

Prognosis.
Any functional derangement will tend to improve for up to two years after surgery. Failure of the track to heal may result from residual infection, which may require examination under anesthesia; excess granulation tissue, which may need to be cauterized with silver nitrate or curetted; or ingrowth of hair resulting from lack of shaving. Crohn’s disease should also be excluded. The two crucial outcomes of fistula surgery are anal sphincter function and recurrence of the fistula. Of those in whom the sphincter had been preserved, 83 per cent had full continence whereas only 32 per cent of those who had undergone sphincter division were fully continent, and some of these needed a subsequent sphincter repair.
UNIT: COLOPROCTOLOGY
Theme: SACROCOCCYGEAL PILONIDAL SINUS (DISEASE)
KEY QUESTIONS FOR HOMEWORK:
Definition, location and aetiology.
Pathology.
Clinical features.
Differential diagnosis.
Treatment.
Recurrent pilonidal sinus.
1. Definition, location and aetiology.
Pilonidal sinus (Latin: pilus = hair, nidus = nest) is an acquired disease due to obstruction of hair follicles in the natal cleft, often associated with ingrowth of hair. Subcutaneous hair acts as a foreign body, initiating a reaction which is often complicated by varying degrees of infection. By reason of the shearing action of the buttocks or by sitting on a hard seat, and especially by vibration of a vehicle, loose hair travels down the intergluteal furrow, to penetrate the skin or the open mouth of a sudoriferous gland, such glands being more active in early manhood. It is not yet clear whether the initial entry of hairs through the skin is a primary event, or follows the softening of the skin due to pustular or other forms of dermatitis. Once a sinus has formed, intermittent negative pressure of the area may suck other loose hairs into the pit. Now is also proved congenital origin of the pilonidal sinus. The sinus is pit lined with epithelium and sometimes containing hair. It is centrally placed in area of the the intergluteal furrow and 4 to 8 cm cephalad to the anus. When the pilosebaceous follicle has been obstructed a cavity lined with granulation tissue forms, with the subsequent development of secondary tracks; these may rupture lateral to the midline creating secondary openings. Pilonidal disease affects young adults after puberty and is unusual after the age of 40. Males with this condition outnumber females by 4 to 1. The condition rarely occurs in blonds; many of the patients are exceptionally hairy and are usually obese. Patients have often poor personal hygiene. The epidemic of pilonidal disease is seen in American military personnel during the Second World War among jeep riders that it became known as «jeep drivers’ disease».
2. Pathology. The sinus extends into the subcutaneous planes as an infected track. Branching side channels are not infrequent. A stratified squamous epithelial lining, of varying degrees of integrity, is found in about half the cases. Hair shafts are found either lying loose in the sinus, embedded in granulation tissue, or deep in mature scar tissue in three-quarters of the cases. Foreign-body giant cells are common.
3. Clinical features.
There is a chronic or recurring sinus in the midline about the level of the first piece of the coccyx. Typically, a tuft of hairs projects from its mouth. The discharge from the sinus or sinuses is often bloodstained, contains foul sebum, and sometimes hairs. The primary sinus may have one, or as many as six openings, all of which are strictly in the midline between the level of the sacrococcygeal joint and the tip of the coccyx. Secondary openings may be present on either side of the midline, often far out on to the buttocks or in the perineum. As has been indicated already, symptoms usually commence during the third decade; patients presenting later in life nearly always give a history dating back to this period.
Clinical features of the pilonidal abscess.
In all cases, it is important to establish whether there is a history of previous episodes of the pilonidal abscess and how these were treated. Often there is a history of repeated abscesses in the region that have discharged spontaneously or have been incised. Pain is a prominent initial feature of the pilonidal abscess, followed by local signs of inflammation. In the case of a abscess, there is a localized, fluctuant, red, hot, and tender swelling placed in area of the the intergluteal furrow and 4 to 8 cm cephalad to the anus.
4. Differential diagnosis.
The sinus is not necessarily pilonidal. It could be a sinus connected with a postanal dermoid or a sinus resulting from a persistent caudal remnant of the original neural canal. The latter occurs in the sacral rather than the coccygeal region, and is definitely connected with the spinal theca. On this account, meningitis from an extradural abscess may occur in a child. Unlike a fistula in ano, the sinus passes upwards and forwards towards the sacrum. It does not reach bone, but ends blindly near the bone.
5. Treatment.
The patient is placed on the operating table, for preference in the «jack-knife» position. Methylene blue is injected into the sinus to colour all the tracks, the nozzle of the syringe being pressed against the opening to obtain some pressure. Excise all the tracks, as stained by blue dye and using sutures.The wound is closed with three or four deeply placed mattress sutures or Donati’s sutures, which are introduced about 1 cm away from the skin edges, and pass right through the fat to the level of the sacral fascia. The sutures are removed after 1 week. If the wound becomes obviously infected during this period, the sutures are removed earlier. Immediately after operation, the patient should avoid sitting on the wound. Preventing further ingrowth of hair whilst the wound remains immature is important, and the patient is advised to keep the area scrupulously clean and free of hair by the use of depilating agents or by shaving.
Treatment of an acute exacerbation (abscess). It is advisable to administer a perioperative bolus of a broad spectrum antibiotic, active against aerobic and anaerobic bacteria. A abscess should be treated in a timely fashion by incision and drainage. The abscess should be opened through a comparatively small incision. Drainage of the abscess under general or local anaesthetic rapidly relieves pain.
6. Recurrent pilonidal sinus. Three possibilities account for this disappointment:
a diverticulum of the main channel has been overlooked at the primary operation;
new hairs enter the skin or the scar;
when the natal fold is deformed by scarring, the least trauma causes tearing of the scar, and the resulting crevice becomes contaminated with coliform and cutaneous bacteria.
TESTS
1. Commonest type of anorectal
abscess is -
Ischiorectal
Submucous
Pelvirectal
Perianal
2. Deep type of anorectal
abscess is -
Ischiorectal
Submucous
Pelvirectal
Perianal
3. Superficial types of anorectal
abscesses are -
Ischiorectal
Submucous
Pelvirectal
Perianal
4. Anorectal abscesses is caused by -
Nonspecific infection of cryptoglandular origin
Specific infection
Viral infection
Pseudomonas
5. The treatment of choice in fistula in
anus -
Anal dilatation
Fissurotomy
Fistulectomy
Fistulotomy
6. The most common complication of pilonidal sinus (disease) is –
Bleeding
Perforation
Abscess
Stricture formation
7. Five-day self subsiding pain is diagnostic of -
Anal fissure
Fistula-in-ano
Thrombosed external hemorrhoids
Thrombosed internal hemorrhoids
8. The treatment of choice in pilonidal sinus (disease) without complications is –
Incision and drainage
Excision
Medical therapy
9. The treatment of choice in pilonidal abscess is –
Incision and drainage
Excision
Medical therapy
10. The treatment of choice in anorectal abscess is –
Incision and drainage
Excision
Medical therapy
ANSWERS
Вопрос |
Ответ |
1 |
d |
2 |
c |
3 |
a,b,d |
4 |
a |
5 |
c |
6 |
c |
7 |
c |
8 |
b |
9 |
a |
10 |
a |
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
CANCER OF THE COLON AND RECTUM. PRECANCER (polyps, familial adenomatous polyposis, inflammatory diseases – ulcerative colitis, colonic Cron’s disease)
Составитель доц. Ю.И.Ломаченко
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
UNIT: COLOPROCTOLOGY
Theme: COLORECTAL CANCER
Basic information
Most colorectal cancers develop as a result of a stepwise progression from normal mucosa to adenomatous polyp into invasive cancer.
A polyp is an elevation above the mucosal surface. The majority of colorectal polyps are adenomas with malignant potential. Adenomatous colon polyps are premalignant, but only those with a villous component (50%-60% of all polyps) have a markedly increased tendency to become malignant.
Polyps must be removed endosco-pically for histological examination: when an infiltrating cancer is revealed, colon resection should be performed. Villous adenomas of the large bowel require total resection of the wall.
Most polyps are asymptomatic and find by chance on X-ray or on colonoscopy when patients are investigated for abdominal pain, intestinal malfunction, haemorrho-idal bleeding or some other causes.
The incidence of colorectal cancer is low in Africa and Asia and this
Раздел: КОЛОПРОКТОЛОГИЯ
Тема: колоректальный рак Цели изучения
Студент должен знать:
Большая часть колоректальных раков развивается путем образо-вания аденоматозных полипов из клеток слизистой оболочки с их трансформацией в инвазивный рак.
Полип представляет собой обра-зование, возвышающееся над поверхностью слизистой оболочки. Аденоматозные полипы являются предраком, ворсинчатые полипы из их числа (50-60% всех полипов) наиболее часто подвергаются озлокачествлению.
Полипы должны быть подверг-нуты гистологическому исследова-нию после эндоскопического уда-ления: в случае выявления рака пациент нуждается в резекции толстой кишки. Ворсинчатые аденомы требуют полнослойной резекции стенки кишки.
Полипы чаще клинически себя не проявляют и обнаруживаются случайно при рентгенологическом или эндоскопическом обследова-нии больных с болями в животе, дисфункцией толстой кишки, геморроидальным кровотечением или по другим причинам.
Болезнь является редкой в Африке и Азии, и эта особенность, вероят-
feature is thought to be largely environmental rather than racial. In the developed countries the inci-dence is rather high. In countries at low or intermediate risk, colorectal cancer is increasing.
There is a certain correlation between the consumption of meat and animal fats and colorectal cancer development.
In the colon certain bacteria convert bile acids into potential carcinogens.
The risk of colorectal cancer may be closely related to a positive family history. There is a 1.7 times increased lifetime risk of colorectal cancer if one first-degree relative is affected, but rises progressively with the number of affected family members. Patients with family polyposis almost invariably develop colorectal cancer at an more early age. Family polyposis requires total colectomy. The risk of colorectal cancer in patients with symptomatic ulcerative colitis may be 20%-25% in long-term cases (over 10 years).
About 90% of colorectal cancers occur in individuals who do not have a strong family history.
Any intestinal malfunction or rectal bleeding must be investigated, particularly in elderly people.
но, определяется окружающей средой, а не расовыми факторами. В развитых странах - высокие показатели заболеваемости. Часто-та колоректального рака увеличи-вается в странах с низким и средним уровнями заболеваемости.
Имеется зависимость заболевания колоректальным раком от употреб-ления мяса и животного жира.
В толстой кишке некоторые бакте-рии преобразовывают желчные кислоты в канцерогены.
Риск заболевания колоректальным раком может быть связан с наслед-ственной предрасположенностью. Вероятность развития рака увели-чивается в 1,7 раза, если болел один из близких родственников, и прогрессивно повышается с увели-чением больных раком в семье. У пациентов с семейным полипо-зом почти всегда развивается рак толстой кишки в более раннем возрасте. Семейный полипоз требует выполнения операции в объеме тотальной колэктомии. Риск заболевания колоректальным раком у больных с неспецифичес-ким язвенным колитом составляет 20-25% при анамнезе заболевания более 10 лет.
Приблизительно в 90% случаев ко-лоректального рака нет указаний на это заболевание у близких родственников больного.
Любое нарушения функции толс-той кишки или выделение крови из прямой кишки - показание к обсле-дованию, особенно у пожилых.
Faecal occult blood tests must use for mass screening for colorectal cancer.
Rectal cancer can be palpated by the digital rectal examination.
Colonoscopy is used to confirm tumor lesions and to obtain specimens for histological examination. Fifty percent of colo-rectal cancers are located within the reach of the proctosigmoidoscope (rectoromanoscope – RRS).
Abdominal and rectal ultrasound is performed prior to surgery to evaluate of the primary tumor size, its local and secondary (metastatic) spread.
Computed tomography (CT) and magnetic resonance imaging (MRI) are useful to evaluate hepatic metastases.
The primary tumor can be removed surgically in over 90% of cases. As a rule surgery is a method of choice and provides cure in a large percentage of cases. The segment of bowel with tumor is resected together with the lymph nodes draining it.
Preoperative radiation therapy is performed in large rectal cancers. Radiation therapy can decrease local recurrence and prolong survival period. Postoperative chemotherapy
Тесты на скрытую кровь в кале необходимо применять в скри-нинге колоректального рака.
Рак прямой кишки можно выявить при пальцевом исследо-вании прямой кишки.
Колоноскопия используется для подтверждения опухолевого по-ражения и взятия материала на гистологическое исследование. Метод проктосигмоскопии (рек-тороманоскопии – RRS) позво-ляет выявить 50% колоректаль-ных раков.
УЗИ брюшной полости и УЗИ ректальным датчиком произво-дятся до операции для оценки размера первичной опухоли, ее местного распространения и метастазирования.
Компьтерная томография и ЯМР полезны для подтверждения или исключения метастазов в печени.
Первичная опухоль может быть удалена хирургическим путем более чем в 90% случаев. Как правило, операция – первичный метод лечения в большинстве случаев колоректального рака. Пораженный отдел кишечника удаляется в едином блоке с регионарными лимфатическими узлами.
Показанием к предоперационной лучевой терапии являются боль-шие размеры опухоли прямой кишки. Лучевая терапия может предупредить развитие местного
is a consideration in patients with invasive tumors and those with metastases in lymph nodes.
Squamous cancers (syn. – cloaco-genic, epidermoid tumors) of the anus are treated successfully with radiotherapy (usually combined with chemotherapy).
18.Although the causes and patho-genesis of the tumors are similar throughout the large bowel, significant differences in the use of diagnostic and therapeutic methods differentiate colon and rectal tumors.
Practical skills:
history-taking procedure;
examination of the abdomen (inspection, palpation, percussion, auscultation);
interpretation of the history and results of examination using obtained knowledge of anatomy, physiology and pathology;
making diagnosis on the basis of laboratory tests and other investi-gations;
digital examination of the rectum;
to choose proper method of treatment and necessary variety of an operation.
рецидива опухоли и продлить жизнь пациента. Проведение послеоперационной химиотера-пии рассматривается у пациентов с агрессивными опухолями и метастазами в лимфоузлах.
17.Анальный плоскоклеточный рак хорошо лечится методом лучевой терапии (обычно в комбинации с химиотерапией).
18.Хотя причины и патогенез рако-вых опухолей толстой кишки являются сходными, важные раз-личия в применении диагности-ческих и лечебных методов требуют разграничения опухолей ободочной и прямой кишок.
Студент должен овладеть:
процессом опроса пациента о его жалобах и развитии заболевания.
обследованием живота (осмотр, пальпация, перкуссия, аускульта-ция).
интерпретацией данных анамнеза и обследования, основываясь на знаниях анатомии, физиологии и патологии.
диагностической гипотезой, кото-рая будет подтверждаться соот-ветствующими лабораторными и другими исследованиями.
пальцевым обследованием пря-мой кишки
знаниями, которые позволят избрать метод лечения и необхо-димый объем операции.
QUESTIONS TO ASSESS BASIC LEVEL OF KNOWLEDGE:
Anatomy of the large bowel (large intestine).
Blood supply to the large bowel.
Function (physiology) of the large bowel.
Macroscopical and microscopical forms of colorectal cancer.
BRIEF INFORMATION TO ANSWER THE QUESTIONS :
1. The large bowel extends from the ileocecal valve to the anus and is divided into five main segments. From proximal to distal these segments are: caecum with the vermiform (wormlike) appendix, ascending (right) colon, transverse colon, descending (left) colon, sigmoid colon and rectum. The hepatic flexure separates the ascending and the transverse colon and the splenic flexure separates transverse colon from the descending colon. Although the average total length of the large bowel is relatively constant (135 to 150 cm), the length of its anatomic divisions varies from person to person.
The large bowel contains the same circular muscular layer underneath the serosa as does the small intestine, but its outer longitudinal muscle layer is quite distinct. This outer longitudinal muscular coat consists of three separate longitudinal strips – the taeniae coli – which give the colon its characteristic appearance. At the level of the rectosigmoid junction, the taeniae generally coalesce and provide a complete longitudinal muscular coat for
ВОПРОСЫ ПО ИСХОДНОМУ УРОВНЮ ЗНАНИЙ:
Анатомия толстой кишки.
Кровоснабжение толстой кишки.
Функции толстой кишки.
Макро- и микроскопические фор-мы колоректального рака.
КРАТКИЕ ОТВЕТЫ НА ВОПРОСЫ ПО ИСХОДНОМУ УРОВНЮ ЗНАНИЙ:
1. Толстая кишка простирается от илеоцекального клапана до заднего прохода и подразделяется на пять основных отделов: слепая кишка с червеобразным отростком, восходя-щая ободочная, поперечно-ободочная нисходящая ободочная, сигмовидная кишка и прямая кишки. Печеночный изгиб отделяет восходящую и поперечно-ободочную кишки, селезе-ночный изгиб – поперечно-ободоч-ную и нисходящую ободочную киш-ки. Хотя средняя длина толстой кишки относительно постоянна (135–150 cm), длина его анатомических отделов может варьировать.
Толстая кишка содержит такой же циркулярный мышечный слой под серозной оболочкой, как тонкая кишка, но его внешний продольный мышечный слой весьма отличается. Он сконцентрирован в три отдельные продольные "полосы" – taeniae coli –что придает толстой кишке характер-ный вид. На уровне ректосигмоид-ного перехода, taeniae вообще соеди-няются и обеспечивают полный продольный мышечный слой для
the rectum. The state of contraction coli is what determines the typical configu-ration of the large bowel with successive sacculations, or protrusions, namely, haustra. On radiographs their appearance is quite characteristic. It allows a distinction of a normal large bowel from an abnormal large or small bowel. The third characteristic feature of the large bowel is the appendices epiploicae, which are extensions of peritoneal fat that hang off the antimesenteric side of the large bowel. The other characteristic features to the large bowel are the differences in diameter of the right and left colon, much higher location of the splenic flexure compared with the hepatic flexure, and the extraperitoneal nature of the pelvic rectum.
The rectum has an ill-defined ana-tomical beginning, the rectosigmoid junction lies opposite the sacral pro-montory. From the site the rectum follows the curve of the sacrum to end at the anorectal junction. At this point, the puborectalis muscle encircles the pos-terior and lateral area of the anorec-tal junction, creating the anorectal angle (normally 120°).
The rectum has three lateral curva-tures: the upper and lower are convex to the right, and the middle convex to the left (Houston's semicircular folds). That part of the rectum that lies below the middle valve has a much wider diame-ter and is known as the ampulla of the rectum. The adult rectum is approxima-tely 18-20 cm in length. The rectum is separated by Denonvilliers' fascia - from the prostate, and Waldeyer's fascia from the coccyx and last two sacral vertebrae. These fascial layers are surgi-
прямой кишки. Их сокращение опре-деляет типичную конфигурацию колон с последовательным мешко-видными расширениями (гаустрами). Их вид на рентгенограммах весьма характерен и позволяет различать нормальную толстую кишку от кишки с патологическими изменени-ями и тонкой кишки. Третье большое уникальное отличие заключается в наличии epiploicae (жировые привес-ки), которые состоят из жировой ткани и свисают с противобрыжееч-ной стороны толстой кишки. Другими характерными особеннос-тями толстой кишки являются различие в диаметре правой и левой половин толстой кишки, более высо-кое расположение селезеночного изгиба по сравнению с печеночным, экстраперитонеальное расположение тазового отдела прямой кишки.
Прямая кишка имеет условное анатомическое начало, ректосигмоид ный переход находится напротив промонториума. Отсюда прямая кишка повторяет искривления крест-ца, заканчиваться аноректальным пе-реходом. В этом месте, m.puborecta-lis, окружая сзади и сбоку область аноректального перехода, создает аноректальный угол (обычно 120°).
Прямая кишка имеет три боковых искривления: верхнее и более низ-кое – направо, среднее – налево (полукруглые складки Гаустона). Та часть прямой кишки, которая нахо-дится ниже средней складки, имеет наиболее широкий диаметр и назы-вается ампулой. Длина прямой киш-ки – приблизительно 18-20 см. Она отделена фасцией Денонвиллье от простаты и фасцией Валдейера – от
cally important as they act as a barrier to malignant penetration.
2. The cecum, ascending colon, hepatic flexure and proximal portion of the transverse colon receive arterial blood from the superior mesenteric artery.
The inferior mesenteric artery supplies blood to the distal transverse colon, splenic flexure, descending colon, and sigmoid via the left colic artery and branches of the sigmoid and superior rectal vessels. As the main vessels course through the mesentery toward the bowel wall, they bifurcate and form arcades at 1 to 2 cm from the mesenteric border. The arcades form a continuous chain of communicating vessels (the marginal artery of Drummond). Anastomosis between the superior and inferior mesenteric vessels is known as the anastomosis of Riolan (the arc of Riolan). The superior rectal artery is the direct continuation of the inferior mesenteric artery and is the main arterial supply of the rectum. A rich network of vessels that originate in both the middle and the inferior rectal arteries also supplies the rectum. The middle rectal artery arises on each side from the internal iliac artery and passes to the rectum in the lateral ligaments. The interior rectal artery arises on each side from the internal pudendal artery.
3. The main function of the colon is the absorption of water and electrolytes.
Approximately 2 L of fluid passes
копчика и последних двух крестцо-вых позвонков. Эти фасциальные слои имеют хирургическое значение, поскольку они препятствуют рас-пространению опухоли.
2. Слепая, восходящая ободочная кишка, область печеночного изгиба, и проксимальный отдел поперечно-ободочной кишки получают артери-альную кровь из верхней брыжееч-ной артерии.
Нижняя брыжеечная артерия кро-воснабжает дистальный отдел попе-речно-ободочной кишки, область селезеночного изгиба, нисходящую ободочную и сигмовидную кишки посредством левой толстокишечной, сигмовидных и верхней прямокишеч-ной артерий. В брыжейке магист-ральные сосуды раздваиваются и формируют аркады, которые образу-ют цепь сообщающихся сосудов (ар-терия Drummond). Анастомоз между верхней и нижней брыжеечными артериями известен как анастомоз Riolan (дуга Риолана). Верхняя пря-мокишечная артерия – прямое про-должение нижней брыжеечной арте-рии и главный источник артери-ального кровоснабжения прямой кишки. Богатой сетью сосудов, обра-зованных средней и нижней прямо-кишечными артериями, также обес-печивается кровоснабжение прямой кишки. Средние прямокишечные ар-терии отходят от внутренних под-вздошных артерий и проходят к киш-ке в боковых связках, нижние прямо-кишечные – от внутренних половых артерий.
3. Главная функция ободочной кишки – всасывание воды и электро-литов. Приблизительно 2 л жидкости
through the ileocaecal valve dayly. The absorption of fluid and electrolytes takes place mainly in the right side of the colon. And only about 150 mL of fluid is passed in the faeces.
The function of the rectum and anus in defaecation is complex. The rectum is usually empty. The entry of faeces from the colon produces relaxation of the internal sphincter and the puborectal muscle. This decreases the acute angle between the rectum and the anal canal. When the rectum contains approxima-tely 100 mL of faeces the urge to defecate is experienced. The rectum is emptied by relaxation of the external anal sphincter (under voluntary control) and an increase in intraabdominal pressure.
4. Microscopically, large bowel tumors are usually adenocarcinomas. Tumors of the anal canal are mostly of the squamous type. Macroscopically, the tumour may be one of five forms: annular, polypoid (cauliflower), diffusely infiltrating (tubular), ulcerative and colloid (mucocele). Cauliflower type is the least malignant form. The annular variety tends to give rise to obstructive symptoms whereas other forms commonly demonstrate bleeding.
проходит каждый день через илеоце-кальный клапан. Всасывание жидкос-ти и электролитов происходит глав-ным образом в правой половине обо-дочной кишки, и только приблизи-тельно 150 мл выделяется с калом.
Функция прямой кишки и заднего прохода в дефекации является слож-ной. Прямая кишка обычно пуста; при поступлении кала из ободочной кишки происходит расслабление внутреннего сфинктера и пуборек-тальной мышцы. Это уменьшает ост-рый угол между основной осью пря-мой кишки и осью анального канала. Когда прямая кишка содержит при-близительно 100 мл кала, появляет-ся позыв на дефекацию. Прямая киш-ка освобождается при расслаблении наружного анального сфинктера (процесс управляем человеком) и увеличении внутрибрюшного дав-ления.
4. Микроскопически раки толстой кишки – обычно аденокарциномы, раки анального канала имеют глав-ным образом форму плоскоклеточ-ного рака. Макроскопически опухоль может иметь одну из пяти форм: стенозирующую, экзофитную (поли-повидную), инфильтративную, язвен-ную и слизистую (коллоидную). Экзофитный тип опухоли – наименее злокачественная форма. Стенозиру-ющие формы вызывают кишечную непроходимость, тогда как другие обычно проявляют себя кровотече-нием.
KEY QUESTIONS FOR HOMEWORK:
Diseases of the large bowel having malignant potential.
Clinical classifications of colon and rectal tumors.
Metastatic spread of colorectal cancer.
Clinical features of colorectal cancer.
Diagnostic procedures (investiga-tions).
Screening of colorectal cancer.
Surgical management. Types of surgical treatment.
Rehabilitation.
Follow-up.
BRIEF INFORMATION TO ANSWER THE QUESTIONS :
Diseases of the large bowel, which have malignant potential:
polyps of the large bowel;
nonspecific inflammatory bowel disease.
Polyps of the large bowel (classification of polyps – see Table 1)
Adenomatous polyps and family adenomatous polyposis have significant malignant potential. Family adenoma-tous polyposis inevitably leads to cancer development. The risk of malignancy in an adenoma depends on the size of tumor. Peutz-Jeghers polyps and Juvenile polyps have minimal malignant potential.
ВОПРОСЫ ДЛЯ САМОПОДГОТОВКИ
Предопухолевая патология толс-той кишки.
Клинические классификации коло-ректального рака.
Метастазирование колоректаль-ного рака.
Клинические проявления.
Диагностические мероприятия.
Скрининг коллоректального рака.
Варианты хирургического лечения.
Реабилитация.
Отдаленные результаты.
КРАТКИЕ ОТВЕТЫ НА КЛЮЧЕВЫЕ ВОПРОСЫ
1. Предопухолевая патология толс-той кишки.
полипы толстой кишки;
неспецифические воспалительные заболевания толстой кишки.
Полипы толстой кишки (классифика-ция полипов – см. табл. 1).
Аденоматозные полипы и семейный аденоматозный (диффузный) поли-поз отличаются наиболее вероятным риском малигнизации. Семейный аденоматозный (диффузный) поли-поз является облигатным предраком. Риск малигнизации в аденоме повышается с увеличением размера опухоли. Малигнизация полипов не характерна для полипоза Пейтц-Егерса (Джегерса) и ювенильного полипоза.
