

Mesenchymal stem cells
Mesenchymal stem cells (MSCs) are multi-potent cells with a strong capacity for self-renewal. They are capable of multilineage differentiation into mesoderm-type cells such as osteoblast, adipocyte, chondrocyte and possibly, but still controversial, other non-mesoderm type cells, for example, neuronal cells or hepatocytes. (Abdallah et al., 2008) (Figure 8)
They can be isolated from a variety of tissues, such as bone marrow, adipose tissue, umbilical cord, and umbilical cord blood. MSCs have the ability to differentiate into a variety of cell types, depending on cues from their microenvironment. MSCs are identified by the expression of many molecular markers, such as: CD105, CD73 and are negative for the hematopoietic markers CD34, CD45, CD14. (Daminici et al., 2006)
An important property of MSCs is their capacity for migration and homing in or around the zones damaged by ischaemia, inflammation, and trauma or tumour sites. Understandably, the efficacy and time course of cell invasion into the damaged tissues depends upon the route of transplantation. (Kholodenko et al., 2013)
MSCs have great potential as therapeutic agents, since they can be obtained fairly effortlessly and can be rapidly expanded ex vivo for autologous transplantation, according to Dharmasaroja et al, (2009).
Figure 8 Variety of tissue types msCs have the potential to differentiate into, depending on signals produced by the local physiological environment. (Kishk et al., 2010)
MsCs for treatment of stroke
MSC therapies include cell delivery via intravenous, inta-arterial, or intracerebral injections.
To attain maximum cell concentration in the area supplied by a particular artery, intra-arterial infusion is very effective, yet it is invasive, as at least minor surgery is needed for access, which may cause blockage of local capillaries with transplanted cells.
For intracerebral injections anaesthesia and surgery are also required and the MSCs are transplanted directly into the damaged are of the brain, which is invasive and can interrupt the blood brain barrier. (BBB) For clinical use, it is best that an open blood brain barrier and access to penubra are available for intravenous delivery of MSCs to occur, which makes it necessary to control the timing of therapy. (Borlongan et al., 2011). Intra-venous stem cell administration is considered safer, than site directed transplantation, because it is widely available, multiple doses of stem cells, even high doses, can be injected for a long time at certain intervals and no contraindications, due to absence of surgical intervention have been identified. Nevertheless, not all IV injected cells transmigrate and reach the site of injury, but only a small number of them.
Despite its limitations, many studies have demonstrated that intracerebral MSC delivery showed effective engraftment, especially in inflammatory conditions. MSCs transplanted into the brain have been demonstrated to promote functional recovery by producing trophic factors that induce survival and regeneration of host neurons, as well as alter the gap junction coupling between astrocytes, allowing them to respond more effectively to damage (Li and Chopp, 2009).
The primary trophic property of MSCs is the secretion of growth factors and other chemokines to induce cell proliferation. MSCs express mitogenic proteins such as: transforming growth factor-alpha (TGF-α), TGF-β, hepatocyte growth factor (HGF), epithelial growth factor (EGF), basic fibroblast growth factor (FGF-2) and insulin-like growth factor-1 (IGF-1). (Table 1)(Murphy et al., 2013).
Benefits of MSCs in the ischemic brain include: transdifferentiation, induction of neurogenesis and angiogenesis, neuroprotection, and activation of endogenous neurorestorative processes, as well as decrease apoptosis, reduce levels of free radicals, encourage synaptic connection from damaged neurons and regulate inflammation, primarily through paracrine actions(Figure 10) (Nanette Joyce et al, 2010).
P
Table 1 Trophic, immunomodulatory and antimicrobial factors sectered by activated MSCs(Murphy et al., 2013).
arekkadan et al.,(2010) and Chen et al., (2001) Conclude that although the benefits of MSCs are undeniable, the homing of MSC to brain infarcted sites is far from ideal.Trophic effects |
Immunomodulatory effects
|
Antimicrobial effects |
Anti-scarring: KGF, SDF-1, Mip-1α and 1β Anti-Apoptotic: STC-1, SFRP2, TGF-β1, VEGF, HGF Angiogenic: TGF-β1, VEGF Mitogenic: TGF-β, TGF-α, HGF, IGF-1, FGF-2, EGF.
|
IL-6, IL-8, IL-10, IL-1RA, PGE2, IDO, HGF, TSG-6, STNF-R, NO, sHLA-GS, TGF-β1 |
LL-37, IDO |
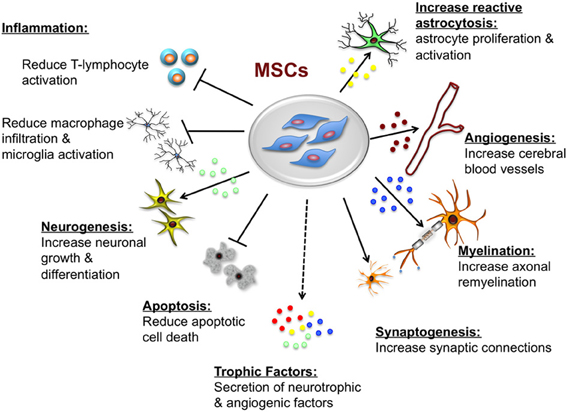
Figure 13 Potential neuroprotective and neurorestorative effects of mesenchymal stem cells. (Castillo-Melendez et al., 2013)