
|
E |
Burst lateral flexion with fractured |
Axial load and lateral flexion |
|
posterior wall of the vertebral body and |
|
|
extrusion towards the side of the flexion |
|
164
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.
9.16 Top Hits
9.15 Sacral Fractures
These are less common and are often caused by shear forces.24 They can injure sacral roots, plexus, and affect pelvic and spinopelvic stability. Injuries below S2 should not affect ambulation, but may be unstable and cause pain that improves after surgical fixation. More medial fractures have higher instances of neurologic injury and worse outcomes.
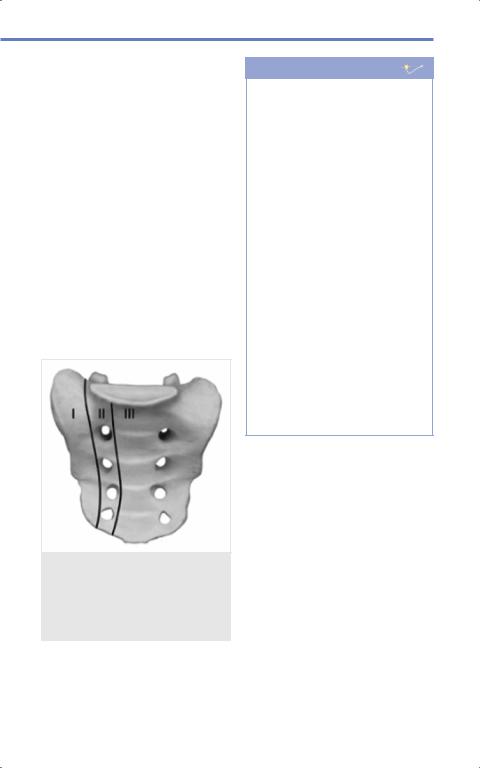
Fig. 9.15 outlines the three zones into which Denis divided the sacrum.
•Zone 1: Lateral to the neural foramina.
•Zone 2: Through the neural foramina.
•Zone 3: Central canal.
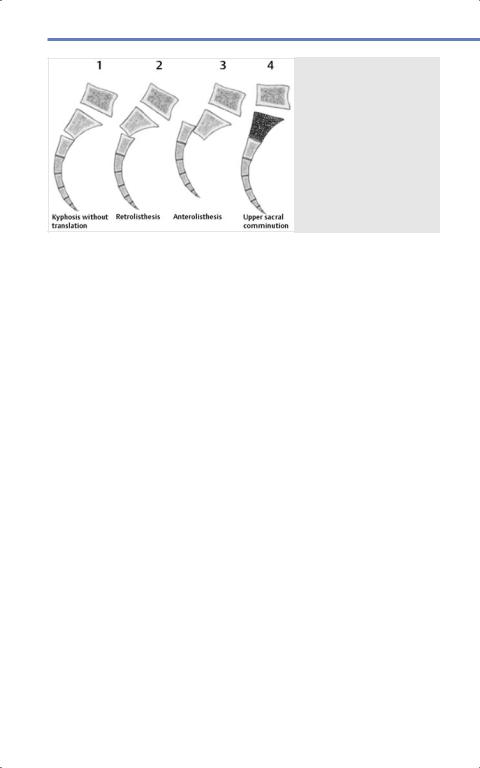
Roy and Camille also presented another schematic to evaluate Zone 3 fractures. It was later modified by Strange-Vognsen and Lebech, as in Fig. 9.16.
Fig. 9.15 The Denis classification of sacral fractures. (Reproduced from Vialle L, AOSpine Masters Series, Volume 6: Thoracolumbar Spine Trauma, 1st edition, ©2015, Thieme Publishers, New York.)
Pearls
•Remember the ABCs of resuscitation. Look for life-threatening injuries in patients with significant spine injuries. Patients in spinal and/or hemorrhagic shock need aggressive treatment and careful monitoring. Avoid hypotension in patients with spinal cord injuries.
•Make sure to perform a thorough neurological examination on any patient with suspected spine trauma. These findings will guide your decision to image the patient.
•Take extra caution when evaluating patients with spinal hardware or conditions predisposing them to cord compression and serious neurological injury.
•There are a multitude of conditions that make individuals more susceptible to major spine injury from a seemingly trivial injury. When a patient presents with an injury that seems out of proportion to the mechanism, obtain imaging promptly and consider these and other predisposing conditions.