Table 1
Classification of large bowel polyps
Class (type) |
Varieties of solitary polyps |
Multiple polyposis syndrome |
Inflammatory |
Inflammatory |
Inflammatory |
Metaplastic (Miscellaneous) |
Metaplastic or hyperplastic Lymphoid |
Benign lymphoid |
Hamartomas |
Peutz-Jeghers polyp Juvenile polyp |
Peutz-Jeghers syndrome Juvenile Cronkhite-Canada syndrome |
Neoplastic |
Adenomas:
|
Family adenomatous |
Классификация полипов толстой кишки
Класс (тип) полипа |
Разновидности одиночных полипов |
Синдромы множественного полипоза |
Воспалительные полипы |
Воспалительные полипы |
Воспалительный полипоз |
Метапластические полипы |
Метапластические или гиперпластические полипы Лимфоидные полипы |
Доброкачественный лимфоидный полипоз |
Гамартомные полипы |
Полип Пейтц-Егерса Ювенильный полип |
Синдром Пейтц-Егерса Ювенильный полипоз Синдром Кронкайта-Кэнедэ |
Неопластические полипы (с вероят-ным риском ма-лигнизации) |
Аденомы (тубулярная, тубуло-ворсинчатая, ворсинчатая) |
Семейный аденоматозный полипоз |
Nonspecific inflammatory bowel diseases.
Two major forms of nonspecific inflammatory bowel diseases are recognized: Crohn's disease and ulcerative colitis. Crohn's disease affects any part of the GI tract. Ulcerative colitis affects only the large bowel. In 10% of clinical colitis cases Crohn's disease and ulcerative colitis cannot be differentiated. Some experts consider these conditions represent two types of the same disease.
Crohn's disease can involve one small area. There also may bee multiple spread with relatively normal areas between them (so called «skip lesions»). The whole colon can also be effected (total colitis).
Ulcerative colitis can affect the rectum alone (proctitis). It can extend proximally to involve the sigmoid and descending colon («left-sided colitis»), or may involve the whole colon («total colitis»).
The incidence of carcinoma is 3‑5% in both conditions. Carcinoma is unlikely to develop in Crohn's disease. Risk of carcinoma development does not depend on the duration of treatment. In ulcerative colitis the risk of colon carcinoma is higher in a patient with 10 year-old total colitis. Ulcerative colitis is the nonobligative precancer.
Неспецифические воспалительные заболевания толстой кишки.
Основными формами неспецифичес-ких воспалительных заболеваний толстой кишки признаны: болезнь Крона, которая может поражать любую часть желудочно-кишечного тракта, и неспецифический язвенный колит, который считается самостоя-тельным заболеванием толстой кишки. В 10% клинических наблю-дений невозможно различить язвен-ный колит от болезни Крона толстой кишки. Не исключается, что эти забо-левания представляют две разновид-ности одной и той же болезни.
В болезнь Крона может вовле-каться часть кишки или обширные области с наличием неизмененных отделов между пораженными участ-ками («скачущий характер пораже-ния»). Болезнь Крона может пора-жать всю толстую кишку.
В язвенный колит может быть вовлечена прямая кишка (проктит), патологический процесс может рас-пространяться проксимально с вовле-чением сигмовидной и нисходящей ободочной кишок («левосторонний колит») или поражать всю толстую кишку («тотальный» колит).
Вероятность развития рака увеличена при обоих патологических состояниях (3-5%). Развитие рака при болезни Крона маловероятно и не зависит от лечения. Риск рака у пациентов с язвенным колитом выше после 10 лет консервативного лече-ния по сравнению с частотой его выявления в общей популяции насе-ления. Неспецифический язвенный колит является факультативным предраком.
Different approaches to classification of colon and rectum tumors.
Table 2
TNM classification |
Stage |
Spread of colorectal cancer |
Duke’s staging (ESMO*) |
Russian approach to classification |
5 year survival rate (data of ESMO*) |
TISN0M0 |
0 |
Carcinoma in situ |
— |
— |
~ 100% |
T1N0M0 |
I |
Mucosa and submucosa |
А |
Iа |
> 90 % |
T2N0M0 |
I |
Muscularis propria |
B1 |
IIа, IIIа |
85% |
T3N0M0 |
II |
Subserosa / pericolic or perirectal tissues |
B2 |
IIIа
IVа |
70 - 80 % |
T4N0M0 |
II |
Tumor perforates the visceral peritoneum and/or directly invades other organs or structures |
В3 |
||
T2N1-2M0 |
III |
T2N1:1−3/N2: ≥ 4 lymph nodes |
C1 |
IIб
IIIб |
25 - 60 % |
T3N1-2M0 |
III |
T3N1:1−3/N2: ≥4 lymph nodes |
C2 |
||
T4N1-2M0 |
III |
T4N1:1−3/N2: ≥4 lymph nodes |
СЗ |
||
any T and N, M1 |
IV |
Distant metastasis |
D |
IVб |
5-30 % |
2. Клинические классификации для опухолей ободочной и прямой кишок.
КлассификацияTNM |
Стадия |
Распространение |
Классификация Dukes (ESMO*) |
Отечествен-ная класси-фикация |
5-летняя общая выживаемость (данные ESMO*) |
TISN0M0 |
0 |
Carcinoma in situ |
— |
— |
~ 100% |
T1N0M0 |
I |
Мукозный и субмукозный слои (слизистая и подслизистая) |
А |
Iа |
> 90 % |
T2N0M0 |
I |
Собственный мышечный слой |
B1 |
IIа, IIIа |
85% |
T3N0M0 |
II |
Субсерозный слой/ ткани вокруг кишки |
B2 |
IIIа
IVа |
70 - 80 % |
T4N0M0 |
II |
Перфорация или инвазия в другие органы |
В3 |
||
T2N1-2M0 |
III |
T2N1:1−3/N2: ≥ 4 лимфоузла |
C1 |
IIб
IIIб |
25 - 60 % |
T3N1-2M0 |
III |
T3N1:1−3/N2: ≥4 лимфоузла |
C2 |
||
T4N1-2M0 |
III |
T4N1:1−3/N2: ≥4 лимфоузла |
СЗ |
||
Любые T и N, M1 |
IV |
Отдаленные метастазы |
D |
IVб |
5-30 % |
* ESMO - Европейское общество медицинской онкологии (ЕвМО).
Classification of colon and rectum cancer spread (TNM-classification):
T – Primary Tumor
Tx – Primary tumor cannot be assessed.
T0 – No evidence of primary tumor.
Tis – Carcinoma in situ (tumor invades only mucosa or malignanc polyps).
T1 – Tumor invades submucosa.
T2 – Tumor invades muscular layer of the intestinal wall.
T3 – Tumor invades through muscular layer of the intestinal wall into subserosa or into nonperitoneali-zed pericolic or perirectal tissues.
T4 – Tumor perforates visceral peritoneum or directly invades other organs or structures.
Note: Direct invasion in T4 includes invasion into other segments of the colorectum through serosa, e.g. invasion of caecum carcinoma into the sigmoid colon.
N – Regional Lymph Nodes
Nx – Regional lymph nodes cannot be assessed.
N0 – No regional lymph node metastasis.
N1 – Metastasis in 1-3 pericolic or perirectal lymph nodes.
N2 – Metastasis in 4 or more pericolic or perirectal lymph nodes.
N3 – Metastasis in any lymph node localed along major blood vessels.
Классификация распространения рака толстой кишки по системе TNM:
Т – первичная опухоль
Тх – Недостаточно данных для оценки первичной опухоли.
Т0 – Первичная опухоль не опреде-ляется.
Тis – Инвазия только слизистой обо-лочки, до базальной мембраны (малигнизированный полип).
Т1 – Опухоль распространяется на подслизистой слой стенки кишки.
Т2 – Опухоль распространяется на мышечный слой стенки кишки.
Т3 – Опухоль распространяется на субсерозу и ткани, прилежащие к неперитонизированным участкам ободочной и прямой кишок.
Т4 – Опухоль прорастает висцераль-ную брюшину или непосредст-венно распространяется на сосед-ние органы и структуры.
Примечание: Прямая инвазия при Т4 включает распространение на другие сегменты толстой кишки путем прорастания серозы, например, инвазия опухоли сле-пой кишки в сигмовидную.
N – регионарные лимфоузлы
Nх – Недостаточно данных для оцен-ки регионарных лимфоузлов.
N0 – Нет метастатического пораже-ния регионарных лимфоузлов.
N1 – Метастазы в 1-3 околокишечных лимфатических узлах.
N2 – Метастазы в 4 и более околоки-шечных лимфатических узлах.
N3 – Метастазы в лимфатических уз-лах, расположенных вдоль любо-го из магистральных сосудов.
M – Distant metastasis
Mx – Distant metastasis cannot be assessed.
M0 – No distant metastasis.
M1 – Distant metastasis.
Duke’s staging
A – The growth is within the intestinal wall. Favourable prognosis.
B – The growth is extended to the extracolic or extrarectal tissues, but no metastasis to the regional lymph nodes. Relatively favourable prognosis.
C – There are secondary deposits in the regional lymph nodes. These are subdivided into C1, in which the local pericolic or pararectal lymph nodes alone are involved, and C2, in which the nodes accompanying the supplying blood vessels are implicated up to the point of division. Cases of hematogenous metastases or metastases in regional lymph nodes are not taken into account. Poor prognosis.
Stage D (it was not described by Duke) signifies the residual disease following surgery or the presence of widespread metastases, mainly hepatic.
Other staging systems have been developed (e.g. Astler-Coller, ESMO) to improve prognostic accuracy.
The TNM classification is now recognised internationally as the optimal classification of staging.
M – Отдаленные метастазы
Мх – Недостаточно данных для опре-деления отдаленных метастазов
М0 – нет отдалённых метастазов;
M1 – имеются отдалённые метастазы.
Классификация Dukes
A – Опухолевый рост ограничен стенкой толстой кишки. Прогноз считается благоприятным.
B – Опухоль распространяется за пределы кишки при отсутствии метастазов в региональных лимфо-узлах. Прогноз считается относи-тельно благоприятным.
C – Имеются метастазы в региональ-ных лимфоузлах (C1 – единичные метастазы в региональных лимфо-узлах, C2 – метастазы по ходу магистральных сосудов, крово-снабжающих пораженный отдел кишечника, от уровня их отхож-дения). Исключаются случаи с гематогенными метастазами и метастазами в отдаленных лимфа-тических узлах. Прогноз считается неблагоприятным.
Часто выделяется стадия D (не счита-ется предложением Dukes). Эта ста-дия обозначает наличие нерадикаль-но удаленной опухоли или отдален-ных метастазов, обычно – в печени.
Для более точного прoгнозиро-вания предложены модификации клинических классификаций (напри-мер: Astler-Coller, ЕвМО).
TNM-классификация является международной и общепризнанной.
Early colorectal cancer.
Early colorectal cancer is carcinoma that invades as far as the submucosa. Patients having this type of cancer demonstrate a five-year survival rate about 90%.
3. Metastatic spread of colorectal cancer.
Colorectal cancer spreads directly into the adjacent organs and structures. Metastatic spread occurs by both the lymph and blood streams; most colon cancers metastasize to the retroperitoneal periaortic nodes following the mesenteric vessels. Anal carcinomas spread more commonly to the groin nodes, rather than retroperitoneally. Distant spread by blood stream affects, in particular, the liver, as well as the lungs and bone. Rectal cancers (below the peritoneal reflection) tend to spread laterally into the pelvic tissues and then directly to the lungs. Anal carcinoma may extend directly into the sphincters, perianal tissues, vagina, or prostate, and it tends to metastasize to lymph nodes behind the rectum and in the groins.
4. Clinical manifestations.
Alteration in bowel habit, with or without abdominal pain, is a common symptom of left-sided colonic lesions. Rectum and sigmoid carcinomas usually discharge blood mixed in with the stool. Sigmoid lesions more commonly cause obstructive symptoms.
Ранний колоректальный рак.
К раннему колоректальному раку относят опухоли, распространяю-щиеся не глубже подслизистого слоя. Пятилетняя выживаемость пациентов с эти видом рака составляет почти 90%.
3. Метастазирование колоректаль-ного рака.
Колоректальный рак распространяет-ся непосредственно в окружающие органы и структуры. Метастазирова-ние происходит гематогенным и лим-фогенным путями; раковые опухоли ободочной кишки главным образом метастазируют в забрюшинные пара-аортальные лимфоузлы по ходу мезентериальных сосудов. Анальные раки метастазируют как правило в паховые, с меньшей вероятностью – в забрюшинные лимфоузлы. Отда-ленное метастазирование происходит гематогенно наиболее часто в печень, а также в легкие и кости. Раки пря-мой кишки склонны распространять-ся на окружающие ткани и органы малого таза, а затем гематогенно метастазируют прямо в легкие. Анальный рак может распростра-няться на близрасположенный сфинктер, перианальные ткани, вла-галище или простату, что сопровож-дается метастазированием в позади-прямокишечные и паховые лимфо-узлы.
4. Клинические проявления.
Изменение функции толстой кишки, с или без абдоминальной боли, является распространенным симпто-мом поражения ее левых отделов. Раки прямой и сигмовидной кишок обычно проявляются кровотечением, кровь смешивается с калом. Рак сиг-
Rectal cancers cause obvious bleeding with defecation and a feeling of incomplete evacuation when the tumor becomes larger. Symptoms of the anal carcinoma (bleeding, pain and a mass) are often mistakenly attributed to hemorrhoids. Carcinoma of the caecum may become large and be asymptomatic. It can present simply as an iron-deficiency anemia or anemia with unknown etiology. Elderly people are often admitted to the hospital with intestinal obstruction.
Diagnostic procedures (investiga-tions).
Diagnostic procedures include:
in order to exclude or confirm local spread (for evaluation of tumor size and local spread):
digital examination;
proctosigmoidoscopy (colonoscopy);
rectal ultrasound;
CT- or MRI-scanning;
barium enemas (Double-contrast barium enema);
urography;
cystoscopy;
biopsy of the tumor provides proof of cancer development;
additional investigations to detect metastases (for evaluation of meta-stases size and secondary spread):
chest and bone X-rays;
liver scanning (abdominal ultrasound and CT or MRI);
other diagnostic procedures:
laboratory studies (blood count and routine biochemistry);
мовидной кишки часто сопровожда-ется развитием признаков кишечной непроходимости. Раки прямой кишки кровоточат при дефекации и могут вызывать чувство неполного опорож-нения прямой кишки, когда опухоль становится большой. Симптомы анального рака (кровотечение, боль, узловое образование) часто ошибоч-но объясняются геморроем. Рак сле-пой кишки даже при больших размерах опухоли могут протекать бессимптомно. При этом может выявляться железодефицитная или необъяснимая анемия. Пациенты пожилого возраста часто поступают с симптомами кишечной непроходи-мости.
Диагностические исследования.
Чтобы исключать или подтвердить местное распространение (для оценки размера опухоли и местного распространения): пальцевое иссле-дование прямой кишки; проктосиг-москопия (колоноскопия); эндорек-тальное ультразвуковое исследова-ние; компьютерное и ЯМР-сканиро-вание; ирригография (в том числе – по методике двойного контрастиро-вания); урография; цистоскопия.
Биопсия доказывает наличие рака.
Дополнительние исследования, с целью обнаружить метастазы (для оценки размера метастазов и распространенности метастазирова-ния): рентгенологическое обследо-вание грудной клетки и костей; сканирование печени (УЗИ брюшной полости, КТ или ЯМРТ);
Другие диагностические проце-дуры:
лабораторные исследования (анализ крови и обычная биохимия);
carcinoembryonic antigen (CEA) is often elevated in colorectal cancer. It is use for early diagnosis. It can also be used to detect recurrence.
fecal occult blood tests for mass screening. But they are of no value in hospital practice.
6. Screening of the colorectal cancer.
Fecal occult blood test is used for screening and is being applied widely. Patients with positive tests are studied further with sigmoidoscopy, barium enemas, and colonoscopy. Annual occult blood stool testing is aimed at both detection of earlier stage cancers and improved long-term survival. Screening sigmoidoscopies are recommended every 4-5 years. Any screening strategy utilizing sigmoido-scopy also requires a colonoscopy to follow any positive sigmoidoscopy to look for synchronous lesions in the more proximal colon. In the lack of screening programs, the existence of colon and rectal cancer must be suspected because of the history. Changes in bowel habits, blood in stools, tenesmus, mucoid discharge, anemia with unknown etiology, and weight loss are suggestive symptoms.
определение уровня карцино-эмбрионального антигена (CEA) – часто повышается при колоректаль-ном раке. Не доказано значение этого исследования для установления ран-него диагноза рака, но имеет значе-ние в выявлении рецидивов заболева-ния прежде, чем появятся клиничес-кие симптомы. В этом случае повтор-ные операции имеют больше шансов на успех.
Анализ кала на скрытую кровь – используется для скрининга рака, но не имеют значения для выбора методов лечения.
6.Скрининг колоректального рака.
Анализ кала на скрытую кровь разра-ботан и широко используется для скрининга колоректального рака. Пациенты с положительным тестом подлежат дальнейшему обследова-нию методами сигмоскопии, колоно-скопии или ирригографии. Ежегод-ное исследования кала на скрытую кровь позволяет выявить опухоли на более ранних стадиях развития, что улучшает результаты лечения. Сиг-москопию с целью скрининга реко-мендуется выполнять каждые 4-5 лет. Любой скрининг, предусматриваю-щий сигмоскопию, при выявлении опухоли требует последующего выполнения колоноскопии, чтобы исключить синхронные опухоли в вышележащих отделах ободочной кишки. В отсутствии программ скри-нинга, рак толстой кишки должен быть заподозрен по анамнестическим данным. Нарушения функций киш-ки, кровь в кале, тенезмы, слизистые выделения, необъясненная анемия и потеря веса – симптомы, позволяю-щие заподозрить рак.
7.Types of surgical treatment.
Radical operations are designed to remove the primary tumor and its draining local lymph nodes. The extent of resection is determined by the location of the tumor, its blood supply and draining lymphatic vessels, and the lack of direct extension into adjacent organs. Manipulation of the tumor should be careful because tumor cells easily dissiminate and reimplant within the peritoneal cavity. There is some evidence that early division of major blood vessels supplying the involved colon can slightly improve the number of successful operations.
Cancer of the caecum or ascending colon. Cancer of the caecum or ascending colon is treated when resectable by right hemicolectomy. Anastomosis is performed between the terminal ileum and the transverse colon.
Cancer of the hepatic flexure.
When the hepatic flexure is involved, the resection must be extended correspondingly (an extended right hemicolectomy). Anastomosis is performed between the terminal ileum and the proximal left colon.
Cancer of the transverse colon.
When there is no obstruction, excision of the transverse colon together with the transverse mesocolon and the greater omentum, followed by end-to-end anastomosis, can be used. An alternative is an extended right hemicolectomy.
7. Варианты хирургического лече-ния. Операции предусматривают удаление первичной опухоли с зоной регионарных лимфатических узлов. Протяженность резекции кишки зависит от местоположения опухоли, особенностей кровоснабжения и лимфооттока, наличия распростране-ния опухоли на соседние органы. При возможности необходимо избе-гать лишних манипуляций с опухо-лью, поскольку опухолевые клетки, как известно, легко диссеминируют и имплантируются в пределах брюш-ной полости. Доказано, что изначаль-ная обработка сосудов, участвующих в кровоснабжении отдела кишки, пораженного опухолью, улучшает результаты лечения.
Рак слепой и восходящей ободоч-ной кишки. Радикальной операцией является правосторонняя гемикол-эктомия. Анастомоз после резекции накладывается между подвздошной и поперечноободочной кишками.
Рак области печеночного изгиба ободочной кишки. При локализации опухоли в области печеночного изгиба границы резекции ободочной кишки расширяются (расширенная правосторонняя гемиколэктомия). Анастомоз после резекции наклады-вается между подвздошной кишкой и проксимальными отделами левой половины ободочной кишки.
Рак поперечноободочной кишки. При отсутствии непроходимости выполняется резекция поперечнообо-дочной кишки вместе с ее брыжей-кой и большим сальником. Альтерна-тивной операцией является расши-ренная правосторонняя гемикол-эктомия.
Cancer of the splenic flexure or descending colon.
Left hemicolectomy is the procedure of choice for descending colon tumors. Anastomosis is performed between the transverse and sigmoid colon. When the splenic flexure is involved, the resection must be extended correspondingly (an extended left hemicolectomy). Anastomosis is performed between the distal right and sigmoid colon. Sometimes removal of the colon up to the ileum (the subtotal colectomy), with an ileorectal anastomosis, is preferable.
Cancer of the sigmoid colon.
Sigmoidectomy is oncologically adequate for tumours of the sigmoid colon.
Subtotal colectomy.
Subtotal colectomy is indicated for multiple primary tumors. Subtotal colectomy is sometimes termed as total colectomy. Subtotal colectomy involves removal of the colon from the cecum to the peritoneal reflection, with an ileorectal anastomosis. Due to loss of the absorptive capacity of the colon, this procedure results in a high postoperative stool frequency.
Cancer of the rectum.
The choice of surgery is determined by the distance of the tumor from the
Рак области селезеночного изгиба и нисходящего отдела ободочной кишки. Левосторонняя гемиколэкто-мия является операцией выбора при раке нисходящего отдела ободочной кишки. Анастомоз после резекции кишки накладывается между попе-речноободочной и сигмовидной киш-ками. При локализации опухоли в области селезеночного изгиба грани-цы резекции ободочной кишки рас-ширяются (расширенная левосторон-няя гемиколэктомия). Анастомоз после резекции накладывается между дистальными отделами правой поло-вины ободочной и сигмовидной киш-ками. Иногда предпочтительным является удаление ободочной кишки до уровня терминального отдела подвздошной кишки с наложением илеоректального анастомоза (субто-тальная колэктомия).
Рак сигмовидной кишки. Резекция сигмовидной кишки при ее опухоле-вом поражении является адекватной операцией с точки зрения онкологи-ческих принципов.
Субтотальная колэктомия. Суб-тотальная колэктомия показана при наличии множественных первичных опухолей. Субтотальная колэктомия (иногда упоминается как тотальная колэктомия) предусматривает удале-ние всей ободочной кишки с после-дующим наложением илеоректоана-стомоза. Из-за потери абсорбционной способности в связи с удалением ободочной кишки, после этой операции отмечается учащение количества актов дефекации.
Рак прямой кишки. Выбор спосо-ба операции во многом определяется
dentate line. A important general principle is that the ends of the colon and rectum to be anastomosed after resection should have a good blood supply and be seen to bleed arterial blood. Ischemia is the main cause of anastomotic failure and subsequent leakage.
Basic types of operations:
1) anterior resection (lesions located 5 to 6 cm above the dentate line). Stapling instruments, first developed in Russia, are now widely used to perform anastomoses.
High anterior resection of the rectum is a colorectal resection with anastomosis of the sigmoid colon to intraperitoneal rectum.
Low anterior resection of the rectum is a colorectal resection with anastomosis of the sigmoid colon to extraperitoneal rectum.
Low anterior resection of the rectum with coloanal anastomosis is a colorectal resection with anastomosis of the colon to the anal canal circumferen-tially.
2) abdominoperineal resection (lesi-ons located 5 to 6 cm to the dentate line).
Complete removal of the rectum and anus, by concomitant dissection through the abdomen and perineum, with permanent closure of the perineal rafe and creation of an end colostomy is called the Quenu’s and Miles’ opera-tion. The abdominal portion of the procedure reaches the level of the levator ani muscles, with removal of the
расстоянием края опухоли от зуб-чатой линии. Важным общим прин-ципом наложения межкишечного анастомоза по типу «конец в конец» является хорошее кровоснабжение, как замечено с краев разреза при этом выделяется алая (артериальная) кровь. Ишемия – основная причина несостоятельности швов анастомоза.
Основные типы операций:
передняя резекция (нижний край опухоли располагается выше 5-6 см от зубчатой линии). Для наложения межкишечных анастомозов сейчас широко применяются сшивающие аппараты, первоначально разрабо-танные в России.
Высокая передняя резекция прямой кишки – резекция с анастомозом сигмовидной кишки и интраперито-неальной части прямой кишки.
Низкая передняя резекция прямой кишки – резекция с анастомозом сигмовидной кишки и экстраперито-неальной части прямой кишки.
Низкая передняя резекция прямой кишки с колоанальным анастомо- зом – резекция с анастомозом ободочной и прямой кишок по окружности в анальном канале.
брюшно-промежностная экстирпа-ция (нижний край опухоли распола-гается на расстоянии 5-6 см от зубчатой линии).
Полное удаление прямой кишки и ануса из брюшного и промежност-ного доступа с закрытием промеж-ностной раны и наложением коло-стомы называется операцией Кеню-Майлса. Абдоминальный этап опера-ции предусматривает достижение уровня мышцы, поднимающей зад-ний проход, путем диссекции вдоль
entire mesorectum and dissection to and along the parietal endopelvic fascia. The perineal portion of the operation removes the anorectal junction and distal rectum, as well as the anal sphincter mechanism.
3) sphincter-sparing procedures.
Although the Quenu’s and Miles’ operation (abdominoperineal resection) is the gold standard for the treatment of distal rectal cancers. Patients with local disease may be adequately treated with sphincter-sparing procedures. To reach adequate continence after resection of the rectum, both sphincter muscles – the puborectalis and the levator ani – must be preserved, as well as the sympathetic and parasympathetic innervation of these muscles, which derives from the sacral plexus.
4) Hartmann's operation.
Hartmann's operation is an anterior resection of the rectum without anastomosis. The proximal bowel end is brought out as a left iliac fossa colostomy and the rectal stump is oversewn. The operation is usually performed as a palliative procedure or sometimes as a procedure for acute cases (acute malignant colonic obstruct-tion, peritonitis from perforation of rectal cancer or bleeding, a much more advanced tumor).
Now it is possible to perform a high anterior resection, hemicolectomy and other operations laparo-scopically.
пристеночной внутритазовой фасции. Промежностный этап операции пре-дусматривает удаление зоны анорек-тального перехода, дистальных отде-лов прямой кишки и мышц анального сфинктера.
сфинктер-сохраняющие операции.
Хотя операция Кеню-Майлса являет-ся золотым стандартом для лечения раковых опухолей дистального отдела прямой кишки, пациентов с местно нераспространенными раками можно лечить с применением сфинктер-сохраняющей операции. Чтобы сфинктер оставался функцио-нально состоятельным после резек-ции прямой кишки, должны быть сохранены обе мышцы сфинктерного аппарата – пуборектальная и подни-мающая задний проход, а также симпатическая и парасимпатическая иннервация этих мышц, исходящая из сакрального сплетения.
4) Операция Гартмана, в сущности, является передней резекцией прямой кишки, но без наложения межкишеч-ного анастомоза. Проксимальный отдел кишки выводится в левой подвздошной области с формирова-нием колостомы, а культя прямой кишки ушивается. Операция обычно выполняется как паллиативная или иногда – в неотложных случаях (острая опухолевая толстокишечная непроходимость, перитонит с перфо-рацией рака прямой кишки или кровотечение, местнораспространен-ная опухоль).
В настоящее время возможно вы-полнение высокой передней резек-ции прямой кишки, гемиколэкто-мии и других операций лапаро-скопическим методом.
Colostomy.
Colostomy is an artificial opening made in the large bowel to divert faeces to the exterior, where it can be collected in an external appliance. A wide range of disposable adhesive bags are available now. Depending on the purpose for which the diversion has been necessary, colostomy may be temporary or permanent.
When the obstructing tumors present in the left colon or rectum, a single stage operation is seldom performed. If a resection can be carried out, an end proximal colostomy should be done. Otherwise, a proximal defunctioning colostomy alone is done. The defunctioning colostomy can be carried out in the sigmoid colon or transverse colon. A proximal colostomy must be performed in these cases as a first stage, with resection of the tumor deferred until proper conditions can be secured. The site of the colon or rectum obstruction and the general condition of the patient determine whether a colostomy is indicated.
Solitary liver metastasis.
The presence of a solitary liver metastasis does not necessarily rule out the feasibility of a radical excision. Many instances have been reported where a presumed solitary liver metastasis has been resected either at the time of excision of the large bowel or subsequently with long-term survival being achieved.
Колостомия. Колостома – искус-ственно наложенный свищ на один из отделов толстой кишки. Выделяю-щийся кал может быть собран в кало-приемник. В настоящее время досту-пен широкий выбор одноразовых фиксирующихся калоприемников. В зависимости от цели, для которой было предпринято оперативное вме-шательство, колостома бывает вре-менной или постоянной.
Когда опухоль, обтурирующая просвет кишки, располагается в ле-вой половине ободочной или прямой кишках, операция редко выполнима в один этап. Если может быть выпол-нена резекция, то должна быть нало-жена концевая колостома на приво-дящий отдел кишки. В других слу-чаях проксимально должна быть наложена декомпрессивная колосто-ма. Она может быть сформирована на сигмовидной или поперечноободоч-ной кишках. В этих случаях колосто-ма на приводящий отдел кишки должна быть наложена как первый этап, резекция по поводу опухоли откладывается, пока не будет долж-ных условий для ее выполнения. Локализация кишечной непроходи-мости в толстой кишке и общее состояние пациента определяют, показана ли колостомия.
Солитарные метастазы в печени. Наличие солитарного метастаза в печени не исключает его радикального удаления. Имеется много сообщений об удалении солитарных метастазов в печени либо во время резекции толстой кишки или в последующем с достижением хороших отдаленных результатов лечения.
8.Rehabilitation.
A good rehabilitation program benefits the colostomy patients in returning to normal life. Special programs have been developed in which patients are instructed in the use of irrigation in order to limit discharge to a once-per-day occurrence. Patients must been trained to manage a variety of problems related to the colostomy (odor, leakage, equipment, sexual readjustment, etc.).
9. Follow-up.
The incidence of subsequent (metachronous) polyps and/or cancer is high, approaching a total of 15%-20% after 15-20 years. These should be diagnosed and treated early. Since patients who have had one colorectal cancer are at much higher risk than other patients, periodic colonoscopy is appropriate. If careful examination of the entire large bowel was not done either preoperatively or at the time of surgery, early follow-up (within 3-4 months) is important because of the high risk of synchronous polyps or carcinomas. Then colonoscopies should be perfopmed periodicaly (every 6-12 months during 5 years, then every 2-3 years). Follow-up for the possibility of recurrences is also very important because some recurrences have a significant chance of being cured:
1) anastomotic recurrences;
8. Реабилитация.
Хорошая программа реабилита-ции помогает возвратиться колосто-мированным пациентам к нормаль-ной жизни. Разработаны специаль-ные программы, в которых пациенты проинструктированы в использова-нии ирригации для того, чтобы ки-шечник опорожнялся один раз в день. Пациенты должны быть обу-чены решению различных проблем, связанных с колостомой (запах, исте-чение жидкого кала, специальные приспособления, вопросы сексуаль-ных отношений и т.д.).
9.Отдаленные результаты.
Выявление последующих (метахрон-ных) полипов и/или рака является частым, приближается к 15-20% после 15-20 лет. Они должны быть диагностированы и своевременно подвергнуты лечению. Поскольку больные, лечившиеся по поводу колоректального рака, имеют более высокий риск повторного заболева-ния, чем другие пациенты, им необ-ходимо периодически выполнять колоноскопию. Если тщательного обследования всей толстой кишки не проведено до или во время операции, важно продолжить обследование (в первые 3-4 месяца) из-за высокого риска синхронных полипов или рака. Затем колоноскопии должны выпол-няться периодически (каждые 6-12 месяцев в течение 5 лет, потом каждые 2-3 года). Продолжение наблюдения за больными также очень важно в связи с возможностью рецидивов рака, некоторые из которых могут быть подвергнуты лечению:
1) рецидивы в области анастомоза;
2) pelvic recurrences that are not fixed to the lateral pelvic walls;
3) apparently single metastases in the liver or (less often) in the lung after a fairly long disease-free interval (1-2 years or more)
2) рецидивы в полости малого таза, не фиксированные к его боковым стенкам;
3) явно одиночные метастазы в печени или (менее часто) в легком после довольно длительного безреци-дивного периода (1-2 года или больше).
TESTS
1. The superior rectal artery arises from the -
a) Superior mesenteric artery
b) Inferior mesenteric artery
c) Internal illiac artery
d) Internal pudendal artery
2. Middle rectal artery is branch of......... artery :
a) Internal iliac
b) Internal pudendal
c) External iliac
d) Femoral
3. Fascia of Denonvilliers -
a) Membranous layer of fascia of the thigh
b) Perirenal fascia
c) Fascia between the rectal ampulla and the prostate and the seminal vesicles
d) Posterior layer of perirenal fascia
4. Muscle which is primarily responsible for rectal continence -
a) Ext. sphincter
b) Int. sphincter
c) Puborectalis
d) Sacrococcygeous
5. Internal sphincter of rectum is formed by -
a) Levator ani
b) Puborectalis
c) Longitudinal muscle fibres condensation
d) Circular muscles fibres condensation
6. Ulcerative colitis almost always involves the ... -
a) Caecum
b) Sigmoid
c) Right colon
d) Rectum
7. Predisposing factors for colonic carcinomas - a) Familial polyposis
b) Gardener's syndrome
c) Juvenile polyp
d) Chronic ulcerative colitis
8. Tenesmus occurs in lesions of - a) ileum
b) Right side of colon
c) Descending colon
d) Sigmoid colon
9. Sulfonamide useful in treating ulcerative colitis is -
a) Sulfadiazine
b) Sulfasalazine
c) Sulfamethoxazole
d) Sulfadimidine
10. Highest risk for malignancy in colon is for -
a) Gardners syndrome
b) Ulcerative colitis
c) Crohn’s disease
d) Familial polyposis
11. Which is true of Ulcerative colitis -
a) Sting sign of kantor positive
b) Skin lesions are seen
c) Rectum is always invlolved
d) Fistulas are common
12. Which is not true of arthritis associated with inflammatory bowel disease -
a) Migratory arthritis
b) Knee joint most common
c) Deformities are common
d) Correlates to severity of colitis
13. Prophylactic polypectomy is done in -
a) Peutz Jegher’s syndrome
b) Gardner's syndrome
c) Familial polyposis
d) None of the above
14. The incidence of carcinoma of the caecum in relation to colonic adenocarcinoma is -
a) 2%
b) 4.5%
c) 20%
d) 44'%
e) 62%
15. The appearance of anastamotic leakage following a low colonic anastomosis most often mainfests -
a) 1-4 days
b) 5-10 days
c) 11-15 days
d) 16-20 days
e) None of the above
16. The most likely cause for suture leak after colon resection and anastomosis for cancer sigmoid is -
a) Subclinical malnutrition
b) Infection of anastomotic site
c) Mechanical disruption due to colonic pressure and contractility
d) Ischemia
17. The adenomatous polyps of large bowel are most often situated in -
a) Ascending colon
b) Transverse colon
c) Descending colon
d) Sigmoid colon
18. Which of the following is not a precancerous condition of colon -
a) Irritable bowel syndrome
b) Ulcerative colitis
c) Familial polyposis
d) All
19. Toxic megacolon is a complication of -
a) Ulcerative colitis
b) Crohn's
c) Aganglionic megacolon
d) Ischemic colitis
20. False regarding involvement in Crohn’s disease -
a) Anorectal area
b) Rectum
c) Small intestine with Rt. colon
d) Large intestine alone without involvement of small intestine
21. Most precancerous condition for carcinoma colon is -
a) Familial polyposis
b) hamartomatous polyps
c) Juvenile polyps
d) Hyperplastic polyps
22. Duke's stage C2 refers to carci-noma –
a) Bladder penetrating the extravesical fat
b) Bladder with metastasis to internal iliac lymph nodes
c) With histological features of 75% anaplastic cells
d) Rectum with metastasis to inferior mesentric lymph nodes
23. Carcinoma of the colon is associated with all of the following except -
a) Low residue diet
b) Vegetarian diet
c) Ulcerative colitis
d) Familial polyposis
24. Best investigation for carcinoma colon -
a) Barium enema
b) Colonic biopsy
c) Clinical examination
d) Colonoscopy
25. Regarding incidence of carcinoma colon in ulcerative colitis which is true -
a) Arise from pseudopolyps
b) Increased incidence if age of onset of ulcerative colitis early
c) Always associated with extraintestinal manifestation
d) Increased incidence with increase in age
26. The best investigation for colorectal carcinoma -
a) Exfoliative cytology
b) Air contrast barium enema
c) Ultrasound
d) Colonoscopy and biopsy
27. In ulcerative colitis, the inflammatory process is usually confined to -
a) Mucosa alone
b) Mucosa and submucosa
c) Mucosa, submucosa and muscularis
d) Mucosa submucosa, muscularis and serosa
28. The polyp with least malignant potential -
a) Hyperplastic polyp
b) Pseudo adenoma
c) Vilious adenoma
d) Tubular adenoma
29. On colonoscopy which of the following is highly malignant -
a) Single pedunculated polyp
b) Multiple flat polyps about hundreds
c) Multiple pedunculated polyps
d) Solitary flat polyp
30. Carcinoma of the right colon usually present with -
a) Perforation
b) Massive bleeding
c) Large bowel obstruction
d) Alteration of bowel habits
31. Management of carcinoma descending colon in a 75 year old male is -
a) Total colectomy
b) Left hemicolectomy
c) Defunctional colostomy
d) Harmann’s procedure
32. True about carcinoma colon is -
a) Left side present with anemia
b) Solitary liver metastasis is not a contraindication to surgery
c) Most common site is ascending colon
d) Right side are usually stenosing variety
33. Which of the following is true about carcinoma colon -
a) Lesion on the left side of the colon presents with features of anemia
b) Solitary metastasis in liver is not a contraindication for surgery
c) Mucinous carcinoma has a good prognosis
d) Duke's A stage should receive adjuvant chemotherapy
34. The following regarding colostomy are true except –
a) A colostomy is an artificial opening made in large bowel to divert the faces to the exterior
b) Temporary colostomy is established to defunction an anastomosis
c) Permanent colostomy is formed after the resection of rectum by the abdominoperineal technique
d) Double barreled colostomy is commonly done nowadays
e) Colostomy hernia is a common complication
35. Best investigation of acute mecha-nical intestinal obstruction is -
a) X-Ray abdomen
b) Barium enema
c) Proctosigmoidoscopy
d) Flatus tube
36. Acute mechanical large bowel obstruction should be operated early because -
a) Electrolyte imbalance due to third space loss
b) Septicemia from absorption of bowel contents
c) Early gangrene and perforation
d) Respiratory embarrassment to massive abdominal distension
37. Acute mechanical large bowel obstruction should be operated early because of the risk of -
a) Respiratory embarrassment due to abdominal distension
b) Electrolyte imbalance from vomiting
c) Septicemia from bowel contents
d) Closed-loop obstruction and caecal perforation
38. Treatment of choice of acute obstruction due to left sided colonic carcinoma in a 70 year old male is -
a) Left sided colectomy
b) Total colectomy
c) Hartman’s procedure
d) Defunctioning colostomy
39. Best way to diagnose lower intestinal obstruction -
a) Pain abdomen
b) Abdominal distension
c) Profuse vomiting
d) Multiple air gas shadows on X-ray
40. Prognosis for carcinoma rectum is best assessed by
a) Site of tumour
b) Histological grading
c) Size of tumours
d) Duration of the symptoms
41. Earliest symptoms of carcinoma rectum-
a) Pain
b) Alteration of bowel habits
c) Bleeding PR
d) Tenesmus
42. Villous polyp of rectum manifest -
a) Bleeding PR
b) Mucus diarrhoea with hypokalemia
c) Prolapse rectum
d) Obstruction
43. Anterior resection is contra indicated in the following-
a) Age more than 60 years)
b) Undifferentiated carcinoma
c) Melanin in liver
d) Cancer is less than 5 cm from anorectal margin
44. In Duke's classification of cancer rectum, B2 denotes-
a) Growth extends to perirectal fat
b) Regional nodes involved
c) Limited to thickness of bowel wall
d) Hepatic metastasis
45. Distal clearance in surgery for carcinoma rectum is-
a) 2 cm
b) 5 cm
c) 10 cm
d) 8cm
46. Best procedure in mid rectal carcinoma is -
a) Abdominoperineal resection
b) Anterior resection
c) Perineal loop
d) Transverse colostomy
47. The best surgical management for villous adenoma of the rectum is –
a) Local resection of lesion
b) Repeated sigmoidoscopy
c) Abdominoperineal resection
d) Electrolyte infusion and chemotherapy
48. Treatment of carcinoma rectum 5 cm from anal verge without nodal metastasis is -
a) Abdominoperineal resection
b) Radiotherapy
c) Endoscopic resection
d)Chemotherapy
49. Rectal polyps usually present with -
a) Obstruction
b) Perforation
c) Bleeding
d) Malignant change
50. In carcinoma of anus distal margin of clearance of anal canal of at least .............
a) 2 cm
b) 5 cm
c) 4 cm
d) 7 cm
51. Cancer of the anus is commonly -
a) Adenocarcinoma
b) Squamous carcinoma
c) Melanoma
d) Sarcoma
52. Below the pectineal line the lymphatic spread is to .....nodes-
a) Superficial inguinal
b) Internal iliac
c) External iliac
d) Para aortic
53. Commonest cause of bleeding PR in a male between 20-40 yrs is -
a) Carcinoma rectum
b) Internal haemorrhoids
c) Fissure in anus
d) Rectal polyp
54. Commonest cause of bleeding PR in India -
a) Cancer rectum
b) Internal haemorrhoids
c) Rectal polyps
d) Fissure-in-ano
55. The most common cause of painless bleeding PR in a man is -
a) Fissure-in-ano
b) Diverticulosis
c) Piles
d) None
56. Ideal treatment for squamous cell carcinoma of Anal canal is –
a) Pelvic exentration
b) Chemotherapy and radiotherapy
c) Chemotherapy alone
d) Abdominoperineal resection
57. In anal carcinoma the treatment of choice is -
a) Radio+ Chemo
b) APR + Radiation c) Only radio
d) Radio+Chemo followed by APR
58. Commonest site for carcinoid tumour is -
a) ileum
b) Appendix
c) Rectum
d) Colon
59. Raised level of Carcino-embryonic antigen is seen in –
a) Carcinoma colon
b) Carcinoma breast c) Carcinoma lung d) Carcinoma ovary
60. The commonest cancer of adult man in India is -
a) Carcinoma lung
b) Carcinoma colon
c) Carcinoma stomach
d) Aerodigestive carcinoma
61. Gasless abdomen in X-ray is a sign of -
a) Acute pancreatitis
b) Necrotising enterocolitis
c) Ulcerative colitis
d) Intussusception
62. Which tumour is treated by hormones –
a) Carcinoma prostrate b) Carcinoma bladder
c) Carcinoma colon
d) Carcinoma pancreas
63. Ca-125 is a tumor marker for - a) Cervix b) Ovary
c) Colon
d) Breast
Answers
-
Test
Answer
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
b
a
c
c
d
d
a,b,d
d
b
d
c
d
d
None
b
d
d
a
a
b
a
d
b
b
b,d
d
b
a
b
b
d
b
b
d
a
c
d
c
d
b
c
b
b,d
c
a
b
a
a
c
a
b
a
b
b
c
b
b
a
a,b,c
d
c
a
b
References
Church J., Lowry A., Simmang C. Practice parameters for the identification and testing of patients at risk for dominantly inherited colorectal cancer - supporting documentation // Diseases of the Colon and Rectum. – 2001. – Vol.44. – No.10, October.
Manual of Clinical Oncology / Edited by D.K.Hossfeld (Chairman), C.D.Sherman, R.R.Love, F.X.Bosch. – Fifth Edition. – P. 228-252.
New trends in coloproctology / Edited by J.A.Reis Neto. – 2000. – P.337-454.
Oxford Textbook of Surgery. - http://med-lib.ru/english/index.shtml
Shankar A., Taylor I. Colorectal cancer // Surgical Treatment: Evidence-Based and Problem-Oriented / Edited by René G. Holzheimer, John A. Mannick. – Part IV. Colon.
Short Practice of Surgery / Edited by R.C.G.Russell, Norman S. Williams, Christopher J.K. Bulstrode. – 24 th Edition. – Chapter 68, chapter 71. – P. 1153-85, 1219-41.
Tjandra J.J., Kilkenny J.W., Buie W.D. et al. Practice Parameters for the Management of Rectal Cancer (Revised) // Diseases of the Colon and Rectum. – 2005. – Vol.48. – No.3, March.- P.411-423.
Ривкин В.Л., Бронштейн А.С., Файн С.Н. Руководство по колопроктологии. – М.: изд-во «Медпрактика», 2001. – Ч.4. – С.195-277.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
ACUTE INTESTINAL OBSTRUCTION (classification, clinical features, surgical tactics).
METHODS OF INTESTINAL DECOMPRESSION, ENTERAL LAVAGE.
Составитель асс. О.Г.Шахбазян
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
The student should know:
The modern theory, etiology and a pathogenesis of acute intestinal obstruction (AIO);
Classification AIO;
The pathoanatomical characteristic of various kinds of intestinal obstruction and complications;
Clinic and features of current of dynamic, mechanical and mixed forms AIO;
Stages of development AIO;
Value of tool methods in diagnostics AIO (radiological, US-researches, videolaparoscopies)
Surgical tactics at various kinds AIO;
Preoperative preparation of patients;
Volume of operations at not complicated and complicated forms AIO, sequence of surgical manipulations and algorithm of the decision of problems at operative intervention;
Conducting the postoperative period, diagnostics and treatment of early and late postoperative complications, prophylaxis and their treatment;
Mistakes in treatment of intestinal obstruction (diagnostic, medical tactical, technical, organizational) and conducting the medical documentation. The reasons of diagnostic mistakes and ways of their prevention;
Qualitative and quantity indicators of treatment AIO: a place in emergency surgical pathology, character of complications, lethality, questions of medical labour examination;
Ways of decrease in lethality at AIO. Value of early diagnostics and duly hospitalization of patients in surgical department.
-Definition
-Classification
-Etiology
-Clinical manifestations. Signs and symptoms.
-Diagnostics. Differential diagnostics
-Treatment: therapy and surgery
Definition.
Impairment of bowel content passage through the intestine can be defined as intestinal obstruction
Classification.
There are different types of intestinal obstruction:
acute;
subacute.
Chronic.
Acute intestinal obstruction can also be classified according to morpho-functional impairments into:
Dynamic.
Spastic
Paralytic (e.g. mesenteric vascular occlusion)
Mechanical.
According to the mechanism of its development intestinal obstruction can be classified into:
strangulation intestinal obstruction (incarceration, volvulus (torsion), formation of nodules)
obturation intestinal obstruction (cancer, a foreign body, a gallbladder or fecal calculas, fetobezoar, a mass of ascarids);
mixed (intussusception, adhesive).
According to the level of obstruction it can be classified into:
high (small bowel);
low (large bowel).
Etiology
Etiology of intestinal obstruction is due to a number of factors.
Mechanical obstruction develops due to anatomical factors having hereditary or acquired nature.
Predisposing factors;
dolichosigma;
cecum mobile;
peritoneal additional folds;
Acquired factors are more common than hereditary.
Acquired factors:
adhesion;
dolichosigma in elderly people;
external and internal hernia.
- intestinal and other abdominal tumors
The nature of presentation will also be influenced by whether the presentation is:
• acute;
• chronic;
• subacute.
Acute obstruction usually occurs in small bowel obstruction with sudden onset of severe colicky central abdominal pain, distension, and early vomiting and constipation.
Chronic obstruction is usually seen in large bowel obstruction with lower abdominal colic and absolute constipation, followed by distension.
Subacute obstruction implies an incomplete obstruction.
Presentation will be further influenced by whether the obstruction is:
• simple - where the blood supply is intact;
• strangulating/strangulated - where there is direct interference to blood flow, usually by hernial rings or intraperitoneal adhesions.
Clinical manifestations.
Small bowel obstruction
GENERAL CONSIDERATIONS
Presentation
Whatever its site and cause, small bowel obstruction leads to rapid accumulation of fluid and gas in the lumen proximal to the site of obstruction. This event is the result both of swallowed air and of intestinal fluid excretion. Peristalsis causes distension in the distal obstructed segment first, with gradual proximal accumulation of air and intestinal fluid. With so-called high obstruction, in areas such as the proximal jejunum, vomiting may supervene early, relieving the distension. When obstruction is distal, vomiting may not occur until late in the course of the disease.
In typical cases of acute obstruction there is initial active peristaltic activity proximal to the site. Most patients complain of crampy pain. Within a few hours this activity declines, and oedema and increasing distension mark the end of peristaltic activity; there may be no cramps or only occasional cramps. Persistent, steady pain usually indicates ischaemia or perforation. A change in the characteristics of small bowel contents is also characteristic of the later stages of obstruction. Bacterial overgrowth and stagnation make the fluid feculent, with an increase in opacity and a foul odour. Appearance of fluid of this type in the vomitus or from a nasogastric tube confirms the diagnosis of obstruction.
Obtaining a detailed history and performing a thorough examination will provide a diagnosis of underlying cause in more than three-quarters of cases. It is especially important to identify abdominal wall hernias, which frequently strangulate when surgery is delayed.
Laboratory tests are of little value beyond helping to rule out other causes of abdominal pain. The exception to this rule is the plain radiograph of the abdomen, which is especially helpful in confirming the clinical impression of obstruction, and can also, when interpreted by an experienced clinician, add additional useful information as to completeness, site, and aetiology of obstruction. Upright films may show air in the biliary or portal system and beneath the diaphragm; these are important observations with respect to timing of surgery.
Etiology
A list of the causes of intestinal obstruction is long, even if those normally only encountered during infancy and childhood are excluded. In geographic areas where life expectancy is long and surgical care readily available, at least half of the cases are the result of adhesions, usually postoperative. Hernias, whether of the abdominal wall or internal organs, are the second leading cause. Other important general causes are primary and metastatic tumours, local inflammatory processes such as appendicitis or diverticulitis of the colon, and various strictures, such as those seen in Crohn's disease. The causes and their relative incidence vary widely with geographic region.
The mechanism of the obstruction is more important than the specific aetiology, since this factor bears on the likelihood of bowel compromise. There are four general mechanisms: most dangerous are, first, volvulus with torsion and, second, incarceration in a confined space. Although volvulus can be the result of a failure of fixation of all or the distal part of the small bowel it is more commonly the result of twisting around a fixed point, as from an adhesion or tumour nodule. This event can rapidly lead to vascular compromise and infarction.
Incarceration in a fixed space is usually due to an abdominal wall hernia. Intra-abdominal defects and traps, congenital or acquired, are also sites of potential incarceration. Once entrapped, impaired venous return and torsion may rapidly lead to infarction of the segment.
Obturation of a segment of bowel, usually narrowed by a pathological process such as fibrosis or tumour growth, is the third mechanism. Such obstruction may be intermittent because of the repeated gradual passage of a bolus of intestinal contents through the stricture. A large bezoar or gallstone may obstruct a normal segment of bowel, usually the distal ileum, by this mechanism. Vascular compromise is unlikely in obturation obstruction.
The last mechanism is intussusception. In adults, it is almost always due to an intramural or mucosal lesion. It does not usually lead to ischaemia and infarction.
Non-operative measures
As a rule, mechanical small bowel obstruction is an urgent indication for surgical intervention. This practice reflects the risks of strangulation and perforation, the fact that persistence of obstruction will eventually require an operation in many cases, and the likelihood of recurrence even with spontaneous resolution.
Preoperative assessment of fluid status with rapid replacement of deficits is important. A patient whose obstruction has been identified many hours from its onset, when there has been vomiting or sequestration of large amounts of fluid in the lumen, intestinal wall and peritoneal cavity, may require administration of several litres of fluid. In these cases, restoration of an adequate urine output serves as a useful general index of adequate replacement. In older patients, especially those with a history of cardiac disease, central venous or pulmonary artery pressure monitoring may be needed. Concurrent, sometimes exacerbated, medical problems such as diabetes mellitus and cardiac impairment must be considered and managed separately.
Nasogastric suction relieves distension from air swallowing and reduces fluid passage into the small bowel; it should be instituted early in management. The use of long intestinal tubes has less justification. They do not pass readily, do not empty the stomach, and delay more definitive management. Generally, they have no useful role in the management of acute obstruction. Although exceptions may be cited, an efficiently functioning nasogastric tube is clearly preferable in most cases.
Surgical intervention
Though sometimes easy, operative intervention may be complex. The procedure requires the management of the segment of intestine at the site of obstruction, the distended proximal bowel and the underlying cause of obstruction.
If the patient has had a previous surgical incision which, with enlargement, will afford a portal for complete abdominal exploration, it should be used. This approach allows repair of all associated hernias and easy access to the most frequent site of obstruction by adhesions, which is the incision itself. It is usually wise to enter the abdomen through an extension into normal tissues to avoid injury to adherent loops.
In patients with late obstruction and in the elderly, the distended segments should be handled with care as they may easily be torn. The object is to find the junction of dilated and collapsed bowel. Though it may be preferable to follow collapsed loops proximally, this is not usually possible.