9.16 Top Hits
9.16.1 Questions
1.An elderly man with a history of untreated cervical stenosis falls down the stairs and immediately complains of numbness and tingling in his hands and weak grip. What is the most likely diagnosis?
a)Unilateral jumped facet
b)Central cord syndrome
c)Atlanto-axial subluxation
d)Compression fracture of the C6 vertebra
165
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.
Spinal Trauma
2.A 25-year-old man is extricated from a burning vehicle and arrives to the hospital unconscious, intubated, and with a cervical collar in place. Initial CT head and cervical spine are negative. His injuries include lower extremity fractures requiring orthopedic surgery and a pneumothorax requiring a chest tube. He is stabilized, extubated, and awake and alert 2 days later. What is the best way to assess the need for his cervical collar?
a)Confrontational examination only
b)Flexion-extension films only
c)Confrontational examination and MRI
d)Repeat CT
3.Which of the following injuries will most likely require operative intervention?
a)A unilateral facet fracture at C4-C5 with intact ligaments on MRI
b)Unilateral transverse process fractures at L2 and L3
c)An isolated C7 superior endplate fracture
d)Bilateral facet fractures at C4-C5
166
Fig. 9.16 Further classification of Denis type 3 sacral fractures. (Reproduced from Vialle L, AOSpine Masters Series, Volume 6: Thoracolumbar Spine Trauma, 1st edition, ©2015, Thieme Publishers, New York.)
9.16.2 Answers
1.b. This is a classic presentation of central cord syndrome. Patients present with distal greater than proximal deficits, and many have pre-existing cervical stenosis.
2.c. The patient cannot undergo a confrontational examination alone, as he has other painful injuries. Any pain on confrontation may indicate ligamentous injury, which can be confirmed or ruled out on an MRI at this point.
3.d. Bilateral facet fractures result in an unstable spine and the patient will need instrumentation to restore stability.
References
[1]Fawcett JW, Curt A, Steeves JD, et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord. 2007; 45(3):190–205
[2]Hoffman JR, Wolfson AB, Todd K, Mower WR.
Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiog- raphy Utilization Study (NEXUS). Ann Emerg Med. 1998; 32(4):461–469
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.

9.16 Top Hits
[3]Theodore N, Hadley MN, Aarabi B, et al. Prehospital cervical spinal immobilization after trauma. Neurosurgery. 2013; 72Suppl 2:22–34
[4]Khan MF, Burks SS, Al-Khayat H, Levi AD. The ef- fect of steroids on the incidence of gastrointestinal hemorrhage after spinal cord injury: a casecontrolled study. Spinal Cord. 2014; 52(1):58–60
[5]Hurlbert RJ. Methylprednisolone for acute spinal cord injury: an inappropriate standard of care. J Neurosurg. 2000; 93(1), Suppl:1–7
[6]Lauweryns P. Role of conservative treatment of cervical spine injuries. Eur Spine J. 2010; 19Suppl 1:S23–S26
[7]Weiss N. Application of closed spinal traction. In: Atlas of Emergency Neurosurgery. New York, NY: Thieme; 2015:170–178
[8]Schneider RC. The syndrome of acute anterior spinal cord injury. J Neurosurg. 1955; 12(2):95– 122
[9]Management of Acute Traumatic Central Cord Syndrome. Contemporary Spine Surgery. 2016; 17(10):1–8
[10]Ishida Y, Tominaga T. Predictors of neurologic recovery in acute central cervical cord injury with only upper extremity impairment. Spine. 2002; 27(15):1652–1658, discussion 1658
[11]Beer-Furlan AL, Paiva WS, Tavares WM, de Andrade AF, Teixeira MJ. Brown-Sequard syndrome associated with unusual spinal cord injury by a screwdriver stab wound. Int J Clin Exp Med. 2014; 7(1):316–319
[12]Denis F. Updated classification of thoracolumbar fractures. Orthop Trans. 1982; 6:8–9
[13]Denis F. The three column spine and its signifi- cance in the classification of acute thoracolumbar spinal injuries. Spine. 1983; 8(8):817–831
[14]Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin Orthop Relat Res. 1984(189):65–76
[15]Denis F, Armstrong GWD, Searls K, Matta L. Acute
thoracolumbar burst fractures in the absence of neurologic deficit. A comparison between oper- ative and nonoperative treatment. Clin Orthop Relat Res. 1984(189):142–149
[16]Shahan CP, Croce MA, Fabian TC, Magnotti LJ. Impact of continuous evaluation of technology and therapy: 30 years of research reduces stroke and mortality from blunt cerebrovascular injury. J Am Coll Surg. 2017; 224(4):595–599
[17]Al-Harthy A, Al-Hinai A, Al-Wahaibi K, Al-Qadhi
H. Blunt cerebrovascular injuries: a review of the literature. Sultan Qaboos Univ Med J. 2011;
11(4):448–454
[18]Leonard JC, Kuppermann N, Olsen C, et al; Pedi- atric Emergency Care Applied Research Network. Factors associated with cervical spine injury in children after blunt trauma. Ann Emerg Med. 2011; 58(2):145–155
[19]Okonkwo DO, Oskouian RJ, Shaffrey CI. Manage- ment of cervical injuries. In: Neurotrauma and Critical Care of the Spine. New York, NY: Thieme; 2009:126–142
[20]Öner FC. Spinal injury classification systems.