Decompression of dilated loops may be desirable to facilitate an anastomosis or closure of the abdominal wound. Closed methods of accomplishing this goal include the milking of contents back into the stomach with aspiration through a nasogastric tube. This method is usually possible without excessive trauma to the bowel only in young children. Alternatively, a long tube may be advanced from the stomach by digital manipulation into the distended loops. Finally, a sump suction device may be passed directly into the distended loops through an enterotomy controlled with a ‘purse string’ suture. Even with careful attention to prevention of local soilage, direct aspiration of enteric contents is associated with an increase in postoperative wound sepsis. Unless clearly needed, the best policy often is to omit decompression altogether.
When indicated, a simple resection of small bowel and direct anastomosis, even when the proximal bowel is distended, is safe enough. Sometimes, as with carcinomatosis or extensive pelvic adhesions, a side-to-side bypass is the better choice. Parenteral administration of antibiotics, begun preoperatively, decreases the incidence of septic complications when resection or bypass is performed.
The determination of the viability of a segment of intestine is a common problem. Generally, the opinion of an experienced surgeon after 10 to 20 min of observation suffices. To prevent early perforation or late strictures, a resection is the best choice when doubt exists. Although fluorescein injections with illumination of the surface with a Wood's lamp and detection of surface flow by Doppler devices provide scientific approaches to the diagnosis, they are neither necessary nor commonly available at the moment they are needed.
When obstruction is due to adhesions the question of whether all or only the offending adhesions should be released is unresolved. Generally, adhesions can be expected to recur when there has been any trauma to serosal surfaces. Thus, as a rule it is probably wise to divide only those adhesions involving the bowel at the site of obstruction and those that prevent restoration of the proximal and distal segments to their normal place of residence in the abdominal cavity.
Reduction of abdominal wall hernias before operation is desirable when easily accomplished. An exception is a hernia in the inguinal or femoral area; prompt operation is required. The surgeon may prefer to be able to examine the incarcerated segment of bowel through the herniorrhaphy incision before it is dropped back in. Another exception is the presence of local signs of inflammation that may indicate strangulation or perforation.
Prevention
Any laparotomy should be performed with operative measures that minimize adhesion formation, decreasing the incidence of small bowel obstruction. All reasonable steps to minimize serosal trauma should be utilized, including gentle handling and packing of intestine and avoiding the unnecessary introduction of foreign material into the peritoneal cavity. Sutures and ties involving the serosa cause small areas of tissue ischaemia and necrosis which can cause adhesions. Serosal defects should not be repaired if the underlying muscularis and submucosa are intact.
The second preventive measure, of course, is the repair of abdominal wall hernias. Any inguinal hernia that is symptomatic or is the site of occasional temporary bowel incarceration should be repaired, as should all incisional hernias.
COMPLEX PROBLEMS
Postoperative obstruction
Mechanical small bowel obstruction can complicate the postoperative course after any operative entry into the peritoneal cavity. The diagnosis is obscured by ileus and the symptoms and signs that are a usual accompaniments of a laparotomy incision.
Normally, paralysis of peristaltic function resolves within 72 h after a laparotomy involving handling of the intestine. There is then an absence of distension, and the patient reports a return of appetite along with expulsion of flatus and faeces. In cases of obstruction, normal peristaltic function may never return, or may do so only to be interrupted by an episode of obstruction. The superimposition of the signs and symptoms of obstruction on those of convalescence after laparotomy makes the diagnosis elusive.
Most cases are the result of adhesions and involve the ileum. Although the extent of adherence of peritoneal surfaces to each other is variable, the time course usually is not. By 72 h after laparotomy, extensive soft adhesions will have formed. These seem most extensive at about 10 days to 2 weeks, by which time they become dense and vascular. A gradual process of resolution then occurs; this may go on for many years, accounting for appearance of obstruction at remote times. This process of adhesion formation in some cases is abnormally vigorous and may then reflect peritoneal reaction to foreign material introduced during the operation. Sterile peritonitis can be an important contributor to a course of delayed resumption of intestinal function without actual mechanical obstruction. Obstruction by adhesions in the early period is usually the result of kinking and tensions on adherent loops of intestine rather than of obturation. The presence of a stoma or intestinal tube may contribute to these mechanical problems by offering a fixed cicatricial point. Other causes of obstruction include internal hernias and peritoneal defects after partial dehiscence of the deep layer of a wound or the peritoneal floor. An abscess involving adjacent segments of intestine can cause obstruction or can lead to localized ileus.
The clinical problem is to distinguish between cases of mechanical obstruction and those that reflect ileus prolonged by a sterile peritonitis or other factors, such as chronic narcotic use. Fortunately, except when there is a peritoneal defect, strangulation of an obstruction is rare in a postoperative patient. Careful repeated observation of the patient is paramount. Radiography offers the next best help: plain films show gas throughout the small and large bowel in most cases of ileus. In difficult cases, the use of barium will sometimes provide important information
Careful replacement of fluid and electrolytes is needed, and nutritional support may facilitate overall recovery. It is generally believed that nasogastric decompression is essential and that decompression through a long tube may be helpful; passage of such tubes is most likely to succeed in those patients with mechanical obstruction. The usefulness of long tubes in the overall management of patients is estimated to be high by some surgeons, but many do not find them useful.
The timing of surgical intervention is difficult. Although it is important to relieve mechanical obstruction promptly, operations on patients with profound ileus and in those with extensive nonobstructing adhesions are fruitless and delay recovery. No simple rule can be offered. Generally, complete obstruction, evidence of sepsis, and an unacceptably prolonged course dictate an exploratory operation. An unacceptably long course is the least useful indication.
Recurrent obstruction
The risk of strangulation and the likelihood of early recurrence usually dictate prompt operation at the first episode of obstruction. An operation for obstruction due to adhesions carries a higher likelihood of recurrence than a laparotomy for other indications. This is of the order of 20 per cent. When obstruction recurs, the possibility of a cause other than adhesions is lower, and there is perhaps more justification for a non-operative management, in the form of decompression with a nasogastric tube and careful parenteral replacement of lost fluids and electrolytes.
During any period of observation, there will be continued concern about the possibility of bowel compromise. The nature of pain is the best indicator of this complication. Plain and contrast studies are helpful in ruling out complete obstruction, which also serves as an indication for surgical relief. If the obstruction resolves, there is generally no reason for a laparotomy in the patient with recurrent obstruction due to adhesions.
There is no good way to prevent the recurrence of adhesions. Some authorities have suggested that plication of the wall or mesentery of the small bowel to form a ladderlike configuration may be helpful: there is no good evidence for the efficacy of these measures, and few surgeons use them. An in-lying long enteric tube may also produce a configuration of loops less prone to obstruction from adhesions. Such tubes should be left in place for at least 2 weeks, but their efficacy has not been clearly established.
Radiation enteritis
Injuries to the small intestine may follow radiation to any part of the abdominal cavity: many result from therapy for pelvic tumours. Although these injuries may lead to perforation with abscess formation of fistulae, the most common complication is intestinal obstruction.
During the actual course of radiation treatment, damage to the mucosa may lead to ulceration and oedema. Delayed damage to small blood vessels causes more serious complications such as progressive arteritis and eventual thrombosis. Infarction and perforation may ensue, but the more frequent result is the induction of dense adhesions containing collateral vessels, and the occurrence of fibrous strictures. Serosal surfaces of injured intestinal segments acquire a characteristic thickened, scarred, hypervascular appearance.
The cause of acute complete obstruction can only be established at the time of operation. Segments of intestine with a grossly abnormal appearance may not heal; when used for anastomosis, there is a high incidence of failure. A segment with a nearly normal appearance and satisfactory bleeding on transection can be used confidently. Microscopic examination adds little to the surgeon's impression in selecting bowel for anastomosis. Resection is the preferred management. If dissection of radiation-damaged loops of bowel out of the pelvis offers an unacceptable risk, a bypass may be selected. It is better to transect the bowel above the obstruction for an end-to-side anastomosis than to perform a side-to-side bypass in continuity.
A trial of non-surgical management is reasonable when a prior history or contrast study has established the diagnosis of radiation enteritis and obstruction is not complete. Some episodes due to obturation or oedema will resolve and may not recur. Parenteral nutrition may aid the process of resolution.
Metastatic malignant tumours
Peritoneal seeding sometimes leads to multiple narrowed segments and consequent obturation obstruction; this may occur in the absence of other terminal manifestations of the tumour. Strangulation is rare, since the loops are relatively fixed. Retroperitoneal or mesenteric deposits may contribute to the impaired motility.
Patients tend to have intermittent episodes of obturation obstruction. A minimal residue diet may reduce symptoms and acute obstruction usually clears on nasogastric suction. In patients with a relatively good prognosis, there may be a role for surgical intervention for bypass or even resection of obstructed sites. Careful evaluation with contrast studies allows selection of the smallest feasible procedure, to be performed through a limited field. Wide exploration of the abdomen is likely to be both unnecessary and counterproductive.
Superior mesenteric artery syndrome
Obstruction of the distal duodenum due to its compression between the artery and posterior structures, either the aorta or vertebral bodies, has been termed the superior mesenteric artery syndrome. Findings on plain film and contrast studies are dilatation of the stomach and duodenum with a termination by obstruction with a linear configuration at the level of the artery.
The syndrome may follow weight loss, immobilization in bed, and various operative procedures, but it also may occur spontaneously. It is seldom seen in obese patients. There appears to be a component of impaired motility in some patients and abnormalities of fixation of the ligament of Treitz have also been cited. The onset is often insidious with the gradual appearance of nausea and vomiting.
Though conservative measures should first be tried, the majority of patients eventually require surgical relief. Simple gastrojejunostomy does not relieve symptoms. Various measures can be used to adjust the position and fixation of the duodenum and proximal jejunum. Duodenojejunostomy performed through the mesocolon in a side-to-side fashion is most likely to succeed. The jejunum just beyond the ligament of Treitz should been employed in the anastomosis.
Obstruction of the colon
Obstruction of the colon as a separate clinical entity is singled out for discussion for two reasons. Firstly, it brings its own serious complications (the most dramatic being perforation), which are not directly related to the underlying cause. Secondly, it introduces special elements that influence the timing and limit the selection of procedures in managing the actual cause of obstruction.
GENERAL CONSIDERATIONS
Obstruction of the intestine at any level leads to progressive distension of the proximal bowel with fluid and gas. In the small intestine, distension may result in early vomiting if the site is proximal or in the sequestration of large amounts of fluid if it is more distal. Neither distension nor sequestration is an important elements in the presentation and course of obstruction of the colon.
The obstructed colon has less peristaltic activity, and dilatation tends to cause fewer and less severe cramps than small bowel obstruction. In the majority of patients the ileocaecal valve prevents decompression of the colon into the small intestine. This situation results in closed loop obstruction, which is especially hazardous because it can result in massive dilatation of a segment of the colon without the signs and symptoms usually associated with intestinal obstruction. Secondary dilatation of the small intestine with its consequences may follow, but it is slow to develop and is usually unimportant.
Colon obstruction presents as an emergency, especially because of the associated complication of perforation. Even when intraluminal pressure is constant, the tension on a segment of colon wall increases with an increase in diameter; the relatively larger diameter and thinner wall of the caecum and ascending colon make these the most frequent sites of perforation. In the final stages before perforation there is an embarrassment of circulation, which can also contribute to rupture of the wall. The site of perforation may be in a more distal segment of the colon, usually just proximal to an obstructing lesion such as a carcinoma.
During barium studies under the fluoroscope the normal ascending colon dilates readily up to only about 9 cm in diameter. In chronic obstruction, much larger degrees of distension may nevertheless be quite harmless. Still, when plain radiographs show distension of the ascending colon beyond 10 cm, the possibility of rupture must be considered as imminent. If the capacity of the right colon is exceeded, the serosa between the taeniae splits, perforations, usually punctuate, appear in the mucosa, and patches of haemorrhage and even infarction are also commonly observed. Perforations of this type initially lead to progressive contamination of the peritoneal cavity, but may not actually decompress the obstructed colon.
The clinical course of colon obstruction is often quite insidious. Up to 80 per cent of cases are caused by a carcinoma. Many of these patients will have experienced prior episodes of partial obstruction and may not be aware that complete obstruction has developed until 2 or 3 days have passed. Although lower abdominal cramps are usually reported, these may be mild. Cessation of the passage of stool or gas is the most frequent complaint, and an observant patient will also report abdominal distension. Physical examination shows a quiet abdomen with obvious tympany and distension, sometimes most pronounced over the ascending colon. There may be tenderness over compromised bowel, the caecum or the area proximal to a tumour. Rectal examination may disclose a low rectal tumour as the cause of obstruction. More commonly, the rectum feels capacious and empty. In the presence of a tumour or compromised bowel, there may be traces of blood. The physical examination should include a careful search for abdominal wall hernias, especially in any old surgical incisions.
Plain radiographs of the abdomen are usually helpful in colon obstruction. They may confirm or support the diagnosis and point to the site and aetiology; they can also suggest the presence of perforation by showing free air and can demonstrate a dangerously distended right colon. If an expeditious barium study is obtained, it will help identify the actual site and nature of obstruction. The barium enema examination should be done without preparation and care must be taken not to push barium above the obstruction.
In practice, it is difficult to assess the likelihood of colon perforation. When obstruction is partial, sequential evaluation of symptoms and the presence and degree of tenderness over the right colon can suggest impending perforation. If obstruction is complete, and especially if decompression into the small intestine is absent, urgent surgical exploration with decompression is the first consideration.
CAUSES OF COLON OBSTRUCTION
Carcinoma
In the more economically developed areas of the world, carcinoma is by far the most frequent cause of colon obstruction. Carcinomas of the left colon are the most likely to lead to obstruction, although those in other areas also cause obstruction, the least frequent being those of the rectum. Most patients in whom the obstruction involves the distal colon have a presentation that includes an initial period of symptoms of partial obstruction. Final obstruction reflects obturation of the narrow residual channel by faecal material. Obstruction in the right or transverse colon is more likely to occur without preceding symptoms, perhaps because of the liquid nature of the stool.
The prognosis of treated obstructing carcinomas is not very different from that of non-obstructing lesions of similar location and extent. Prognosis may be estimated by use of the Dukes' or other classification. The early operative risk is much higher in these patients especially with respect to perforation.
Diverticulitis
Complete acute colon obstruction is rarely caused by diverticular disease, although it sometimes occurs due to obturation of a strictured oedematous segment. Incomplete obstruction is more usual, and there may be associated partial or complete obstruction of an adherent loop of small intestine.
Differentiation between a carcinoma and diverticular disease of the sigmoid may be very difficult and can lead to an incomplete or delayed resection in a patient incorrectly diagnosed as having diverticulitis.
Volvulus
Volvulus of either the ileum, caecum and right colon or of the sigmoid colon almost always leads to acute obstruction. The twist of 180° or more around the mesenteric axis imparts a similar twist in the longitudinal axis; this is the immediate cause of obstruction. Because vascular compromise may result, there is a danger of perforation in neglected cases. Expert interpretation of the plain radiograph will usually establish the diagnosis. Contrast enemas may be needed when there is considerable dilatation of the proximal colon or small intestine. Volvulus of the right colon generally reflects a failure of fixation of the colon. Sigmoid volvulus is probably an acquired abnormality but is usually observed in patients with an elongated colon. Spontaneous reduction of all forms of volvulus will often occur, relieving obstruction; recurrence is the rule.
Other causes
Only a few cases of colon obstruction are due to causes other than cancer diverticulitis, and volvulus. The uncommon causes include incarceration in hernias, strictures such as those that follow vascular compromise, metastatic malignant tumours, especially those of pelvic origin, radiation strictures, and various inflammatory conditions. Adhesions, although a common cause of small bowel obstruction, are a rare cause of colon obstruction.
MANAGEMENT
General principles
Management should be directed at relief of obstruction before perforation occurs. Secondary objectives include treatment of the underlying cause and restoration of the continuity of the colon with the smallest number of operations in the shortest time feasible. Choices between the various surgical alternatives reflect the urgency of the situation, the condition of the patient, the state of the bowel to be used for anastomosis, and the potential for cure of a malignancy. Impending or actual rupture of the right colon is another major modifying factor. As with anastomosis in elective resections, tension, impaired circulation, and local contamination may all dictate a staged procedure. An anastomosis between distended ileum and normal colon is usually safe: one between distended and normal colon much less so.
Carcinoma of the colon
In the treatment of obstructing tumours in the caecum, ascending or right transverse colon, a right colectomy extended across to the transverse colon as needed is the usual procedure. Even if the colon is distended, an adequate dissection for cure is feasible, and an anastomosis of the ileum to normal and usually empty collapsed distal colon is safe. If the caecum is perforated or when other factors make the risk exceptionally high, a resection with ileostomy carries less immediate risk, although a second stage is required for reanastomosis.
If the obstructing lesion is in the region of the splenic flexure and down to the mid-sigmoid colon, a right colectomy with extension to include the lesion (a subtotal colectomy) with ileocolonic anastomosis may still be selected. In the young and healthy patient seen by an experienced surgeon subtotal colectomy is an acceptably low risk and troublesome diarrhoea afterward is the exception. A segmental resection with direct anastomosis using distended and unprepped proximal bowel carries a high risk. The safe procedure is to perform a resection with an end colostomy and with reanastomosis as a second stage. A proximal transverse colostomy or a caecectomy and ileostomy for caecal perforation with staged later section may be dictated by the general or local operating conditions. Recent reports suggest that antegrade intraoperative irrigation may be used in selected cases to establish safe conditions for a direct anastomosis.
When a tumour is present in the distal sigmoid colon or upper rectum, a single stage operation is seldom feasible. If a satisfactory dissection can be carried out under the operating conditions, a resection with an end proximal colostomy should be done. Otherwise, a proximal defunctioning colostomy alone is done. If the defunctioning colostomy can be carried out in the sigmoid colon rather than in the transverse colon, a single subsequent operation may be possible: many surgeons consider it unsafe to have two separate colon suture lines because of an increased risk of postoperative leakage. A prior colostomy remote from the operative anastomoses makes a third stage necessary.
When the obstructing tumour is at or below the peritoneal reflection, fortunately an unusual site for obstruction, a two- or three-stage operation is generally the best choice because a satisfactory dissection for the resection of a malignant tumour is often neither feasible nor safe under these conditions. If hepatic or other unresectable metastases are present, however, a Hartmann procedure (resection of the tumour with closure of the rectum and an end sigmoid colostomy) is a good single stage choice. Alternatively, a proximal transverse colostomy must be performed as a first stage, with resection of the tumour deferred until proper conditions can be secured.
In the presence of colonic obstruction there is always a risk when the caecum is not directly examined: severe damage to the wall caused by distension can result in perforation occurring even after distal decompression. Most operations should therefore include visualization of the caecum. Some minor transmural injuries can be managed by imbrication or by the placement of a caecostomy tube. Right colectomy is necessary with more advanced injuries or perforation. The site of colon obstruction and its management and the general condition of the patient determine whether an ileostomy or an ileocolonic anastomosis is indicated.
Diverticulitis
Complete obstruction from diverticulitis is, in fact, rare. In most cases, obstruction is incomplete, and an element of inflammation and oedema will respond to antibiotics and to ‘putting the colon at rest’. When non-surgical treatments fail, a primary resection can almost always be performed safely. An extensive dissection of mesenteric nodes is not necessary.
Conditions for a primary unprotected colonic or colorectal anastomosis often cannot be met. A safe colon anastomosis is one that can be left in a clean, normal field: there must be no gross faecal contamination, nor any exudate and purulent material from an abscess. Most cases of obstructive diverticulitis are best managed by primary resection and end colostomy. Continuity is restored at a second operation several weeks later. When there is a large abscess or the local inflammatory reaction precludes a safe dissection, a defunctioning transverse colostomy with drainage of the abscess as a first stage may be the only safe alternative. Another alternative in selected patients is percutaneous drainage of the abscess, with later resection if obstruction resolves.
Volvulus
Obstruction due to volvulus of the ileocaecal area requires prompt diagnosis and management in order to avoid the otherwise common complication of perforation. The diagnosis can be made on plain radiograph, but a contrast study is usually obtained. Once the diagnosis is established, an urgent laparotomy is needed. Although colonoscopic decompression or reduction by a column of barium may be feasible, the possibility of mural compromise and the likelihood of recurrence make resection with primary anastomosis the favoured management in almost all cases. In the presence of perforation with extensive peritoneal contamination or when other factors dictate a more expeditious procedure, resection with ileostomy and later reanastomosis may be the best choice.
When the caecum is intact and undamaged, caecopexy offers an alternative to resection. A long segment of the ascending colon should be secured to the left abdominal wall by raising a peritoneal flap and forming a retroperitoneal track for the colon, fixing the cut edge of the peritoneum to the anterior aspect of the colon with multiple sutures.
The management of sigmoid volvulus is in some ways quite different from that of a caecal volvulus. Perforation is rare and decompression through a rigid sigmoidoscope, perhaps by inserting a well lubricated tube through the lumen, is easily accomplished in most patients. The tube can be left in place. In chronically debilitated patients, simple decompression by this technique, when needed, may be the best choice.
If decompression is successful and definitive treatment is selected, the procedure would be an elective sigmoid resection after routine bowel preparation. An unprotected primary resection and anastomosis can usually be undertaken safely. Fixation of the sigmoid colon without resection is usually not successful because of marked redundancy and the adjacent location of the colon segments in the proximal and distal ends of the volvulus.
When decompression fails or when there is evidence of infarction or perforation, management is difficult. Reduction of the loop at operation can result in perforation and massive faecal contamination of the peritoneal cavity. If a tube is placed in the rectum before surgery, it can sometimes be manipulated into the loop by the surgeon for decompression. Primary anastomosis is seldom feasible after emergency resection. Most surgeons perform an end sigmoid colostomy with staged restoration of colon continuity. An alternative in the absence of perforation or of bowel infarction would be intraoperative decompression with the rectal tube, followed by an elective resection after proper preparation of the colon and patient.
Volvulus of the transverse colon is rare, and principles of management are the same as for caecal volvulus.
Miscellaneous causes
Numerous other anatomical and pathological causes of acute colon obstruction are encountered. Although certain principles for their management can be re-emphasized, the surgeon is left to analyse and resolve each as an individual problem. Whatever the primary site of obstruction, the possibility of caecal perforation should be considered; failure to visualize the caecum always carry a risk. Healing of any anastomosis is uncertain when it cannot be placed in a normal, uncontaminated area of the peritoneal cavity. Even a diverting proximal colostomy will not ensure healing of a questionable anastomosis. The additive risks of staged operations favour a one-stage procedure, but only under near optimal conditions of anastomosis. Finally, bypassing an obstructed segment of colon does not always preclude the risk of subsequent perforation, especially when an ileocolonic bypass is used.
The task for independent work.
Prophylaxis of an adhesive desease of a belly cavity.
Laparoscopy in diagnostics and treatment of adhesive intestinal impassability.
Enterosorbtion - mechanisms of medical action.
TESTS
1. Acute intestinal obstruction can also be classified according to morpho-functional impairments into:
1)
2)
2. According to the mechanism of its development intestinal obstruction can be classified into:
1)
2)
3)
3. According to the level of obstruction it can be classified into:
1)
2)
4. Cardinal features of obstruction:
1)
2)
3)
4)
5. Clinical features of strangulation:
1)
2)
3)
6. Principles of treatment of intestinal obstruction:
1)
2)
3)
7. The causes of obstruction may be organic:
1)
2)
3)
8. The causes of intraperitoneal adhesions:
1)
2)
3)
4)
5)
6)
9. The following are potential sites of internal herniation:
1)
2)
3)
4)
5)
6)
7)
8)
Definition of volvulus.
Answers
1. Acute intestinal obstruction can also be classified according to morpho-functional impairments into:
1) Dynamic;
-Spastic:
-Paralytic (e.g. mesenteric vascular occlusion)
2) Mechanical.
2. According to the mechanism of its development intestinal obstruction can be classified into:
1) strangulation intestinal obstruction (incarceration, volvulus (torsion), formation of nodules)
2) obturation intestinal obstruction (cancer, a foreign body, a gallbladder or fecal calculas, fetobezoar, a mass of ascarids);
3) mixed (intussusception, adhesive).
3. According to the level of obstruction it can be classified into:
1) high (small bowel);
2) low (large bowel).
4. Cardinal features of obstruction:
1) Abdominal pain
2) Distension
3) Vomiting
4) Absolute constipation
5. Clinical features of strangulation:
1) Constant pain
2) Tenderness with rigidity
3) Shock
6. Principles of treatment of intestinal obstruction:
1) Gastrointestinal drainage
2) Fluid and electrolyte replacement
3) Relief of obstruction
7. The causes of obstruction may be organic:
1) intramural - faecal impaction;
2) mural - colorectal cancer, diverticulitis, strictures (Crohn's disease, ischaemia), anastomotic stenosis;
3)extramural - adhesion (small bowel only), metastatic deposits, endometriosis
8. The causes of intraperitoneal adhesions:
1) Ischaemic areas (sites of anastomoses, reperitonealisation of raw areas, trauma, vascular occlusion)
2) Foreign material (talc, starch, gauze, silk)
3) Infection (peritonitis, tuberculosis)
4) Inflammatory conditions (Crohn's disease)
5) Radiation enteritis
6) Drugs (Practolol)
9. The following are potential sites of internal herniation:
1) the foramen of Winslow;
2) a hole in the mesentery;
3) a hole in the transverse mesocolon;
4) defects in the broad ligament;
5) congenital or acquired diaphragmatic hernia;
6) duodenal retroperitoneal fossae - left paraduodenal and right duodenojejunal;
7) caecal/appendiceal retroperitoneal fossae - superior, inferior and retrocaecal;
8) intersigmoid fossa.
10. Definition of volvulus:
A volvulus is a twisting or axial rotation of a portion of bowel about its mesentery.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
PERITONITIS (classification, clinical features, surgical tactics). INDICATIONS FOR METHODS PERITONEAL LAVAGE. INDICATIONS FOR PROGRAMMED RELAPAROTOMY. LAPAROSTOMY.
Составитель доц. Н.П.Снытко
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
THE PERITONEUM
The peritoneum is conveniently divided into two parts: the visceral surrounding the viscera and the parietal lining the rest of the cavity. The parietal portion is richly supplied with nerves and, when irritated, produces severe pain accurately localised to the affected area. The visceral peritoneum, on the other hand, is poorly supplied with nerves, and pain arising therefrom is vague and badly localised.
Surgical physiology. The peritoneal cavity is the largest cavity in the body, the surface area of its lining membrane being nearly equal to that of the skin. This veil-like, serous membrane is composed of flattened polyhedral cells, one layer thick, resting upon a thin layer of fibroelastic tissue, the two layers constituting the peritoneum. Beneath the peritoneum, supported by a small amount of areolar tissue, lies a network of lymphatics and rich plexuses of capillaries, from which all absorption and exudation must occur. In health, only sufficient peritoneal fluid, which is a pale yellow, somewhat viscid fluid containing lymphocytes and polymorphs, is secreted to ensure that the more mobile viscera glide easily. The specific gravity of the intra-abdominal contents is approximately 1-000. Mobile, gas-filled structures float upwards under the influence of posture, as does free air ('gas') in the peritoneal space.
In the erect position, when free fluid is present in the peritoneal cavity, pressure is reduced in the upper abdomen compared with the lower abdomen. When air is introduced it rises, allowing all the abdominal contents to sink.
Under the influence of decreased intra-abdominal pressure occasioned by the upward movement of the diaphragm during expiration, aided by capillary attraction, intraperitoneal fluids travel continuously in an upward direction to the subphrenic region where experimental evidence shows that fine coloured particulate matter and bacteria are absorbed rapidly into the peritoneal lymphatic network. In a matter of minutes, these coloured particles reach the lymph vessels above the diaphragm. This upward movement of intra-abdominal fluids is responsible for the subphrenic distribution of many intra-abdominal purulent collections.
When there is outpouring of large amounts of peritoneal fluid, e.g. when the contents of the stomach or duodenum escape into the peritoneal cavity through a perforation, such excess of free fluid within the peritoneal cavity unobstructed by adhesions runs downwards, largely directed by the normal peritoneal attachments.
When parietal peritoneal defects are created, healing occurs not from the edges, but by metamorphosis of mesenchymal cells in situ. Large defects heal as rapidly as small defects.
The peritoneal membrane can absorb and secrete large volume of fluid under osmotic principles: this ability to act like a semipermeable membrane is made use of by the process of peritoneal dialysis in the treatment of renal failure.
ACUTE PERITONITIS
Nearly all varieties of peritonitis are due to an invasion of the peritoneal cavity by bacteria. To such an extent is this true that when the term peritonitis is used without qualification, bacterial peritonitis is implied. Most cases of bacterial peritonitis are polymicrobial and usually both aerobic and anaerobic organisms are present. The exception is primary peritonitis (‘spontaneous' peritonitis) in which a pure infection with streptococcal, pneumococcal, or haemophilus organisms is seen.
Bacteriology
Bacteria from the alimentary canal. Usually the infection is caused by two or more strains. The commonest invaders are Escherichia coli, aerobic and anaerobic streptococci, and the Bacteroides. Less frequently Clostridium welchii is found; still less frequently staphylococci or Klebsiella pneumoniae (Friedlander's bacillus). Many of the strains of E. coli, Bacteroides, and Cl. welchii produce toxins that cause severe illness or death when they invade a large absorptive area (endotoxin shock).
The Bacteroides. Only recently has the frequency and importance of the presence of Bacteroides in the causation of peritonitis been realised. These Gram-negative, nonsporing organisms, though predominant in the lower intestine, often escape detection because they are strictly anaerobic, and slow to grow on culture media unless there is an adequate carbon dioxide tension in the anaerobic apparatus (Gillespie). In many laboratories, the culture is discarded if there is no growth in 48 hours. These organisms are resistant to penicillin and streptomycin but sensitive to metronidazole, clindamycin and lincomycin and the new cephalosporin compounds.
Since the widespread use of metronidazole (Flagyl), Bacteroides infections have diminished greatly.
Bacteria NOT from the alimentary canal. Examples are peritonitis due to the gonococcus, beta-haemolytic streptococcus, pneumococcus, and Mycobacterium tuberculosis. Since the advent of antibiotics, haemolytic streptococcal peritonitis has lost many of its dreaded lethal properties. In young girls and women, pelvic infection via the Fallopian tubes is responsible for a high proportion of 'nonalimentary' infections, e.g. gonococcus and streptococcus, but Bacteroides is also found normally in the female genital tract.
Paths of bacterial invasion of peritoneal space
1.Direct infection
- via perforation of some part of the gastrointestinal canal;
- through a penetrating wound of the abdominal wall;
- operative, e.g. drains, dialysis tubes, foreign material.
2.Local extension
- from an inflamed organ, e.g. appendicitis, cholecystitis;
- migration through gut wall, e.g. strangulated hernia;
- from or via the Fallopian tubes.
3.Blood-stream
- Part of general septicaemia.
Even an initially 'sterile' peritonitis (e.g. one due to intraperitoneal rupture of the bladder or a haemoperitoneum) so on becomes infected by transmigration of organisms from the bowel, and it is not long (often a matter of hours) before such a situation becomes a peritonitis in the usual meaning of the term. Most duodenal perforations are initially sterile for up to several hours, and many gastric perforations are also sterile at first; intestinal perforations are usually infected from the beginning. The proportion of anaerobic to aerobic organisms increases with the passage of time. Mortality reflects:
the degree and duration of peritoneal contamination;
the age of the patient;
the general health of the patient;
the nature of the underlying cause.
Natural factors that favour localisation of peritonitis
These factors are anatomical, pathological and surgical.
Anatomical. Excluding the subphrenic spaces, the greater sac of the peritoneum is divided into the pelvis, and the peritoneal cavity proper. The latter is redivided into a supracolic and an infracolic compartment by the transverse colon and transverse mesocolon, which deter the spread of infection from one to the other. When the supracolic compartment overflows, as is often the case when a gastric ulcer perforates, it does so over the colon into the infracolic compartment, or, by way of the right paracolic gutter to the right iliac fossa, and thence to the pelvis. Posture can assist in directing collections into the pelvis, as in the Sherren regime for perforated appendicitis.
Pathological. The clinical course is largely governed by the manner in which adhesions form around the affected organ. Inflamed peritoneum loses its glistening appearance and becomes reddened and velvety. Flakes of fibrin appear and cause coils of intestine to become adherent to one another and to the parietes. There is an outpouring of serous fluid rich in leucocytes and antibodies that soon becomes turbid; if localisation occurs, the turbid fluid becomes frank pus. Peristalsis is retarded in affected coils, and this helps in preventing distribution of the infection. The greater omentum, by enveloping and becoming adherent to inflamed structures, often forms a substantial barrier to the spread of infection.
Surgical. Drains are frequently used postoperatively to assist localisation (and exit) of intra-abdominal collections: their value is disputed, and certain types of drain, e.g. red rubber, are known to be both a cause of increased peritoneal exudate and a route for bacterial invasion.
Natural factors that tend to cause diffusion of peritonitis
There are several natural factors promoting diffusion:
a prime factor in the spread of peritonitis is whether it develops rapidly or slowly. If an inflamed appendix or other hollow viscus perforates early on before protective mechanisms have mobilised, there is a free gush of intestinal contents into the peritoneal cavity, which spreads over a large area almost instantaneously (Fig. 1). Perforation proximal to an obstruction, or from sudden anastomotic separation, is associated with severe generalised peritonitis and a high mortality.
the ingestion of food, or even water, by stimulating peristaltic action, hinders localisation. Violent peristalsis occasioned by the administration of apurgative or an enema, promotes a widespread distribution of an infection that might otherwise have remained localised;
when the virulence of the infecting organism is so great as to render control of the infection difficult or impossible;
in children, the omentum is small;
injudicious and rough handling of localised collections, e.g. appendix mass or pericolic abscess;
deficient natural resistance ('immune deficiency'): this can result from drugs (e.g. steroids), disease (e.g. AIDS) or infancy and old age.
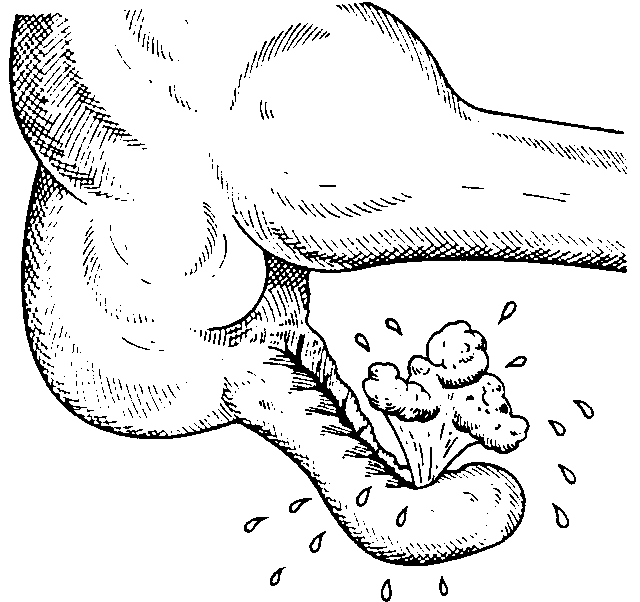
Fig. 1 Sudden perforation, especially if engendered by purgation,
often results in an immediate, widespread bacterial peritonitis.
Clinical features
Localised peritonitis is bound up intimately with the causative lesion, and the initial symptoms and signs are those of that lesion. When the peritoneum becomes inflamed the temperature, and especially the pulse rate, rise. The pain increases and usually there is associated vomiting. The most important sign is guarding and rigidity of the abdominal wall over the area of the abdomen which is involved, with a positive 'release' sign. If inflammation arises under the diaphragm, shoulder tip ('phrenic') pain may be felt. In cases of pelvic peritonitis arising from an inflamed appendix in the pelvic position or from salpingitis, the abdominal signs are often slight, deep tenderness of one or both lower quadrants alone being present, but a rectal or vaginal examination reveals tenderness, often exquisite, of the pelvic peritoneum. With appropriate treatment, localised peritonitis usually resolves. In about 20 per cent of cases an abscess follows. Infrequently, localised peritonitis becomes diffuse. Conversely, in favourable circumstances diffuse peritonitis can become localised, most frequently in the pelvis or at multiple sites within the abdominal cavity. A large collection of bile localised to the subhepatic space can remain dangerously 'silent' until a late stage.
Diffuse (syn. generalised) peritonitis.
Initial phase. There is severe pain which is made worse by moving or breathing. It is first experienced at the site of the original lesion, and spreads outwards from this point. Vomiting may occur. The patient usually lies still. Tenderness and rigidity on palpation are typically found when the peritonitis affects the anterior abdominal wall. Abdominal tenderness and rigidity are diminished or absent if the anterior wall is unaffected as in pelvic peritonitis or, rarely, peritonitis in the lesser sac. Patients with pelvic peritonitis may complain of urinary symptoms; they are tender on rectal or vaginal examination. Infrequent bowel sounds may still be heard for a short time, but they cease with the onset of paralytic ileus. The pulse rises progressively but if the peritoneum is deluged with irritant fluid there is a sudden rise. The temperature changes are variable and can be subnormal.
Intermediate phase. Peritonitis may resolve, so that the pulse slows, the pain and tenderness diminish leaving a silent, soft abdomen. (These are features that can easily mislead the observer.) The condition may localise, producing one or more abscesses, will overlying swelling and tenderness.
Terminal phase. If resolution or localisation have no occurred, the abdomen remains silent, and increasingly distends. Circulatory failure ensues, with cold, clammy extremities, sunken eyes, dry tongue, thready (irregular) pulse, drawn and anxious face (Hippocratic facies. Fig. 2). The patient finally lapses into unconsciousness. With early diagnosis and adequate treatment, this condition is rarely seen in moden surgical practice.
Diagnostic aids. Investigations will not save the need for careful confirmation of the history and physical signs, which are tendeness, guarding and rigidity with a distending silent abdomen. It unwise to rely slavishly on any single symptom or sign; not one incontrovertible.
A battery of investigations may elucidate a doubtful diagnosis. More often, they only confuse it. Peritonitis usually produces leucocytosis, often delayed for many hours.
Peritoneal diagnostic aspiration may be helpful but is usual unnecessary. After infiltrating the skin of the abdomen with local anaesthetic, fine-needle aspiration of each quadrant of the abdominal cavity is made. Bile-stained fluid indicates perforated peptic ulcer, the presence of pus indicates bacterial peritonitis; blood is aspirated in a high proportion of patients with intraperitoneal bleeding. When aspiration fails, the introduction of a small quantity of sterile physiological saline, followed after a few minutes by repeat aspiration, may produce fluid of diagnostic value.
A radiograph of the abdomen may reveal free air, or confirm the presence of dilated gas-filled loops of bowel with multiple fluid levels. If the patient is too ill for an 'erect' film to demonstrate free air collecting under the diaphragm, a lateral decubitus film is just as useful, showing gas beneath the abdominal wall.
Serum amylase estimation may uphold the diagnosis of pancreatitis, provided it is remembered that raised values are frequently found following other abdominal catastrophes, and operations, e.g. perforated duodenal ulcer.
Ultrasonography is a most valuable investigation for demonstrating the presence of intraperitoneal collections of fluid or pus. It can be combined with guided aspiration of any demonstrated collection.
An isotope scan is valuable in cases of serious difficulty.
Treatment
It cannot be stressed too strongly that in any case of doubt, early surgical intervention is to be preferred to a 'wait and see' policy; for greater numbers of patients die from delay than from an 'unnecessary' laparotomy. This rule is particularly true for postoperative peritonitis.
Treatment consists of three parts:
• general care of the patient;
• neutralisation of the local source;
• peritoneal lavage.
General care of the patient.
Intravenous fluids. These patients are often hypovolaemic and have electrolyte disturbances. The plasma volume must be restored and the plasma electrolyte concentrations corrected. The use of a central venous line is imperative for monitoring accurate fluid replacement. Plasma protein depletion may need correction – inflamed peritoneum leaks protein calamitously and continuously. If the patient's recovery is delayed for more than 7-10 days, intravenous feeding ('hyperalimentation') is required.
A nasogastric tube is passed into the stomach, which is aspirated. Intermittent aspiration is maintained until paralytic ileus resulting from peritonitis has resolved. Measured volumes of water are allowed by mouth when only small amounts are being aspirated. If the abdomen is soft and not tender, and bowel sounds return, oral feeding may be progressively introduced. It is important not to prolong the ileus by missing this stage.
Antibiotics. Administration of antibiotics prevents the multiplication of bacteria, and the release of endotoxins. As the infection is usually a mixed one, initially parenteral broad-spectrum antibiotics active against aerobic and anaerobic organisms and metronidazole may be given.
A fluid balance chart must be started at once so that daily output by gastric aspiration and urine are known, and losses from the lungs, skin, and in faeces are estimated, so that the intake requirements can be calculated and seen to have been administered.
Throughout recovery, haematocrit and serum electrolyte values and the blood urea must be checked frequently.
Analgesia. The patient, nursed in the sitting-up position, must be relieved of pain before and after operation. Once the diagnosis has been made, morphine may be given, and small doses continued for 48 hours. Freedom from pain allows early mobilisation and adequate physiotherapy in the postoperative period, to prevent atalectasis, deep-vein thrombosis and pulmonary embolism.
Oxygen. Especially if septic shock is present, special measures may be needed for cardiac, pulmonary and renal support. Administration of oxygen postoperatively can help to prevent and mitigate the effects of septic shock, especially adult respiratory distress syndrome (ARDS). If oligaemia persists despite adequate fluid replacement, both dopamine and diuretics may be needed.
Neutralisation of local source. If the cause is amenable to surgery, such as in perforated appendicitis, diverticulitis, peptic ulcer, gangrenous cholecystitis, or rarely in perforation of the small bowel, operation must be carried out as soon as the patient is fit for anaesthesia. This is usually within a few hours. In peritonitis due to pancreatitis, salpingitis, or in cases of primary peritonitis of streptococcal or pneumococcal origin, conservative treatment is the procedure of choice (if the diagnosis can be made with certainty).
Peritoneal lavage. In surgery for general peritonitis it is essential that after the cause has been dealt with, the whole peritoneal cavity should be explored with the sucker and mopped dry, if necessary until all seropurulent exudate is emoved. The use of a large volume of antibiotic saturated saline (1-2 litres) has been shown to be very effective for 'cleaning' the peritoneum.
Prognosis
With modern treatment diffuse peritonitis carries a mortality of about 10 per cent. The lethal factors are:
• bacterial toxaemia;
• paralytic ileus;
• bronchopneumonia;
• electrolyte imbalance;
• renal failure;
• undrained collections;
• bone-marrow suppression;
• 'multisystem breakdown'.
Post-operative peritonitis has a mortality of at least 50 per cent. Faecal peritonitis has a mortality of 75 per cent. Peritonitis associated with appendicitis, perforated peptic ulcer or bile-leakage are much less dangerous (mortality less than 10 per cent).
Complications of peritonitis
All the complications of a severe bacterial infection are possible, but the special complications of peritonitis are as follows.
Acute intestinal obstruction due to peritoneal adhesions. This usually gives central colicky abdominal pain with radiological evidence of gas and fluid levels confined to the upper portion of the small intestine. It is more common with localised peritonitis. It is essential to distinguish this from paralytic ileus.
Paralytic ileus. There is usually little pain and gasfilled loops with fluid levels are seen distributed throughout the small and large intestines on the radiograph. In intestinal obstruction, bowel sounds are increased. In paralytic ileus bowel sounds are reduced or absent.
Residual abscesses. Abscess formation following local or diffuse peritonitis usually occupies one of the situations shown in Fig,2, The symptoms and signs of a purulent collection may be very vague and consist of nothing more than lassitude, anorexia, and failure to thrive; pyrexia (often low-grade), tachycardia, leukocytosis, and localised tenderness are also common. Later on a palpable mass may develop. When palpable, an intraperitoneal abscess should be monitored marking out its limitations on the abdominal wall, meticulous daily examination.
Fig.2 Common situations for residual abscesses: (1) subphrenic(2) paracolic; (3) right iliac fossa(4) elvic.
In the majority of cases with the aid of antibiotic treatment, the mass becomes smaller and smaller, and finally is impalpable. In others, the abscess fails to resolve, or becomes large in which event it must be opened. In many situations, by waiting a few days, the abscess becomes adherent to the abdominal wall, so that it can be drained without opening the general peritoneal cavity. For deeper-situated residual collections, percutaneous placement of drainage tubes under fluoroscopic or ultrasonographic control can be very effective. Open drainage of an intraperitoneal collection should carried out by cautious blunt finger exploration to minimise the risk of an intestinal fistula.
PELVIC ABSCESS
The pelvis is the commonest site of an intraperitoneal abscess, because the vermiform appendix is often pelvic in position and also the Fallopian tubes are frequent loci of infection. A pelvic abscess can also occur as a sequel to any case of diffuse peritonitis and is a common sequel of anastomotic leakage following large bowel and rectal surgery. Pus can accumulate in this area without serious constitutional disturbance, and unless the patient is examined carefully from day to day, such abscesses may attain considerable proportions before being recognised. The most characteristic symptoms of a pelvic abscess are diarrhoea and the passage of mucus in the stools. It is no exaggeration to say that the passage of mucus occurring for the first time in a patient who has, or is recovering from, peritonitis, is pathognomonic of pelvic abscess. Rectal examination reveals a bulging of the anterior rectal wall which, when the abscess is ripe, becomes softly cystic. Left to nature, a proportion of abscesses burst into the rectum, after which the patient nearly always recovers rapidly. If this possible happy termination does not readily occur, the abscess should be drained deliberately. In women, vaginal drainage through the posterior fornix is often chosen. In other cases, where the abscess is definitely pointing into the rectum, rectal drainage (Fig.3) is employed. If any uncertainty exists as to the presence of pus, either an ultrasound examination aspirating needle introduced into the collection through the rectal wall or through the abdominal wall (after emptying the bladder by a catheter) will settle the question. Laparotomy is almost never necessary.
Provided the abscess is shut off from the general peritoneal cavity, a point which can be ascertained undeniably when the abdomen has been opened, rectal drainage of a pelvic abscess is far preferable to suprapubic drainage, which breaks down nature's barriers and exposes the general peritoneal cavity to the dangers of spreading infection.
Fig.3 Opening a pelvic abscess into the rectum.
SUBPHRENIC ABSCESS
Anatomy. The complicated arrangement of the peritoneum results in the formation of four intraperitoneal and three extraperitoneal subphrenic spaces in which pus may collect. Three of these spaces are on either side of the body, and one approximately in the midline
(Figs 4 and 5).
Left superior (anterior) intraperitoneal ('left subphrenic'), bounded above by the diaphragm, behind by the left triangular ligament and left lobe of the liver, the gastrohepatic omentum and anterior surface of the stomach. To the right is the falciform ligament, and to the left the spleen, gastrosplenic omentum, and diaphragm. The common cause of an abscess here is following operations on the stornach, the tail of the pancreas, the spleen or the splenic flexure of the colon or in diverticulitis.
Left inferior (posterior) intraperitoneal ('left subhepatic') is another name for the ‘lesser' sac. The commonest type of suppuration here is the pancreatic pseudocyst. In practice, perforated gastric ulcer rarely causes a collection here, because the potential space is obliterated by adhesions.
Right superior (anterior) intraperitoneal ('right subphrenic'), which lies between the right lobe of the liver and the diaphragm. It is limited posteriorly by the anterior layer of the coronary and the right triangular ligaments, and to the left by the falciform ligament.
Common causes here are perforating cholecystitis, a perforated duodenal ulcer, a duodenal cap 'blow out' and appendicitis.
Right inferior (posterior) intraperitoneal ('right subhepatic') lies transversely beneath the right lobe of the liver in Rutherford Morison's pouch. It is bounded on the right by the right lobe of the liver and the diaphragm. To the left is situated the foramen of Winslow, and below this lies the duodenum. In front are the liver and gallbladder, and behind, the upper part of the right kidney and diaphragm. The space is bounded above by the liver, and below by the transverse colon and hepatic flexure. It is the deepest space of the four and the commonest site of a subphrenic abscess which usually arises from appendicitis, cholecystitis, a perforated duodenal ulcer or following upper abdominal surgery.
Extraperitoneal. There are three of these:
• Right and left extraperitoneal which are terms given to perinephric abscesses.
• Midline extraperitoneal which is another name for the 'bare' area of the liver which may develop an abscess in amoebic hepatitis (the commonest cause) or it may be a pyogenic liver abscess.
Fig. 4. Intraperitoneal subphrenic abscesses on transverse
section. (1) the left superior space; (2) left inferior space (lesser sac);
(3) right superior space which becomes shut oft by adhesions from (4)
right inferior space.
Fig. 5. Intraperitoneal subphrenic abscesses on sagittal section.
(1) left superior erior) abscess (left subphrenic'); (2) left inferior
(posterior) abscess (left subhepatic'); (3) right superior (anterior)
abscess ('right subphrenic'); (4) right inferior (posterior) abscess ('right
subhepatic').
Clinical features. The symptoms and signs of subphrenic infection are frequently unspecific, and it is well to remember the aphorism, 'Pus somewhere, pus nowhere else, pus under diaphragm'.
Symptoms. A common history is that when some infective focus in the abdominal cavity has been dealt with, the condition of the patient improves temporarily, but after an interval of a few days or weeks, symptoms of toxaemia reappear. The condition of the patient steadily, and often rapidly, deteriorates.
Sweating, wasting, and anorexia are present. There is sometimes epigastric fullness and pain, or pain in the shoulder on the affected side, owing to irritation of sensory fibres in the phrenic nerve, referred along the
descending branches of the cervical plexus. Persistent hiccup may be a presenting symptom.
Signs. A swinging pyrexia is usually present, unless antibiotics or drugs (steroids) have interfered. If the abscess is anterior, abdominal examination will reveal some tenderness, rigidity, or even a palpable swelling.
Sometimes the liver is displaced downwards, but more often it is fixed by adhesions. Examination of the chest is important, and in the majority of cases collapse of the lung or evidence of basal effusion or empyema is to be found.
Accessory investigations.
Blood count. A relative and absolute leucocytosis is usual.
A plain radiograph sometimes demonstrates the presence of gas (Fig.6) or a pleuralffusion. On screening, the diaphragm is often seen to be elevated (so-called 'tented' diaphragm) and its movements impaired.
Ultrasonography and CT, NMR and scinti-scanning have proved strongly contributory to diagnosis (Fig. 9).
Differential diagnosis. Pylephlebitis, tropical abscess, pulmonary collapse, and empyema give rise to most of the diagnostic difficulties.
Treatment. The clinical course of suspected cases is watched, and blood and radiological examinations are made at suitable intervals. If suppuration seems probable, intervention is indicated. If skilled help is available it is frequently possible to insert a percutaneous drainage tube 'blindly' under combined ultrasonic and fluoroscopic control. The same tube can be used to instil antibiotic solutions into the abscess cavity. To pass an aspirating needle at the bedside through the pleura and diaphragm invites catastrophic spread of the infection into the pleural cavity.
If a swelling can be detected in the subcostal region or in the loin, an incision is made over the site of maximum tenderness, or over any area where oedema or redness is discovered. The parietes usually form part of the abscess wall, so that contamination of the general peritoneal cavity is unlikely.
If no swelling is apparent, the subphrenic spaces should be explored either by an anterior subcostal approach or from behind after removal of the outer part of the 12th rib according to the position of abscess as indicated on a lateral radiograph (see above). With the posterior approach the pleura must not be opened, and after the fibres of the diaphragm have been separated a finger is inserted beneath the diaphragm so as to explore the adjacent area. Thus both approaches must be extraserous to avoid dissemination of pus into the peritoneal or pleural cavities (Barnard).
When the cavity is reached, all the fibrinous loculi must be broken down with the finger and one or two drains or drainage tubes must be fully inserted. Drains are withdrawn gradually during the next 10 days and the closure of the cavity checked by radiological sinograms (as also after percutaneous drainage).
SPECIAL FORMS OF PERITONITIS
Postoperative peritonitis. The patient is ill, with raised pulse and peripheral circulatory failure. Following an anastomotic dehiscence, the general condition of a patient is far more grave than if the patient had suffered leakage from a perforated peptic ulcer with no preceding operation. Local symptoms and signs are less definite, particularly if steroids are being given,
Abdominal pain may not be prominent, tenderness may be masked by the presence of a recent wound.The patient's deterioration may be wrongly attributed to cardiopuirnonary collapse, which is usually concomitant.
Peritonitis follows abdominal operations more frequently than is realised. The principles of treatment do not differ from those of peritonitis of other origin. Antibiotic therapy alone is inadequate; no antibiotic can stay the onslaught of bacterial peritonitis due to leakage from a suture line, which must be dealt with surgically.
In patients under treatment with steroids. Pain is frequently slight or absent. Physical signs are similarly vague and misleading.
In children. The diagnosis is in some ways more difficult, in other ways more easy, than in adults. If a history can be taken it is plain and unembroidered. Any physical signs elicited, by a gentle, patient, and sympathetic examiner are meaningful. The 'assistance' of an overanxious mother can be a serious impediment: conversely, the opinion of an experienced nurse can be fundamental in making the diagnosis.