In: Neurotrauma and Critical Care of the Spine. New York, NY: Thieme; 2009:45–67
[21]Yang SY, Boniello AJ, Poorman CE, Chang AL, Wang S, Passias PG. A review of the diagnosis and treatment of atlantoaxial dislocations. Global Spine J. 2014; 4(3):197–210
[22]Dickman CA, Greene KA, Sonntag VKH. Traumatic injuries of the craniovertebral junction. In: Surgery of the Craniovertebral Junction. 2nd ed. New York, NY: Thieme; 2012:116–133
[23]Rajasekaran S, Kanna RM, Shetty AP. Management of thoracolumbar spine trauma: An overview. Indian J Orthop. 2015; 49(1):72–82
[24]Bellabarba C, Bransford RJ. Spinopelvic fixation.
In: AOSpine Masters Series, Volume 6: Thoracolumbar Spine Trauma. New York, NY: Thieme; 2015
167
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.

10 Spine
Robert F Heary, Raghav Gupta, Georgios A Maragkos, Justin M Moore
10.1 Introduction
Nontraumatic spine diseases affect millions of people around the world. These can include common age-related degenerative diseases of the cervical, thoracic, and lumbar spines which may present with pain, functional deficiencies, and/or neurological symptoms. Other pathologies include vascular, neoplastic, and/or infectious lesions which can lead to pain from instability or can compress the neural elements leading to symptoms of spinal cord or nerve root compression. In the present chapter, we have provided an overview of these various conditions and outlined their pathophysiology, clinical and radiographic presentations, available treatment options, and clinical outcomes.
10.2 Cervical Spine Degenerative Disease
Degenerative conditions of the cervical spine are prevalent and affect nearly two-thirds of the population at some time during their lifetime leading to neck pain and neurological symptoms in a subset of these patients.1 The baseline prevalence of radiographically-deter- mined cervical disc degeneration, for example, has been previously reported to be 21.7%.2 While most degenerative conditions of the cervical spine follow a benign clinical course, they can also result in compression of the neural elements leading to myelopathy and/or radiculopathy in addition to local mechanical neck pain.
10.3 Degenerative Cervical Myelopathy
Nontraumatic degenerative cervical myelopathy is the most common cause of spinal cord pathology among the elderly and it is estimated to have a prevalence of 605 per million individuals in North America alone.3,4 These degenerative changes can be subdivided into osteoarthritic (spondylotic) and nonosteoarthritic changes though both types can ultimately lead to symptomatic spinal cord compression or myelopathy. The various subtypes of degenerative cervical myelopathy are considered in the sections below.
10.3.1 Cervical
Osteoarthritis Degenerative Disc Disease
The intervertebral disc, which is an avascular fibrocartilaginous structure,5 is comprised of an outer annulus fibrosus and the inner nucleus pulposus both of which contain poorly vascularized cells. The former contains fibrocyte-like cells and the latter contains chondrocyte-like cells. Proteoglycans and collagen fibers comprise the extracellular matrix (ECM) in which these cells are suspended. The disc structure allows for the radial redistribution of compressive forces that would otherwise be transmitted longitudinally. However, over time, with excessive or repetitive use, trauma, and/or the influence of genetic or environmental factors, disc degeneration can occur.4 Guiot et al have reported that compromised diffusion of
168
Agarwal, Neurosurgery Fundamentals (ISBN 978-1-62623-822-0), copyright © 2019 Thieme Medical Publishers. All rights reserved. Usage subject to terms and conditions of license.