In senile patients. These can be as fractious as, children and unable to give a reliable history. Abdominal tenderness is usually well localised, but guarding and rigidity are less marked because the abdominal muscles are thin and weak.
Bile peritonitis. Unless there is reason to suspect that bile duct was damaged, it is improbable that bile has a cause of peritonitis will be thought of until the
• following biliary surgery, e.g. damage to the common bile duct, slipping of a ligature on the cystic duct, leakage from a divided accessory bile duct in the gallbladder bed or dislodgement of a T-tube drain in the early postoperative phase;
• instrumental perforation at endoscopic retrograde cholangiopancreatography or placement of a bile-duct stent;
• following perforation or gangrene of the gallbladder or leakage from a choledochus cyst;
• following gastroduodenal surgery, e.g. duodenal cap 'blow out' or leakage from a suture line.
Unless the bile has extravasated slowly, when the collection becomes shut off from the general peritoneal cavity, there are signs of diffuse peritonitis with a degree of shock. After a few hours a tinge of jaundice is not unusual. Local drainage, and when necessary suprapubic peritoneal drainage, is imperative, and if performed early enough, these measures will save the patient's life. When bile is seen issuing from a perforation of some part of the biliary tree, a drainage tube should be passed through the opening and secured there. Infected bile is more lethal than sterile bile. The gallbladder, if present, hould be drained. A 'blown' duodenal stump must be drained as it is too oedematous to repair, but sometimes it can be covered
by a jejunal patch. If the patient is jaundiced the surgeon must ensure that the abdomen is not closed until any possible cause of obstruction to a major bile duct has been either excluded or relieved.
Meconium peritonitis. Meconium is a sterile mixture of epithelial cells, mucin, salts, fats, and bile, and is formed when the fetus commences to swallow amniotic fluid. By the third month of intrauterine life, the upper third of the small intestine has become filled with meconium; by the fourth month, the accumulation has reached the ileocaecal valve; during the remainder of intrauterine life the colon becomes increasingly filled.
Meconium peritonitis is an aseptic peritonitis which develops late in intrauterine life or during, or just after, delivery. Meconium enters the peritoneal cavity through an intestinal perforation, and in over 50 per cent of cases the perforation is the result of some form of neonatal intestinal obstruction; in the remainder no cause for the perforation is discernible. When meconium, which is sterile, enters the peritoneal cavity an exudate is secreted that organises rapidly; matting of intestinal loops occurs, and in many cases in a matter of weeks the extruded meconium becomes calcified.
Meconium remains sterile until about 3 hours after birth; thereafter, unless the perforation has become sealed, sterile meconium peritonitis gives place to acute bacterial peritonitis which, unless treated promptly, is rapidly fatal.
Clinical features. Meconium peritonitis should always be considered when a baby is born with a tense abdomen. There is vomiting, and failure to discharge meconium. The differential diagnosis between neonatal intestinal obstruction and peritonitis is, in many cases, virtually impossible; indeed, in half the cases both are present. Free fluid in the peritoneal cavity is often sufficient to give a fluid thrill. In many cases, there are exocrine secretory deficiencies elsewhere, e.g. lungs, pancreas, salivary glands (syn. 'mucoviscidosis'). Bronchial obstruction by mucus plugs can be an immediate cause of fatal pneumonia. In some cases the mother may have been identified as having the abnormal genes responsible for the condition.
Radiography. Free air in the peritoneal cavity, an abundant quantity of abdominal fluid, fluid levels, calcification (often most distinct on the surface of the liver or the spleen, and most readily seen in a lateral view) are characteristic findings, all of which are unlikely to be present in every case. Meconium peritonitis has been diagnosed by radiography of the fetus in utero 2days before birth.
Treatment. The prognosis is bad, but recovery has followed prompt operation in some cases. The greatest
chance of survival is in those patients who have an intestinal perforation but no intestinal obstruction, in which case closing the perforation and draining the peritoneal cavity is all-sufficient, and can be performed expeditiously. Intestinal lavage can prevent reformation of meconium bolus' obstruction, and supplements of pancreatic exocrine enzymes may be necessary until adult life. If there is an associated pulmonary problem, the condition requires special treatment (e.g. 02, bronchial lavage, nebulisers and long-term use of antibiotics).
Pneumococcal peritonitis. There are two forms of this disease: (1) primary, and (2) secondary to pneumonia.
Primary pneumococcal peritonitis is much the more common. The patient is often an undernourished girl between 3 and 6 years of age, and it is probable that the infection sometimes occurs via the vagina and Fallopian tubes, for pneumococci have been cultured from patients' vaginas. At other times, and always in males, the infection is blood-borne from the upper respiratory tract or the middle ear. After the age of 10 years, pneumococcal peritonitis is most unusual. Children with nephritis are more liable to this condition than others. During the past 30 years, the incidence of pneumococcal peritonitis has declined greatly and the condition is now rare. Perhaps this is on account of the greater cleanliness and higher standard of living of what were the poorer classes, as well as early use of antibiotics to treat infections.
Clinical features. The onset is sudden, and the earliest symptom is pain localised to the lower half of the abdomen. The temperature is raised to 39.8°C or more, and there is usually frequent vomiting. After 24 to 48 hours profuse diarrhoea, occasionally bloodstained, is characteristic. There is usually increased frequency of micturition. The last two symptoms are due to severe pelvic peritonitis. Herpes on the lip or nostril is often present. In acute forms of the disease, even in cases where there is no involvement of a lung, there is a tinge of cyanosis of the lips and cheeks, and movement of the alae nasi is often discernible. On examination rigidity is usually bilateral, but is less than in most cases of acute appendicitis with peritonitis.
Differential diagnosis. A leucocytosis of 30 OOO/mm3 (30 x 10"/l) or more with approximately 90 per cent polymorphs speaks more for pneumococcal peritonitis than appendicitis. Even so, it is often impossible, especially in males, to exclude perforated appendicitis. The other condition which is extremely difficult to differentiate from primary peritonitis in its early stage is pneumonia. An unduly high respiratory rate and the absence of abdominal rigidity are the most important signs supporting the diagnosis of pneumonia, which is usually clarified by a radiograph of the thorax.
Treatment. Early operation is always required. After correcting dehydration and electrolyte imbalance, a short paramedian incision is made over the right rectus abdominis. The peritoneum is incised. Should the exudate be odourless and sticky, the diagnosis of pneumococcal peritonitis is practically certain, but it is desirable to perform a routine laparotomy to exclude other lesions. Assuming that no other cause for the peritonitis is discovered, some of the exudate is removed with a syringe, and sent to the laboratory for culture and sensitivity tests. Thorough peritoneal lavage is carried out and the incision closed. The patient is returned to bed and antibiotic and fluid replacement therapy continued. Gastrointestinal suction drainage is essential. Recovery is usual.
Primary streptotoccal peritonitis of infants and children is rather more frequent than the foregoing but still uncommon. When a streptococcus is the infecting organism, the peritoneal exudate is thin, slightly cloudy, and contains flecks of fibrin. From the standpoints of clinical aspects and treatment, streptococcal peritonitis in infants and children does not differ from those detailed in the account of pneumococcal peritonitis (see above), but the mortality is higher. An intravaginal foreign body (e.g. a toy) should always be looked for in female patients.
Idiopathic streptococcal and staphylococcal peritonitis in adults is fortunately rare, for, before the antibiotic era, it was nearly always fatal, and the mortality is still very high. Rightly, in early cases the abdomen is opened, usually on a diagnosis of acute appendicitis. In streptococcal peritonitis the peritoneal exudate is odourless, thin, contains small flecks of fibrin, and may be bloodstained. In these circumstances pus is removed by suction, the abdomen closed with suprapubic drainage, and the measures detailed in the conservative treatment of peritonitis carried out. The use of intravaginal tampons has led to an increased incidence of Staph. aureus infections: these can be associated with 'toxic shock syndrome' and disseminated intravascular coagulopathy.
Peritonitis following abortion/parturition. The abortionist has usually pushed an instrument through the uterine vault and streptococcal peritonitis follows. When peritonitis follows puerperal infection, it is a notifiable disease. It is more common after first deliveries. Rigidity is seldom much in evidence; this, in part, is due to the stretched condition of the abdominal musculature. The lochia may be offensive but not necessarily so. Diarrhoea is common.
Treatment. Provided the infection is limited strictly to the pelvis, the correct treatment is rest for the alimentary canal, intravenous fluids, the required antibiotic, and attention to electrolyte balance. Posterior colpotomy may be necessary if a pelvic abscess forms. If the peritonitis is generalised, the patient is usually extremely ill and drainage is advisable. This is best carried out by making a small suprapubic incision under local anaesthesia and inserting a drain. This can be done with the patient in bed, if necessary. In the preantibiotic era, the mortality of general peritonitis following parturition or abortion was at least 50 per cent; with antibiotic therapy and timely operation, the mortality has fallen to less than 10 per cent (Brews).
Periodic peritonitis is characterised by abdominal pain and tenderness, mild pyrexia, polymorphonuclear leucocytosis and, occasionally, pain in the thorax and joints. The duration of an attack is 24 to 72 hours, when it is followed by complete remission, but exacerbations recur at regular intervals. Most of the patients have undergone appendicectomy in childhood. The disease, often familial, is limited principally to Arabs, Armenians, and Jews; other peoples occasionally are affected. At laparotomy, which may be necessary to exclude other causes, the peritoneum - particularly in the vicinity of the spleen and the gallbladder - is inflamed. There is no evidence that the interior of these organs is abnormal.
Differential diagnosis. Patients with abdominal epilepsy do not have positive physical signs of pyrexia, and their attacks are usually controlled by anticonvulsive medication. The aetiology of periodic peritonitis is unknown, and no form of treatment has been found to be of the slightest avail. Usually, children are affected, but it is not rare for the disease to make its first appearance in early adult life, when females out- number males by two to one. Exceptionally, the disease becomes manifest in patients over 40 years of age.
TUBERCULOUS PERITONITIS
Acute tuberculous peritonitis. Tuberculous peritonitis sometimes has an onset that resembles so closely acute peritonitis that the abdomen is opened. Straw-coloured fluid escapes, and tubercles are seen scattered over the peritoneum and greater omentum. Early tubercles are greyish and translucent. They soon undergo caseation, and appear white or yellow, and are then less difficult to distinguish from carcinoma. Tubercles occasionally simulate fat necroses or the nodules of peritoneal carcinomatosis. On opening the abdomen and finding tuberculous peritonitis, the fluid is evacuated, some being retained for bacteriological study. A portion of the diseased omentum is removed for histological confirmation of the diagnosis, and the wound closed without drainage. At other times, although acute abdominal symptoms arise, the presence of ascites makes the diagnosis of acute tuberculous peritonitis reasonably evident.
Chronic tuberculous peritonitis. Although the incidence of turberculous peritonitis has declined in Britain, in many parts of the world where measures for eradicating tuberculosis (especially the disease in cows) are enforced less strictly, the condition still occurs.
Presentation. Abdominal pain is present in 90 per cent, fever in 60 per cent, loss of weight in 60 per cent, ascites in 60 per cent, night sweats in 37 per cent, and abdominal mass in 26 per cent.
Origin of the infection
Infection originates from:
• tuberculous mesenteric lymph nodes;
• tuberculosis of the ileocaecal region;
• a tuberculous pyosalpinx;
• blood-borne infection from pulmonary tuberculosis, usually the 'miliary' but occasionally the 'cavitating' form.
There are four varieties of tuberculous peritonitis: ascetic, encysted, fibrous and purulent.
Ascitic form. The peritoneum is studded with tubercles, and the peritoneal cavity becomes filled with pale, straw-coloured fluid. The onset is insidious. There is loss of energy, facial pallor, and some loss of weight. The patient is usually brought for advice because of enlargement of the abdomen. Pain is often completely absent; in other cases there is considerable abdominal discomfort which may be associated with constipation or diarrhoea. On inspection, dilated veins can be seen coursing beneath the skin of the abdominal wall. Shifting dullness can be elicited readily. In the male child, congenital hydroceles sometimes appear, due to the patent processi vaginales becoming filled with ascitic fluid from the peritoneal cavity. Because of the increased intra-abdominal pressure, an umbilical hernia commonly occurs. On abdominal palpation, a transverse solid mass can often be detected. This is rolled-up greater omentum infiltrated with tubercles.
Diagnosis is seldom difficult, except when it occurs in an acute form or when it first appears in an adult, in which case it has to be differentiated from other forms of ascites, especially from malignant secondary deposits. A positive Mantoux test in a child with ascites strongly suggests, and a negative test is good evidence against, tuberculosis. In adults this test is of negligible value. The diagnosis of tuberculous peritonitis having been made, it is always important to look for tuberculous disease elsewhere, and in this respect the possibility of tuberculous salpingitis in females should be remembered. A chest radiograph should always be taken before a laparotomy is performed.
The fluid is pale yellow, usually clear, and rich in lymphocytes.
The specific gravity is comparatively high, often 1.020 or over. Even after centrifugation, rarely can M. tuberculosis be found, but presence can be demonstrated by culture and confirmed by guineapig inoculation.
Treatment. If the general condition is good, the patient can return home and, if an adult, to light work, before the course of chemotherapy has been completed.
Encysted (syn. loculated) form is similar to the above, but one part of the abdominal cavity alone is involved. This produces a localized intra-abdominal swelling which gives rise to difficulty in diagnosis.
In a female above the age of puberty, when the swelling is in the pelvis, an ovarian cyst will probably be diagnosed. In the case of a child, it is sometimes difficult to distinguish the swelling from a mesenteric cyst. For these reasons laparotomy is often performed, and if an encapsulated collection of fluid is found, it is evacuated and the abdomen is closed. The general treatment already detailed is required, but the response to this treatment is more rapid. Late intestinal obstruction is a possible complication.
Fibrous (syn. plastic) form is characterised by the production of widespread adhesions, which cause coils of intestine, especially the ileum, to become matted together and distended. These distended coils act as a 'blind loop' and give rise to steatorrhoea, wasting and attacks of abdominal pain. On examination, the adherent intestine with omentum attached, together with the thickened mesentery, may give rise to a palpable swelling or swellings. The first intimation t of the disease may be subacute or acute intestinal obstruction. Sometimes the cause of the obstruction can be remedied easily by the division of bands. Lateral anastomosis between an obviously dilated loop and a collapsed loop of small intestine should not be done, as the 'blind loop' syndrome is a certain outcome. If the adhesions are accompanied by fibrous strictures of the ileum as well, it is best to excise the affected bowel, provided not too much of the small intestine needs to be sacrificed. If adhesions only are present, a plication may be performed. Chemotherapy after adequate surgery will rapidly cure the condition.
Purulent form is rare. When it occurs, usually it is secondary to tuberculous salpingitis. Amidst a mass of adherent intestine and omentum, tuberculous pus is present. Sizeable cold abscesses are wont to form, and point on the surface, commonly near the umbilicus, or burst into the bowel. In addition to prolonged general treatment, operative treatment may be necessary for the evacuation of cold abscesses and possibly for intestinal obstruction. If the patient survives long enough to overcome the infection, it may be possible to close a faecal fistula, which otherwise usually persists because of obstruction distal to it. Closure must therefore be combined with some form of anastomosis between the segment of intestine above the fistula and an unobstructed area below. The prognosis of this variety of tuberculous peritonitis is relatively poor.
SCLEROSING PERITONITIS
Practolol, a b-adrenergic blocking agent used in the treatment of cardiovascular disorders, has been found to be associated with the late development of a sclerosing condition in the peritoneum, which may cause intestinal obstruction. At laparotomy, the condition resembles plastic tuberculous peritonitis. It may be confused with mesothelioma or carcinoid syndrome. Lysis of the adhesions is indicated. The condition may cause recurrent obstruction. Since the development of better drugs, this condition is no longer seen.
PERITONEAL BANDS AND ADHESIONS
Congenital bands and membranes occur in the peritoneum as described in textbooks of anatomy. None of them causes intestinal obstruction except an obliterated vitellointestinal duct.
Talc granuloma. Talc (silicate of magnesium) should never be used as a lubricant for rubber gloves for it is a cause of peritoneal adhesions and granulomas in the Fallopian tubes. Potassium bitartrate, which is completely soluble, is free from these serious objections.
TESTS
1. Commonest site of an intraperitoneal absecess is-
a) Subphrenic
b) Paracolic
c) Paraappendix
d) Pelvic
2. Treatment of pouch of Douglas abscess is -
a) Laparotomy
b) Posterior colpotomy
c) Antibiotics
d) Extraperitoneal drainage
3. Early surgery is indicated in -
a) Amoebiasis peritonitis
b) Biliary
c) Typhoid peritonitis
d) All
4. Most common site for intra abdominal abscess following laparotomy is -
a) Subhepatic
b) Subphrenic
c) Pelvic
d) Paracolic
5. Most common cause of generalised peritonitis in a 40 year old adult male is -
a) Enteric perforation
b) Ruptured liver abscess
c) Duodenal Ulcer perforation
d) Perforated Ca stomach
6. Correct about subphrenic abscess is
a) Rarely chest symptoms
b) Toxaemia
c) Rarelly toxaemia
d) No sign and symptoms
7. Odourless peritoneal fluid is noticed in -
a) Perforated petic ulcer
b) Perforated ileum
c) Perforated appendix
8. Best investigation for air in peritoneal cavity is -
a) USG
b) Laparotomy
c) Laparoscopy
d) X-ray abdomen-erect view
e) CT scan
9. Colpotomy is done to treat -
a) Ischeorectal abscess
b) Pelvic abscess
c) Appendicular abscess
d) Perianal abscess
10. Least irritant fluid to peritoneum -
a) Blood
b) Urine
c) Bile
d) Pancreatic fluid
e) Pus
11. The commonest organism seen in peritonitis is -
a) Escherichia coli
b) Clostridium welchii
c) Staphylococci
d) Klebsiella
12. Clinical sign of peritonitis is –
a) Coffee-grounds vomit
b) Sense of fullness in the abdomen
c) Abdominal pain
d) Melena
13. Symptom of peritonitis is –
a) Frog abdomen
b) Board-like abdomen
c) Soft abdomen
d) Abdominal murmur
14. Rebound tenderness symptom is –
a) Symptom of reflex constipation
b) Only abdominal painfulness
c) Guarding of abdominal muscles
d) Shchotkin-Blumberg symptom
15. Sign of peritonitis in its later stage isn’t –
a) Hypoproteinemia
b) Secondary constipation
c) Septic shock (SIRS)
d) Increase of intestinal peristalsis
16. What of investigations is particularly important for the proper diagnostics of peritonitis before the operation?
a) Physical examination
b) USG
c) Laboratory investigations
d) X-ray abdomen-erect view
17. What are functions of the peritoneum? (To answer in writing)
a)
b)
c)
d)
e)
18. What are causes of a peritoneal inflammatory exudate? (To answer in writing)
a)
b)
c)
d)
e)
19. What are paths to peritoneal infection? (To answer in writing. To write examples.)
a)
b)
c)
d)
e)
Answers
№ вопроса |
Ответ |
1 |
D |
2 |
B |
3 |
D |
4 |
A |
5 |
C |
6 |
B |
7 |
A |
8 |
D |
9 |
B |
10 |
A |
11 |
A |
12 |
C |
13 |
B |
14 |
D |
15 |
D |
16 |
A |
17. What are functions of the peritoneum? (To answer in writing)
a) Pain perception (parietal peritoneum)
b) Visceral lubrication
c) Fluid and particulate absorbtion
d) Inflammatory and immune responses
e) Fibrinolytic activity
18. What are causes of a peritoneal inflammatory exudate? (To answer in writing)
a) Bacterial infection, e.g. appendicitis, tuberculosis
b) Chemical injury, e.g. bile peritonitis
c) Ischaemic injury, e.g. strangulated bowel, vascular occlusion
d) Direct trauma, e.g. operation
e) Allergic reaction, e.g. starch peritonitis
19. What are paths to peritoneal infection? (To answer in writing. To write examples.)
a) Gastrointestinal perforation (for example perforated ulcer, diverticular perforation)
b) Exogenous contamination (for example drains, open surgery, trauma)
c) Transmural bacterial translocation, no perforation (for example inflammatory bowel disease, appendicitis, ischaemic bowel)
d) Female genital tract infection (for example pelvic inflammatory disease)
e) Haematogenous spred (rare, for example septicaemia)
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
WOUNDS AND SURGICAL INFECTION IN WOUNDS. ULCERS OF THE LEG (classification, management), PRESSURE SORES (decubitus ulcers) AND ISCHAEMIC ULCERS (classification, prevention, treatment)
Составитель ассистент О.Г.Шахбазян
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
Motivation.
Annually in the country than 12 million patients with bruises, wounds, crises of bones of the top and bottom extremities is registered more, that very often leads to development of purulent processes. In the general structure of surgical diseases the surgical infection is observed at 35-45 % of patients and proceeds in the form of sharp and chronic illnesses or a suppuration of posttraumatic and postoperative wounds (A.M. Svetuhin, UL. Amiraslanov, 2003).
The problem of a surgical infection remains to one of actual in modern surgery. It is connected both with high frequency of case rate, and with essential material inputs that translates this problem from the category medical in the category social and economic, i.e. the state problems. The problem has got the special importance in connection with growth of number of technogenic and natural accidents, military conflicts and acts of terrorism.
Owing to the big social and economic importance of their decision it is necessary to carry questions of an intrahospital infection which development essentially increases lethality, to number of priority questions terms of stay of patients in a hospital and demands significant additional charges on treatment. Today an intrahospital infection transfer from 12 up to 22 % of patients, lethality among which exceeds 25 %.
The retrospective analysis of the reasons of development of heavy purulent complications at 15000 patients translated from various hospitals on treatment in specialized branch of purulent surgery of Institute of surgery of a name of A.V.Vishnevskogo of Russian Academy of Medical Science (Moscow), has revealed in many cases unjustified use of antibiotics (benzilpenicillin, semisyntetic penicillins, cefalosporins and aminoglicozids I-II generations), ineffective now, and the out-of-date preparations for local treatment of wounds (a hypertonic solution of chloride of sodium, ointment Vishnevskovo, ichtiol ointments, streptocid, tetraciklin, phurocillin, hentamicin ointments on a fatty basis). As a result the due antibacterial effect is not provided, and at local treatment of wounds also is not reached necessary anesthetizing, osmotic and antiedematic effects. As show numerous researches, the structure of originators of purulent complications of wounds (the significant share is necessary on anaerobs and fungi) has changed also.
Formation of stability of microorganisms to "old" preparations dictates necessity of introduction of new groups of medical products with a wide spectrum of activity (not only concerning aerobs, but also anaerobs) and their applications in strict conformity with a phase of wounds process.
The purposes of studying.
The student should be able :
To estimate complaints of the patient, revealing data for the complicated current wound process (strengthening be ill, occurrence of attributes of an inflammation, development of the general reaction of an organism in the form of a fever, rises in temperature of a body, etc.);
In detail to collect the anamnesis of disease, paying special attention On aetiological and the pathogenetic moments of formation of a wound, background conditions (stress, an alcoholic, medicamental, narcotic intoxication, violent actions, etc.);
To reveal in the anamnesis the diseases influencing on reparativ process and the immune status of the patient;
To estimate a way of life and working conditions, to establish their possible value in development of a pathology;
To make external survey and to interpret the received data (character of damage of tissues, the sizes of a wound, number of damages, their localization, presence of inflammatory changes, danger of development of a bleeding, a condition regional lymphatic noduls);
To estimate the general condition of the patient, a degree of an intoxication of an organism, character and volume of lesion (depth of a wound, the attitude the wound channel to cavities of a body, presence of damages of bones and internal organs, presence of inflammatory changes in depth of a wound);
To interpret results of bacteriological research (to detail a microbic landscape of a wound to estimate its microbic obsemenation, sensitivity of microflora antibiotics);
To estimate dynamics of current wound process;
To carry out a fence of a material from a wound for microbiological research;
Independently to tie up patients with purulent wounds, to make necrectomia;
To appoint antibacterial, immuncorrectial, dezintoxication treatment, physiotherapeutic methods of treatment.
The student should know:
Wound process is a complex of local and general reactions of the organism developing in reply to damage of tissues and introduction of an infection;
The so-called "critical" level is necessary for development of an infection in a wound bacteriemic obsemenation, corresponding concentration of microorganisms - 105-106 microbic bodies on 1 gram of a tissue (in the certain conditions the "critical" level can be and lower);
The surgical infection has features of clinical displays depending on the originator or associations of microorganisms in a wound that defines strictly an individual approach in treatment on a background of a recognition of uniform principles of treatment of purulent wounds;
The mephitic gangrene is the heaviest kind of a surgical infection;
Treatment of purulent wounds provides carrying out of the multidirected medical influence which is carried out according to a phase of wound process;
Principles of active surgical treatment of purulent wounds include a complex of the actions directed on the maximal reduction of terms of current of all phases of wound process with the purpose of its limiting approach not complicated current;
Microbiological researches of contents from a wound is obligatory and provides direct microscopy a material, bacterial inculatiuon and definition of sensitivity of microflora to antibiotics;
Results of microbiological research allow to corection spent treatment of a purulent wound;
Modern preparations for local treatment of wounds possess the combined medical action (antimicrobic, anesthetizing, osmotic, antiedematic, wound healing, necrolitic), and application wound coverings, owing to their structure, promote least traumatic and to painless carrying out of bandagings;
Any change of a bandage should occur in sterile conditions;
The doctor who is carrying out bandaging, should take special measures for own protection against an infection - from latex, protection gloves are necessary for eyes, and also a mask on a mouth and a nose;
Accurately imposed bandage, being visible end of processing of a wound, creates feeling at the patient, that it qualitatively treat and serve.
Basic knowledge.
1. Patophisiology of wound process.
Lectures on pathological physiology.
2. The Doctrine about an inflammation.
Lectures on pathological physiology.
3. Morphology of wound process.
Lectures on pathological anatomy.
4. Microbiology of wounds.
Lectures on microbiology.
5. Aseptics and antiseptics.
Lectures on the general surgery.
6. Kinds of healing of wounds.
Lectures on the general surgery.
6. Primary and secondary surgical treatments of wounds.
Lectures on the general surgery, traumatology.
7. Methods drenaging of wounds.
Lectures on the general surgery.
8. Bandaging.
Lectures on the general surgery.
9. The Surgical infection.
Lectures on the general surgery.
Questions for self-preparation:
On basic knowledge;
1. Attributes of an inflammation.
2. The Pathogenesis of wound process.
3. The Histogenesis of wound process.
4. The Microbiological characteristic of wounds.
5. Kinds of healing of wounds.
6. Primary and secondary surgical treatments of wounds.
7. Kinds of a surgical infection.
8. Methods drenaging of wounds.
9. Principles of imposing of bandages.
On a new theme:
1. Concept about a wound, classification of wounds.
2. Phases of current of wound process.
3. Characteristic of a purulent wound.
4. General principles of treatment of wounds.
5. Treatment of wounds depending on a stage of wound process.
6. Principles of active surgical treatment of purulent wounds.
7. Suturation on a purulent wound.
8. Rules of a fence of a material from a wound for microbiological research.
9. " Physical methods of influence " on wound process.
10. The Mephitic gangrene.
11. Practical carrying out of change of a bandage.
The maintenance of employment.
1. Wounds - mechanical damage of a tissue with infringement of their integrity.
Classification of wounds.
1. 1. By the form the wound agent
Bullet
Fragmental
From influence of a blast wave
From a secondary splinter
From a cold steel
From the casual reasons (trauma)
Surgical
2. On character of damage of tissues
Dot
Fragmentary
Crushed
Contused
Incised
Chopped
Chipped
Sawed
Bitten
Scalped
3. On extent and the attitude To cavities of a body
Blind
The Tangent
Through
Not Getting
Getting into a cavity
4. On number of damages At one wounded
Single
Plural
Combined
5. By the form damaged tissues- With damage:
Soft parts
Bones and joints
Nerves
Large arteries and veins
Internal organs
6. To an anatomic attribute
Heads
Necks
Breasts
The Stomach
The Basin
Extremities
7. On microbic obsemenation
Is bacteriemic-polluted
Aseptic
Fresh wounds till the moment of a full covering their granulations are capable to soak up toxins, bacteria, products of disintegration of tissues. The wounds covered by granulations, practically do not possess soaking up ability.
Theoretical researches show, that the major factor in development of an infection are the structure and a functional condition of tissues of a wound. Presence at a wound of the closed cavities, the alien bodies which have become lifeless, the tissues deprived blood supply promotes development of a wound fever. Development of pathogenic microflora in a wound and resorption products of disintegration of impractical tissues stimulations of blood cells and promote a connecting tissue, lead to allocation citokins and other mediators of an inflammation with a wide spectrum of biological action (system changes of a metabolism, immunity, a condition of a vascular wall, hemopoesis, functions of regulitary systems).
A.M. Svetukhin and J.L.Amiraslanov (2003) specify, that there are no qualitative distinctions during of wound process depending on aetiologycal factors. Proceeding from it, the concept of unity of a pathogenesis wound process irrespective of an origin, the sizes, localization and character of a wound is developed.
2. Phases of current wound process.
Current wound process can be divided into three basic phases:
I - a phase of an inflammation
The period of vascular changes;
The period of clarification from necrosis tissues;
II - a phase of neogenesis and development granulation tissues;
III - a phase of scar reorganization and cuticularizations.
3. The characteristic of a purulent wound.
It is proved, that for development of an infection in a wound presence of 105-106 microbic bodies on 1 gram of a tissue is necessary. It is a so-called "critical" level bacteriemic obsemenation. But the "critical" level can be and low. So, for development of an infection at presence of blood, alien bodies, ligature in a wound there are enough 104 (10000) microbic bodies; at setting ligature in a zone the ligatur ischemia of tissues - has enough 103 (1000) microbic bodies on 1 gram of a tissue. The combination of damage of tissues to a shock reduces threshold value of microbic number up to 103 (1000) in 1 г tissues, and with radiating lesions - up to 102 (100).
Wound ekssudat from a purulent wound it is rich with fiber, consists of cellular elements, basically - neutrophil leukocytes, a plenty of bacteria, the rests of the destroyed cells and a mix transsudat with fibrin.
A plenty of the microorganisms, the expressed degeneration neutrophil leukocytes, phagocytozis in pus specify presence of plasmocytes, decrease in quantity of one-nuclear leukocytes and absence adverse current of healing of a wound.
Development of inflammatory reaction depends on a degree of resistibility of tissues, reactance of an organism and virulently of infections.
According to recommendations the CART, all most often meeting bacteriemic patogens are divided on levels prerogative:
I. Patogens a high level prerogative:
A piogenic streptococcus;
A golden staphilococcus.
II. Patogens an average level prerogative:
Enterobacterias;
Pseudomonads and other not fermenting Gram-negative bacteria;
klostridias
bacteroids and others anaerobs;
Streptococcuses (other kinds).
III. Patogens a low level prerogative:
Bacillus anthracis;
Mycobacterium tuberculosis, Mulcerans, etc.;
Pasteurella multocida.
Originators of virus infections unlike fungi and bacteria very seldom are producers purulent ekssudat.
4. The general principles of treatment of wounds.
Surgical methods: a surgical treatment of a wound, disclosing congeries, necrectomia, performance decompression cuts, suturation, dermal plastic (the artificial skin, the split moved rag, a walking stalk on Filatov, autodermoplastic completlayer rag, free autodermoplastic slightlayer rag on Tirsh).
Local treatment of a wound with application of various kinds of drenaging, bandages and medicinal preparations.
Physiotherapeutic treatment: laser therapy, a magnetotherapy, UHV, UVI, the operated abacterial environment, etc.
The General treatment: antibacterial therapy; correction of infringements of functions of organs and systems, metabolic frustration; detoxication therapy; Increase of nonspecific resistency of an organism and immunocorrection therapy; stimulation reparativ processes.
5. The medical program depending on a stage wound process.
The phase of an inflammation (ekssudation) is characterized plentiful wound separated, expressed by peryfocal inflammatory reaction of soft parts and bacteriemic obsemenation the wounds, therefore applied medical preparations should possess high osmotic activity to provide intensive outflow ekssudat from depth of a wound in a bandage, should render antibacterial influence on contagiums, cause tearing away and fusion necrosis tissues. With this purpose antiseptic bandages (moist desiccation with chemical preparations and antiseptics, water-soluble ointments), during vascular changes - drenaging and hydrophil bandages (hypertonic, absorbing and adsorbing), during clarification from necros tissues - necrolitic means (proteplitic enzymes, hydrogel bandages) are applied; For stimulation of tearing away necrosis tissues - ointments on the water-soluble basis, possessing high osmotic activity (levomecol, levosin, dioxicol, etc.).
Considering the high cost price wound sorbtion coverings (hydrophil bandages), in a daily medical practice with success it is possible to use children's pampers or hygienic linings.
During clarification of a wound from necrosis tissues ointments for enzymatic clarifications of wounds which worthy representative is ointment «Irucsol», containing enzymes from Clostridium hystolyticum and broad-spectrum antibiotic «Chloramfenicol» (levomicetyn) are applied.
At presence perifocal dermatitis around of a wound it is expedient to impose zincoxid ointment (paste Lassara).
To all patients for 10-14 days recommend semi bed rest. The basic components of therapy are broad-spectrum antibiotics Ftorchinolon (maxaquin, tarivid, ciproby, cyfran, etc.) or Cefalosporin (dardum, duracef, cephzol, mandol, cefamezin, etc.) of some, entered parenteral (it is less preferable - peroral). Considering frequent associations of pathogenic microorganisms with bacteroid and fungoid flora, antibacterial therapy in some cases is expedient for strengthening, having included in it antifungoid preparations (diflucan, nizoral, orungal, etc.) and derivatives nitroimidazol (flagil, metronidozol, trichopol ,tinidazol, etc.).
The active inflammation and the expressed painful syndrome define expediency of system application of nonspecific antiinflammation means, such as dyclofenac (voltaren, ortophen), cetoprophen, oruvel, etc.
System and local hemoreological infringements follows correction by infusions antiagregants (reopolyglucin in a combination with pentoxiphillin).
Sensitization of an organism as a result of massive resorbtion structures with antigenic activity (fragments of fibers of microorganisms, products of degradation of soft parts, etc.), synthesis of a plenty of mediators of an inflammation (hystamin, serotonin, etc.) are absolute indications to carrying out desensitization therapies (Dimedrolum, suprastyn, diazolin, claritin, cetotyfen, etc.).
The basic preparations for treatment of wounds in 1-st phase wound process:
Ointments on a water-soluble basis: ( levomecol, levosin, dioxicol, dioxidin 5 % ointment, ointment of 10 % mafenid acetate, sulfamecol, furagel, ointment of 0,5 % chinifuril, iodopiron 1 % ointment, iodmetrixelen, streptonitol, nitacid, ointment miramistin 0,5 %, ointment lavendula, ointment lipacantin, methylurocil ointment with miramistin.
Sorbents and hydrogels: gelevin, celosorb, immosgent, carbonet, Multidex Gel, AcryDerm, Carrasin Hydrogel, Hydrosorb, Elasto-Gel, Purilon.
Enzymes: chimopsin, callagenasa the crab, caripasim, terrilitin (proteasa), protogentin (sipralin, lizoamidasa), enzim content dressing means (teralgim, immosgent), trypsin + urea, trypsin +chlorgecsidin, profezim, sipralin, lysosorb, collavin.
Solutions of antiseptic tanks: a solution iodopyroni, 02 % a solution furagini kalii, suliodopyroni, 15 % a solution dimefosfoni, 30 %-solution ПЭГ-400, 0,01 % solution miramistini.
Aerosols: nitazol, dioxizol, gentazol.
Wound bandages: «TenderVet», «Sorbalgon».
The phase of a reparation(neogenesis, formation and maturing granulation tissues) is characterized by clarification wound surfaces, occurrence of granulations, стиханием perifocal inflammations and reduction of ekssudation. The Primary goal of treatment becomes stimulation of growth and maturing of a connecting tissue alongside with suppression of microbes remaining in a small amount or their again appeared hospital shtamms. Such stimulators of neogenesis, as vinilin, vulnuzan, polymerol, and also antiseptic bandages with fat-soluble ointments and hydrophyl bandages (polyuretan and ot.) are widely applied.
System therapy correction, appointing antioxidants (aevit, tocopherol, etc.) and antihypoxants - deproteinic derivatives of blood cows (actovegin, solcoseril). For acceleration of growth of a connecting tissue it is expedient to appoint curiozin. It represents association hyaluronic acids and zinc. The hyaluronic acid increases activity phagocytozis in granulocyts, makes active phybroblasts and endoteliocyts, promotes their migration and prolipheration increases prolipherativ activity of cells of an epithelium, creating favorable conditions for remodelation connective tissue matrix. Zinc, possessing antimicrobic action, makes active a lot of the enzymes participating in neogenesis.
Very well itself have recommended biodegrading wound coverings (it is scarlet-levin, альгипор, альгимаф, гешиспон, свидерм, etc.).
The basic preparations for treatment of wounds in 2-nd phase wound process:
Ointments on an adjustable osmotic basis: methyldioxylin, sulfargin, fuzidini 2 % gel, lyncomicini 2 % ointment.
Polymeric coverings: combutec-2, digispon, algipor, algimaf, algicol, algico-АКF, kolahit, kolahit-F, sisorb, hydrosorb.
Hydrocolloids: galagran, galakton, hydrocoll.
Oils: meliacyl, oil of sea-buckthorn berries, oil of a dogrose.
Aerosols: dioxyplast, dioxyzol.
In a phase of the cuticularization, described the beginning of a cuticularization and maturing connective tissue of scar (scar formations and reorganization), among means of local influence optimum is application polymeric wound coverings which essentially accelerate process of a cuticularization, and also silicon semipermeable bandages.
Polymeric wound coverings can be subdivided conditionally (one bandage can be multi-purpose) on absorbing, protective, isolating, atraumatic and biodegrading. Sorbtion ability of coverings (the degree and speed of linkage ekssudat wounds) depends on the size of times of coverings.
6. Principles of active surgical treatment of purulent wounds (A.M.Svetukhin, J.L.Amiraslanov, 2003).
Wide section and disclosing of the purulent center. Already at this stage of treatment (the purulent surgery and traumatology) should contain elements of plastic surgery. At performance of cuts of tissues and a choice of access to the purulent center it is necessary to expect an opportunity of formation of the future blood suppling rags from the sites of a body next to a wound.
Excision all impractical and doubtful soft parts impregnated by pus within the limits of healthy tissues (in one or several stages). Removal of all osteal sequesters and necrosis bones shplins. Performance of a regional, trailer or segmentary resection of the amazed site of a bone also within the limits of healthy tissues.
Removal the immerse metal clamps which are not carrying out the applicability, and vascular prostheses.
Application of additional physical methods of processing of a wound.
Use during a surgical treatment of elements of plastic or reconstructive operations with the purpose of restoration or closing of the important anatomic formations.
The external osteosynthesis of long bones (under indications), provides an opportunity dynamic distraction-compressions manipulations.
7. Suturation on a purulent wound.
The primarily-delayed seam - apply in 5-6 days after a surgical treatment, before occurrence in a wound of granulations (is more exact within the first 5-6 days).
Early secondary seam - impose on the wound covered by granulations with mobile edges before development in it a cicatricial tissue. An early secondary seam impose within 2-nd week after a surgical treatment.
Late secondary seam - impose on granulating wound in which the cicatricial tissue has already developed. Closing of a wound probably in these cases only after preliminary cicatricial excision of tissue. Operation is made on 3-4 week after wound and later.
Indispensable condition for suturation on a purulent wound is maintenance of sufficient outflow wound separated, that is reached active drenaging, and the rational antibacterial therapy directed on destruction of a microflora which has remained in a wound.
8. Rules of a fence of a material from a wound for microbiological research.
After careful processing a surgery field the surgeon defines a place where pus accumulates, are located necrosis tissues, gas (crepitating is allocated or other attributes of an infection are observed. The particles of the amazed tissues intended for laboratory research, place in a sterile gauze and then in sterile capacity. Pus or another exudates should be accurately collected and placed in a sterile test tube. If it is possible, it is not necessary to use a wadded tampon. Exudates it is necessary to select a sterile syringe with a needle. If the wadded tampon is used, it is necessary to select as much as possible exuded and to place all tampon in capacity for sending in laboratory.
9. " physical methods of influence " on wound process.
1). The methods based on use of mechanical fluctuations:
Processing of a liquid by a pulsing jet,
Processing by low-frequency ultrasound.
2). The methods based on change of external pressure of the air environment:
Vacuum processing and vacuum therapy,
The operated abacterial environment,
Hyperbaric oxygenation.
3). The methods based on change of temperature:
•cryotherapy.
4). The methods based on use of an electric current:
Direct currents of a low pressure (an electrophoresis, an electrical stimulation),
The modulated currents (electrical stimulation).
5). The methods based on use of a magnetic field:
Low-frequency magnetotherapy,
Influence of a constant magnetic field.
6). Use of electromagnetic fluctuations of an optical range:
•laser radiation:
High-energy,
Low intensity,
•ultraviolet radiation.
7). The combined methods of influence.
Application of plasma streams. Influence of high-temperature streams of plasma on a wound surface allows to execute an adequate surgical treatment of a wound without blood and precisely. Advantage of a method besides is aseptic and a noninvasive section of tissues, that at a surgical infection has important value.
Ozonotherapy. Local ozonotherapy in the form of the ozonized solutions with concentration of ozone of 15 mkg/ml leads to decrease microbic obsemenation the purulent center, to increase of sensitivity of microflora to antibacterial preparations, stimulates reparaiv processes in a wound. System ozonotherapy renders antiinflammatory, detoxication, antihypoxy action and normalizes metabolic processes in an organism.
Use oxide nitrogen. Opening endogenous oxide nitrogen (NO) which is produced by cells by means of NO-syntez and carries out functions of a universal regulator-messenger, was large event of biology and medicine. In experiment the role endogenous NO in oxygenations of tissues and its deficiency in purulent wounds is established. Combination application of surgical treatment is purulent-necrosis lesions of soft parts and a complex of factors of physical influence (US, ozone and to NO-therapy) promotes acceleration of clarification of a wound from microflora and necros weights, to easing and disappearance of inflammatory displays and microcirculation infringements, activization to macrophageal reaction and prolypheration of fybroblasts, to growth a granulation tissue and a regional cuticularization.
10. A mephitic gangrene.
Anaerobs make overwhelming majority of normal microflora of the person. They live: in a mouth (in gingival pockets the flora on 99 % consists from anaerobs), in a stomach (at hypo-and anacids conditions the microbic landscape of a stomach comes nearer to intestinal), in a thin gut (anaerobs contain in smaller quantity, than aerobs), in a thick gut (the basic place of dwelling anaerobs). On etiology anaerobs are subdivided on clostridial (forming disputes), nonclostridial (not forming disputes), bacteroids, peptstreptoccocs, fuzobacterial.
One of the general symptoms of a mephitic gangrene is absence of microflora in crops at standard ways of their allocation (without application anaerostats). As microbiological identification anaerob microflora demands the special equipment and long time, great value methods get the express train-diagnostics, allowing to confirm the diagnosis within an hour:
- Microscopy of fixed smear, painted on Gram;
- Urgent biopsy the amazed tissues (are characteristic expressed focus of hypostasis tissues, necrosis basic layer focus of epidermis, hypodermic cellulitis, fascias, miolysis and destruction muscular fibres, perivascular hemorrhages, etc.)
- gas-liquid chromatography (flying fat acids-acetic, oil, isooil, kapron are defined, phenol and its derivatives produced on Wednesday of growth or in pathologically changed tissues anaerobs during a metabolism).
According to gas-liquid chromatographies and weights-spectrometry it is possible to identify not only asporogenic anaerobs, but also clostridial microflora (originators of a gas gangrene), for which presence 10-oxyacid is characteristic.
Without dependence from localization of the center anaerob process has a number of the general and characteristic attributes:
The Unpleasant putrefactive smell ekssudat.
Putrefactive character of lesion.
Dirty poor ekssudat.
Gas-plant (bubbles gas from a wound, crepiting hypodermic , gas above a level of pus in a cavity of an abscess).
Affinity of a wound to places of natural dwelling anaerobs.
From the anaerob processes which are taking place in surgical clinic, it is necessary to note the special form - epifascialis creeping phlegmon of a forward abdominal wall which develops as complication after operations (more often after appendectomia at gangren-perphorativ appendicites).
Anaerob clostridial infection - the acut infectious disease caused by penetration into a wound and duplication in it forming disputes anaerobs of a sort clostridis (Clostridium perfringens, Clostridium oedematiens, Clostridium septicum, Clostridium hystolyticum). Disease develops in the first 3 days after wound, less often - later some hours or week is more often, is observed at gunshot wounds, in surgical branches - after ablation of the bottom extremities in occasion of an atherosclerotic gangrene and even after appendectomia, etc. the Probability of occurrence of a mephitic gangrene acutly raises at presence in wounds of alien bodies, crises of bones and the damaged large arteries as in such wounds it is a lot of ischemic, necrosis tissues, deep, badly aerated pockets.
Anaerobs clostridium allocate a number of the strongest eczotoxins (neuro-, necro-, enterotoxins, hemolyzin) and enzymes (gialuronidase, neuraminidase, fibrinolisine, a collagenase and elastase, lecytinase, etc.) which cause a hypostasis of tissues, acut permeability of vessels and hemolyzis, necrosis and fusion of tissues, a heavy intoxication of an organism with damage of internal organs.
Patients first of all feel holding apart pain in a wound, the hypostasis of tissues around of it quickly accrues. On a skin there are the centers of cyanotic painting extending quite often on significant distance from a wound in a proximal direction, and the bubbles filled muddy by hemorragial contents. Palpation at tissues around of a wound it is defined crepitation.
Simultaneously with local displays deep general frustration are marked: weakness, depression (less often - excitation and euphoria), rise in temperature of a body up to the febril figures, acutly expressed tachycardia and increase of breath, pallor or yellowness of the skin, a progressing anemia and an intoxication, at lesion of a liver - yellowness of sclers.
At roentgenography of the amazed extremity gas in tissues is found out. Diagnostics of a mephitic gangrene is based basically on clinical data. Medical tactics is under construction also in a clinical picture of disease.
At a mephitic gangrene prevail necros changes in tissues and practically are absent inflammatory and prolypheration.
Anaerob nonclostridial infection (a putrefactive infection) is caused anaerobs, not forming dispute: B. coli, B. putrificus, Proteus, bacteroides (Bacteroides fragilis, Bacteroides melanogenicus), Fusobacterium, etc., it is frequent in a combination with staphilococcuses and streptococcuses.
On local changes of tissues and the general reaction of an organism the putrefactive infection is close to anaerob clostridial infection. Prevalence processes of necrosis above processes of an inflammation is characteristic.
Clinically local process in soft parts usually proceeds in the form of nonclostridial phlegmons, destroying hypodermic fatty cellulitis, fasces (fasciitis), muscles (miozitis).
The general condition of the patient is accompanied expressed toxemia, quickly leads to a is bacteriemic-toxic shock with a frequent lethal outcome.
The putrefactive infection is more often observed at heavy infected lacerate-contusion wounds or at the open crises with extensive destruction of soft parts and pollution of a wound.
The surgical intervention at anaerob clostridial and nonclostridial infections consists in a wide section and full excision become lifeless tissues, first of all muscles. A wound after processing plentifully wash out solutions of oxidizers (peroxide of hydrogen, a solution KMnO4, the ozonized solutions, hypochlorir sodium), make additional «lampas» cuts in a zone of pathological changes outside a wound, « lampas » cuts overstep the bounds of edge of the center of an inflammation, in addition excision of necroses, a wound do not sew up and not tamponade, provide in subsequent their aeration. After operation use hyperbaric oxygenation.
Antibioticotherapia of mephitic gangrenes.
For empirical application at mephitic gangrenes it is recommended clyndomycin (delacil). But considering, that the majority of such infections mixed, therapy is usually spent by several preparations, for example: clyndomycin with aminoglycozids. Many stamms of aerobs suppresses riphampin, lyncomycin. On Gram-positive and Gram-negative anaerob coccuses well operates benzilpeniccils. However to it quite often there is an intolerance. Its substitute is erythromycin, but it badly acts Bacteroides fragilis and fuzobacterias. Concerning anaerob coccuses and sticks the antibiotic fortum (it is combined with minoglycozids), cefobid (cefalosporins) is effective.
The special place among the preparations applied to influence on anaerobic microflora, borrows metronidazole - metabolic poison for many strict anaerobs. On Gram-positive forms of bacteria metronidazole operates much more poorly, than on Gram-negative, therefore its application in these cases is not justified. Relatives on action to metronidazole have appeared others imidazols - niridazol (more actively metronidazole), ornidazol, tynidazol.
Solution dioxydin (up to 120 ml in/in 1 % is applied to adults) also, and also carbenicillin (12-16 g/day in the adult).
11. Practical carrying out of change of a bandage.
Any change of a bandage should occur in sterile conditions. Always it is necessary to use so-called « non-touch technique » (a contactless technique). To a wound or a bandage it is not supposed touches without gloves. The doctor doing bandaging, should take special measures for own protection against an infection: from latex, protection gloves are necessary for eyes, and also a mask on a mouth and a nose. The patient it is necessary to arrange conveniently, and the area of a wound should be well accessible. The good source of illumination is necessary.
If the bandage is not removed, it cannot be torn off. A bandage moisten with aseptic solution (peroxide of hydrogen, solution Ringer) while it will not come unstuck.
At the infected wounds the area of a wound is cleared in a direction outside inside, disinfectants are if necessary used. Necroses in a wound it is possible to remove mechanical by by means of a scalpel, scissors or curette (the preference should be given a scalpel, removal by scissors or curette entails risk compression of tissues and repeated trauma).
Are effective enough for clearing a wound of washing aseptic solution from a syringe at easy pressure of the piston. At deep wounds washing is spent by means of bulbous-end, grooved probe or through short cateter. The liquid should be collected by means of a napkin in a tray.
Granulation tissue sensitively reacts to external influences and damaging factors. Granulation tissue constant maintenance of a wound in a damp condition and protection from trauma in the best way promotes formation at change of bandages. Excessive granulations usually leaves by means of a cauterizing pencil.
If edges of a wound show propensity to a cuticularization and kinking inside carrying out of a surgical treatment of edges of a wound is shown.
Well developing epithelium does not demand other leaving except for maintenance in a damp condition and protection from trauma change of bandages.
The surgeon should provide, that chosen the wound bandage optimum approached to a surface of a wound - wound secret can be absorbed only under condition of good contact between a bandage and a wound. Unreliably fixed bandages at movement can cause irritation of a wound and slow down its healing.
The scheme of inspection of the patient.
At revealing complaints at the patient to reveal data of the complicated current wound process (attributes of an inflammation, rise in temperature of a body, etc.).
The anamnesis of disease to collect in detail, paying special attention On etiological and the pathogenetic moments of formation of a wound, background conditions (stress, an alcoholic, medicamental, narcotic intoxication, violent actions, etc.).
In the remote anamnesis to reveal the transferred diseases or the available sufferings influencing on reparativ process and the immune status, to establish possible value in development of a pathology of a way of life and working conditions of the patient.
To make external survey and to interpret the received data (character of damage of tissues, the sizes of a wound, number of damages, their localization, presence of inflammatory changes, danger of development of a bleeding, a condition regionar lymphatic nodules).
To estimate the general condition of the patient, a degree of an intoxication of an organism, to specify character and volume of lesion (depth of a wound, the attitude wound channel to cavities of a body, presence of damages of bones and internal organs, presence of inflammatory changes in depth of a wound).
To carry out a fence of a material from a wound for microbiological research or to interpret already available results (a microbic landscape of a wound, a degree microbic obsemenation, sensitivity of microflora antibiotics).
To tie up the patient, if necessary to make necrectomia, washing of a wound, drenaging, physiotherapeutic treatment.
At repeated bandaging to estimate dynamics of current wound process.
To appoint antibacterial, immunocorrectial, dezintoxication treatment, physiotherapeutic methods of treatment.
TESTS
1. Primary closure of incised wounds must be done within ...........
a) 2hrs
b) 4hrs
c) 6hrs
d) 12hrs
e) 16hrs
2. The tensile strength of wound reaches that of normal tissue by-
a) 6 weeks
b) 2 months
c) 4 months
d) 6 months
3. The worst position for scars is
a) Back
b) Shoulder
c) Sternum
d) Abdomen
4. The best scars are seen in
a) Infants
b) Children
c) Adults
d) Very old people
5. Patient has lacerated untidy wound of the leg and attended the casualty after 2 hours. His wound should be -
a) Sutured immediately
b) Debrided and sutured immediately
c) Debrided and sutured secondarily
d) Cleaned and dressed
6. Lacerated wound looks like an incised wound in the
a) Scrotum
b) Scalp
c) Abdomen
d) Thigh
7. Following are required for wound healing
a) Zinc
b) Copper
c) Vitamin C
d) Calcium
8. Wound healing is worst at -
a) Sternum
b) Anterior neck
c) Eyelid
d) Lips
9. When is the maximum collagen content of wound tissue -
a) Between 3rd to 5th day
b) Between 6th to 17th day
c) Between 17th to 21st day
d) None of the above
10. If rupture marks are to be avoided, skin sutures should be removed by -
a) 72 hours
b) 1 week
c) 2 weeks
d) 3 weeks
11. What is true about keloids -
a) It appears immediately after surgery
b) It appears a few days after surgery
c) It is limited in its distribution
d) It is common in old people
12. Keloid is best treated by -
a) Intrakeloidal injection of triamcinolone
b) Wide excision and grafting
c) Wide excision and suturing
d) Deep X-ray therapy
13. A patient with grossly contaminated wound presents 12 hours after an accident. His wound should be managed by -
a) Thorough cleaning and primary repair
b) Thorough cleaning with debridement of all dead and devitalised tissue without primary closure
c) Primary closure over a drain
d) Covering the defect with split skin graft after cleaning
14. Delayed wound healing is seen in all except -
a) Malignancy
b) Hypertension
c) Diabetes
d) Infection
15. Keloid scars is made up of -
a) Dense collagen
b) Loose fibrous tissue
c) Granulamatous tissue
d) Loose areolar tissue
16. Highest concentration of hydroxy proline is seen in -
a) Elastin
b) Collagen
c) Fibrous tissue
d) Gelatin
17. The following statement about keloid is true -
a) They do not extend into normal skin
b) Local recurrence is common after excision
c) They often undergo malignant change
d) They are more common in whites than in blacks
18. Fibroblast in healing wound derived from -
a) Local mesenchyme
b) Epithelium
c) Endothelial
d) Vascular fibrosis
19. In the healing of a clean wound the maximum immediate strength of the wound is reached by -
a) 2 - 3 days
b) 4-7 days
c) 10- 12
d) 13- 18 days
20. The normal tensile strength of tissue at the site of wound is gained after --
a) One week of wound healing
b) Two weeks of wound healing
c) Two months of wound healing
d) Two years of wound healing
21. Management of an open wound seen 12 hrs. after the injury-
a) Suturing
b) Debridement and suture
c) Secondary suturing
d) Heal by granulation
22. Degloving injury is -
a) Surgeon made wound
b) Lacerated wound
c) Blunt injury
d) Avulsion injury
e) Abrasive wound
23. The best cure rate in keloids is achieved by -
a) Superficial X - ray therapy
b) Intralesional injection of triamcinolone
c) Shaving
d) Excision and radiotherapy
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
SURGICAL DISEASES AND DIABETES. PROBLEMS OF THE INFECTION IN DIABETES (IN DIABETIC PATIENTS). THE DIABETIC FOOT
Составитель асс. О.Г.Шахбазян
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
The purpose of employment.
Mastering by students of special knowledge and purchase of practical skills on diagnostics and treatment of such complication of diabetes mellitis (SD), as « a syndrome of diabetic foot » (DF), leading development ulcer-necrosis and infectious process, and in the further - a gangrene of foot.
The student should know:
Urgency of a studied problem and patophiziologi mecanizms developments micro-and macroangiopathy at DF.
Role not fermental autooxidation glycolysis and oxidizing stress in development of aggregation trombocitis, increase of permeability of a vascular wall, decrease antiagregations functions of an endothelium and induce is permanent existing trombodangerous.
The classification of syndrome DF accepted on 1-st International symposium on diabetic foot (the Netherlands, 1991), and recommended by domestic experts.
Degrees of ischemic damages of the bottom extremities according to the classification offered W. Wagner in 1979.
Features of purulently-necrosis process at diabetic foot.
Clinical and special methods of research in diagnostics of syndrome DF.
Methods of conservative treatment diabetic angiopathy.
Choice of medicamental preparations and their combinations depending on a stage of an ischemia, weight of trophic infringements, the mechanism of action of a preparation, a kind and weight of an accompanying pathology.
Role prostoglandin and its derivatives (vasoprestan, etc.), preparations glicozaminoglicans (sulphodexid, etc.) and enzim therapy (vobenzim, flogenzim) in correction of infringements of a blood flow and treatment of purulent complications.
Feature of a surgical treatment of the purulent center and ablations at diabetic foot.
The student should be able:
To diagnose various clinical forms DF.
To estimate a degree of lesion by purulently-necrosis process of feet.
To interpret on doppler-and angiograms of infringement of an arterial circulation of the bottom extremities.
To define a pulsation of arteries on a femoralis, a poplitea and vessels of foot.
To estimate on roentgenograms attributes osteopathy and deformations of foot.
To tie up patients with purulent-necrosis processes of foot and after ablations.
To prepare for a set of surgical toolkit for a resection of a segment of foot and ablations of an extremity at a level of a hip and a shin.
The maintenance of studied disease.
Urgency of a problem
Diabetes mellitis (SD) now is the widespread disease. In economically developed countries meets at 2-6 % of adult population. According to the CART (1999г.), now diabetes mellitis 120 million person suffers. In Russia the number of patients with SD comes nearer to 8 million person.
Patients with SD in 2-3 times have ischemic heart disease, a blindness - in 10, and a gangrene of the bottom extremities - in 20 times more often, than at persons without SD is more often. Lethality at patients of elderly and senile age at purulent-necrosis complications and a gangrene of extremities at SD reaches 20 %. For development of the uniform approach to diagnostics and treatment of patients with SD characteristic for a diabetes neuropathy, angiopathy and osteopathy in 1987г. Under the decision of research group the CART has been offered the term « diabetic foot » and it is recommended to consider it as a potential infectious problem.
Pathogenesis diabetic angiopathy
«Diabetic angiopathy» - the term entered H. Burger in 1954г., includes various on character morphofunctionals multiorgan lesions of vessels at patients SD. Thus lesion arteriols, venuls and capillaries H. Burger has named diabetic microangiopathy . While atherosclerotic lesion of average and large vessels carry to diabetic microangiopathy.
In norm there are two ways of oxidation of glucose:
the glycolitic way of oxidation to cycle of Crebs demands presence of enough of insulin;
At deficiency of insulin joins a sorbitology way.
At surplus of glucose in blood and insufficiency of insulin in tissues and vessels collects sorbitol and fructose which lead angiopathy by infringement of osmotic balance in walls of capillaries and to a thickening basic membranes.
Development diabetic angiopathy influences not only duration of disease SD, but also its weight. The basic changes thus occur in to a basic membrane of capillaries in which collect mucopolisacarids, fructose, sorbitol, glucoproteids, lipids, various albuminous substances. A basic membrane thickening in 2-5, and sometimes at 8-10 time.
Besides at microangiopathis occurs prolipheration and a thickening of cytoplasm of cells of an endothelium arteriols and fine arteries, that appreciably complicates transcapillar exchange. The thickening of basic membranes of capillaries and an endothelium breaks a selective filtration of biological liquids and exchange diffusion that interferes with removal of products of an exchange, maintenance of tissues with nutrients and oxygen. The thickening basic membrane also complicates migration of leukocytes and phagocytes in paravasalis space, reducing resistibility of tissues to an infection. Infringement of vascular permeability and change of microcirculation in turn promotes an output of plasma in soft parts, than presence at patients with diabetic angiopathy a subfascial hypostasis speaks. All these circumstances promote occurrence of various degrees of an ischemia and a diabetic gangrene.
For diabetic lesions of arteries it is characteristic segmentary and circular mediocalcinosis (arteriosclerosis of Menkeberg). As a result calcification vascular wall becomes rigids, loses ability to reduction and dilitation, that sharply reduces adaptable opportunities of vascular system of extremities, and lesion of fine intramuscular arteries interferes with development collateral circulations.
A number of authors consider, that microangiopathy is not complication, and enters into clinical syndrome SD. Thus some authors consider as the basic or initial form of display of disease neuropathy which in turn leads to development microangiopathy. At the same time W. Kane (1990г.) considers, that neuropathy at a diabetes is consequence of an ischemia of a nerve, т. е. Result of lesion vasa nervorum. In its opinion, lesion of fine vessels (capillaries, vasa vasorum, vasa nervorum) is characteristic and patognomatic for a diabetes. Lesion of independent nerves in turn leads to infringement of function of vessels. Degenerate changes in peripheral nerves owing to what there can come full loss of painful sensitivity stop and a shin in parallel develop.
Classification
The most widespread classification diabetic microangiopathy is classification W. Wagner (1979) on which distinguish 6 degrees of ischemic lesion of the bottom extremities:
Degree 0 - without visual changes of integuments;
Degree 1 - the superficial ulcerations which are not extending on all derms, without attributes of an inflammation;
Degree 2 - deeper ulcerations grasping adjoining sinews or an osteal tissue;
The degree 3 – ulcer and necrosis process, is accompanied by connection of an infection with development of a hypostasis, hypertherms, occurrence of abscesses, phlegmons, contact osteomyelitis;
Degree 4 - a gangrene of one finger and more or a gangrene distal department of foot;
Degree 5 - a gangrene of a greater part of foot or all foot.
For the characteristic diabetic microangiopathy the majority of surgeons classification of Fonten-Pokrovsky adhere.
Methods of diagnostics
Methods of inspection of patients with diabetic angiopathy can be divided into following groups:
Clinical;
Special;
-Reflecting macro-and microcirculation of an extremity;
-Studying a condition of various parts of a homeostasis: a metabolism, endotoxigions, immunoreactions, a hemostasis, central hemodinamic, etc.
Clinical methods
Clinical methods of diagnostics are of great importance at specification of the diagnosis diabetic angiopathy.
So, well collected and correctly estimated anamnesis enables not only correctly to formulate the primary diagnosis, but also to define character of current of disease.
Frequency of exacerbations and remissions allows to make a full picture of disease as a whole, to predict its current and consequently and to plan subsequent tactics of treatment.
At survey of the patient the doctor should pay attention to the following moments:
Condition of a skin (thickness, color, presence of ulcers, scars, attritions, corns);
Deformation of fingers and feet;
Hypostasis;
Condition of nails (hyperceratousis);
Pulsation of arteries;
Capillary blood flow;
Blood supply veins;
Scalp;
Muscle tone;
Sensitivity;
Presence be ill in rest and at walking;
Dermal temperature.
Thus both extremities should be surveyed in the comparative plan.
Special methods of research
At presence diabetic angioneuropathy patients should be directed on more profound clinical and tool inspection including:
Research of vibrating sensitivity a tuning fork or biotenzimetr.
Research of tactile temperature sensitivity.
Estimation of a dermal blood flow - laser research of a dermal blood flow,
a capillaroscopy, polarygraphy, transcutaneus definition of a pressure of oxygen.
Ultrasonic dopplerographia with definition of ankle-humeral index and linear speed of a blood flow.
Duplex scanning of arteries.
Rentgenography of bones of foot for osteopatology and deformations.
Angiographia.
Features of purulently-necrosis process
At diabetic foot
Acute decrease the in the general both local immunoactivity and resistibility to an infection because of reduction of transport O2, leukocytes and phagocytes and paravasalis space through thickening basic membrane.
Because of presence diabetic neuropathy and decrease in a threshold of painful sensitivity a trauma of patients do not pay to infectious process of attention that promotes fast distribution of purulently-necrosis process.
Purulently- necrosis process usually begins in the field of heads deformed metatarsus bones with frequent development of osteomyelitis and pathological crises.
The damp component of an inflammation because of interstitial hypostasis as a result of a thrombosis of lymphatic and venous vessels and infringement of an adequate drainage of tissues (microlimphatic and venous trombosis) prevails.
Propensity to fast generalization of purulent process on tendinous and to interfascial spaces at a constant skin.
Mediocalcinosis of Menkenberg and hyalinosis of arteries leads them rigidity, to decrease in an extensibility and reduction collateral overflow and decompensation blood supplies of tissues.
Expressed endotoxigy with fast development of multiorgan insufficiency.
Frequent development of a sepsis.
Fast decompensation SD with development of a metabolic acidosis, ketosis, and their difficult correction without liquidation the centers of necrosis.
Heavy infringement of an albuminous, fatty and electrolytic exchange.
Prevalence anaerobic and the mixed flora in the center of an inflammation.
Presence of hypercoagulation and the raised aggregation and adhesion of uniform elements of blood.
Fast approach of an anemia and hypoproteinemia.
Principles of treatment it is purulent-necrosis complications of diabetic foot
Urgent hospitalization in angiological department or department « diabetic foot ».
Insulin therapy (insulin before full healing wounds and ulcers).
Surgical treatment - wide necrectomia within the limits of healthy tissues.
Antibioticotherapia (it is better long intraarterial continuous) in view of sensitivity dosages, nefropatology.
At indications extracorporalis detoxication (hemosorbtion, a plasmapheresis, enterosorbtion).
Introduction of the preparations improving microcirculation (anticoagulants, antiagregants, antioxidants).
Immunostimulation (Т-activin, licopid, leycinpheron, an antibody, pentoglobin, immunal, etc.).
Sindromic therapy (correction AAS (acid alkaline status); the broken functions of organs and systems; a metabolism).
Local treatment.
After decrease inflammatory process it is necessary to solve the problem improvements of a circulation in stop and shins.
(Items 2, 3, 4, 5, should be realized after hospitalization in parallel with inspection of the patient).
Treatment purulently-necrosis complications at diabetic macroangiopathy can be divided into three stages.
1-st stage:
Liquidation of an acuteness of purulently-necrosis process:
Opening and drenaging phlegmons;
Wide necrectomia;
Translation of a damp gangrene in dry;
Achievement of a precise demarcation shaft.
Struggle with endotoxigions.
Normalization of carbohydrate, albuminous, fatty and HYDRO-ELECTROLYTIC exchanges.
Restoration of the immune status.
Improvement of microcirculation.
2-nd stage: restoration or improvement of a circulation.
3-rd stage: closing of defect of tissues after necrectomia and restoration of functions of an extremity.
Conservative treatment diabetic macroangiopathy
Long-term supervision show, that the basis of treatment of diseases of vessels is made with complex therapy which should be rational and individual.
We emphasize a word "rational" as, unfortunately, in most cases in out-patient departments reception and treatment of this category of patients are carried out by surgeons of the general structure, thus the opportunity of casual selection of medical products as the market is more and more sated various is great, including effective enough and is very frequent inefficient preparations. Treatment should be directed on removal of a spasm and a pain, improvement collateralis circulations, microcirculation, reological properties of blood with the purpose of translation of disease from a heavy stage to easier. Prophylaxis of the further developments (stabilization) overcooling, nervous stresses, infringement of a diet spend by influence on the general condition of the patient, its activation protective and compensatory mechanisms with obligatory elimination of such factors, as smoking.
Diet and mode
At treatment of a diabetes basic value equally important four moments - a feed, physical activity have, medicines and self-checking. Its health depends on a level of consciousness of patient SD. Very important that each patient competently concerned to the illness and observed a special diet, works, rest, etc.
Medicamental therapy
The choice of this or that preparation and their combinations depends on a stage of an ischemia, weight of trophic infringements, the mechanism of action of a preparation, compatibility, changes in a homeostasis, a kind and weight of an accompanying pathology, etc. is the Most frequent at treatment diabetic micro-and macroangiopathy use following groups of the preparations united on the mechanism of action:
Spasmolitics (papaverini, drotoverina hydrochloride, tolperison).
The preparations, improving fabric a metabolism (solcoseril, actovegin).
Hypolipidemic preparations.
Angioprotectors (pentoxiphillini, hynko biloba, alprotastil, vazoprostan).
Dezagregants (Acidum acetylsalicylicum, thyclopediny, sulodexid).
Reological preparations (reopoliglyukin).
Antioxidants (vitamin E, Acidum ascorbinicum, mexidol).
Immunostimulators (immunophan, polioxidony, Т-activin).
Anticoagulants (phraxipariny, enoxapariny, varpharin, etc.).
The preparations improving venous and lymphatic outflow (calcium debosilat, escusan, troxerutin, diosminy).
Alongside with medicinal therapy at not complicated diabetic angiopathy appoint following actions.
Physiotherapy
As indications to purpose of physiotherapeutic procedures at diabetic macroangiopathy initial stages of disease serve in a phase decrease inflammatory process and a stage of remission of pathological process.
Pulse currents, magnetotherapy, laser therapy, diadinamic currents which appoint to lumbar area and on a course of a neurovascular bunch on a hip and a shin are most effective.
Sanatorium treatment
At initial stages of disease, when there is no trophic infringements and exacerbations, alongside with a physiotherapy sanatorium treatment is recommended.
Sanatorium treatment has double medical effect - owing to change of a habitual mode, a climate, a conditions of life and as a result applications of balneological procedures.
From balneological procedures are most effective rodonic, hydrosulphuric, narzans, iodbromic baths.
The resorts located in an average strip of Russia and on Caucasus (Pyatigorsk, Mineral Waters, Kislovodsk, etc.) are recommended.
Local treatment
At purulently-necrosis processes the actions directed on improvement of the general condition of the patient, restriction of necrosis, improvement of a circulation, removal of the become lifeless tissues, prophylaxis and treatment of an ascending infection are spent. At a damp gangrene with the purpose of its translation in dry appoint antibiotics, diuretics, UFО. Necrosis fingers close the gauze napkin impregnated of 3-5 % by iod tincture, 5-10 % a solution manganous K, camphor spirit, xeroforms, tincture of a calendula, 70 % spirit a solution.
At quickly progressing damp gangrene with its transition to a back surface of foot or a shin, especially at the expressed intoxication, it is necessary to execute ablations at a level of a hip or the top third of shin for rescue of a life of the patient.
At patients with a dry gangrene the basic actions are directed on mummification of tissues, thus application of damp bandages and ointments is inadmissible. To the amazed site access of air should be provided. Some times in day the area of necrosis is processed 70 % spirit by a solution, 3-5% iod tincture, tincture of diamond greens, tincture of a calendula. Fast mummification and demarcation comes at processing a place of necrosis 5-10 % a solution KMnO4 At favorable current it is necessary to aspire to independent tearing away mummificatioms site or spend bloodless necrectomia on a line of demarcation.
At necroses and ulcers before clarification purulently-necroses tissues spend bandagings 1-2 times to day with use of a fabric sorbent "MISS-TH", etc. After removal necroses tissues of a wound wash out 3 % a solution of peroxide of hydrogen, solutions phuracillini, hypoclorit sodium, and impose bandages with proteolitics enzymes (tripsyn, chymotripsyn, rhybonucleaza, dezoxyrhybonucleaza , etc.) with water-soluble ointment, curiozins, etc.
Application for bandagings sorbents and various napkins with immobilizing enzymes, antiseptics and biostimulators allows to reach following results:
To lead dehydrotation tissues in a zone of purulently-necroses process at the first stage of wounds process
To create local high concentration antiseptics.
To reach atravmatic bandagings.
To reduce time of bandaging and to facilitate work of medical staff.
To exclude a hotbed effect under a napkin as a result of good air permeability.
To accelerate terms of treatment and transition in a phase dehydrotation.
During bandagings at good blood supply it is recommended to irradiate a wound erythema doses of ultra-violet beams. At occurrence of granulations for acceleration of clarification of bandaging spend with iruxol ointment, juice calanhoe, solkoseril jelly, ektericids, ointment of a calendula, vulnuzan, 40 % ointment of Acidum salicylicum, ointment levomecol, etc. After clarification of a wound (ulcer) and at good granulations of bandaging spend in day with use of 10 % methyluracil ointments, sperm ointment, solkoseril ointments, vinilin, ointment with heparin (hepatrombin, etc.).
The success of treatment of trophic infringements can be reached only under condition of improvement of a circulation in an extremity.
Prophylaxis of complications of diabetic foot
Indemnification SD - the first necessary condition of prevention of lesion of the bottom extremities.
For the most effective treatment of lesions of foot early revealing the patients having raised risk of development of a syndrome of diabetic foot is necessary. The risk raises with the years and duration of illness.
The patients having especially high risk, should be examined by the expert for acceptance of urgent measures.
Adequate training of patients considerably reduces frequency of ablations of the bottom extremities.
Survey of legs of patient SD with the purpose of revealing of a mycosis is necessary for spending dermatology not less often than 1 time to a year.
As at far come stages of disease diabetic polyneuropathy is irreversible without special prophylaxis it is necessary to collide with relapse of a syndrome of the neuropathy-infected foot. Basically this prophylaxis consists in an explanation of patients, in what consequences results infringement of painful and temperature sensitivity. Patients should examine daily the legs, paying attention on damage of integrity of a skin and attributes of an inflammation (reddening, hyperemia, puffiness). Nails on legs should be shortened so that they could not grow (to not cut, and accurately to file a file). Callouses need to be processed cautiously pumice. Even the smallest scratchs need to be processed antiseptics. At presence of intermanual mycosises it is necessary to spend antymycos treatment.
The ILLUSTRATIONS:
Tables and figures, slides, videofilms, angiograms, dopplerograms.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
SURGICAL SEPSIS. SEPTIC MANIFESTATION (MULTIPLE ORGAN DISFUNCTION SYNDROME – MODS). SYSTEMIC INFLAMMATORY RESPONSE SYNDROME (SIRS)
Составитель асс. О.Г.Шахбазян
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
The student should be able:
To estimate complaints of the patient, bringing to a focus to a fever, a fever, dryness in a mouth, the general weakness, infringement of a dream, a short wind, vomiting;
In the anamnesis of disease special attention to turn on presence of the purulent center and zones of aggressive manipulations (a purulent wound; bacteriemic lesion of internal organs, bones, joints; a puncture and catheterizations of vessels; quinsy; purulent diseases of integuments and hypoderms; a thrombophlebitis);
In the anamnesis of a life to reveal the burdening factors promoting development of a sepsis: treatment of immunosuppressive preparations, diseases of blood, diabetes mellitis, a cirrhosis of a liver, collagenose, a radial illness, a HIV - an infection, is purulent-infectious lesions of urinogenital ways, a gastrointestinal tract, bilious channels, respiratory ways;
At survey to pay attention to a condition of integuments and mucous: petexis, attributes of exicosis, pallor, cyanosis, hot or cold;
At physical research to estimate a condition of primary purulent process: color and viability of granulations, character and quantity purulent separated, presence purulent not drenaging centers, presence regional lymphangitis, lymphadenitis and thrombophlebitis. At localization of purulent process in a belly cavity to reveal symptoms of functional infringement of a gastrointestinal tract and a peritonitis: meteorism, oppression or absence peristaltic, a pressure of muscles of an abdominal wall, positive symptom Shetkin-Blumberg;
To mark infringements of a mental condition (from anxiety up to delirium and coma), cardiovascular system (a tachycardia, a hypotonia, hipoxigen changes of an electrocardiogram, increase CVP; infringements of microcirculation); to reveal pulmonary complications (a pneumonia, a pleurisy, attributes of a "shock" lung, sharp respiratory « distress syndrome »); lesion of a liver (yellow sclera’s and integuments, increase in an organ), kidneys (oligury, change of color of urine), spleens (increase);
Correctly to interpret data of a laboratory blood analysis, bringing to a focus on leucocytes and shift leukocyte formulas to the left, electrolytic balance, a condition of an oxygen mode and AAC blood, a level of bilirubin, fiber, a fibrinogen, sugar, urea, creations, to estimate of enzimemia (LDG, ALT, nuclear heating plant, alkaline phosphatesis), parameters of a coagulogram (attributes of development of the DIC-SYNDROME), daily allowances quantity of urine and changes in urine (proteinuria, microhemouria);
To estimate data of tool diagnostics:
Roentgenographies of a belly cavity and thorax, radiopaque methods of research;
Ultrasonic scanning and computer tomography of the pathological center;
Endoscopic methods (a laparoscopy, FEGDS);
To spend differential diagnostics: with purulent-resorb fever, a heart attack of a myocardium, aseptic pancreonecrosis, a thromboembolism of a pulmonary artery, a thrombosis mesenteric vessels, a poisoning, diabetic coma;
To carry out bandagings, to open the purulent centers, to make laparocentes, punctures of a pleural cavity and joints at their purulent lesions, to spend active drenaging a purulent cavities.
Summary of the maintenance of employment.
The urgency of a problem of a sepsis and toxic-septic shock is caused by that for last 50 years lethality at this heavy pathology has decreased only on 20 %, and to the beginning of XXI century on the average makes about 40 %. Specification of concept of "sepsis", as syndrome of the system inflammatory answer arising in conditions of massive receipt of an infection and their toxins from the purulent center in a blood flow and leading development of infectious multiorgan insufficiency. Clinical attributes of system inflammatory reaction are simple. They include: a body temperature more 380С or less 360С, a tachycardia more than 90 impacts in a minute, tachypnoe more than 20 in a minute or Pa СО2 less 32 mm Hg, leukocytes more than 12000 or less than 4000, or more than 10 % of unripe forms of leukocytes. Diagnostic information these attributes it is rather great and at presence of the center of an infection these symptoms should guard, as the sepsis is the phasic process leading development of a polysystem inconsistency and deep hemodynamic infringements , hypoxigen, a metabolism. It is necessary to note, that the sepsis is a dynamic pathological process which initial displays can quickly pass in a fatal stage of multiorgan insufficiency and an irreversible toxics-septic shock. It is necessary to pay attention to ways of penetration of an infection to a vascular channel and the reasons of development septic endotoxicosis. To note features of current of a toxics -septic shock at Gram-negative microflora, a mephitic gangrene and a staphylococcal bacteriemia. To disassemble mechanisms of formation the factor of necrosis tumors, proinflammatory cytokines, endogenous toxins and to emphasize their role in development of set of the pathological reactions defining weight endtoxics. To pay attention on pat morphology aspects septic endtoxics.
Clinical picture of a sepsis - a basis of its diagnostics. The major method of acknowledgement of the diagnosis at a sepsis is the microbiological blood analysis, separated of wounds, the purulent center, and as urine, separated of belly and chest cavity. Thus essential value has not only identification of the found out microorganisms, but also their degree , and also sensitivity antibacterial preparations.
Features of a clinical picture, as a rule, depend on extensiveness and character of the primary purulent center. Now clinical and laboratory attributes of the system inflammatory answer, a sepsis, a heavy sepsis and a toxic-septic shock are precisely formulated. It is necessary to note value of modern methods of tool diagnostics (ultrasonic scanning, a computer tomography) in revealing the primary center and an establishment of indications to volume and character of operative intervention, for revealing of the primary purulent center important for successful treatment of a sepsis of any genesis. Special value has it for a surgical intervention as successful operative sanitation of the center is impossible without the topic diagnosis. Special attention to turn on the abdominal sepsis complicating current of various intrabelly inflammatory and destructive processes. The abdominal sepsis represents most a challenge as in the diagnostic and medical plan, and economically. In structure of an abdominal sepsis the priority place is borrowed with a peritonitis and pyoinflammatory complications of a destructive pancreatitis. It is necessary to note a role of gastrointestinal decompression, enterosorbtion and intestinal oxygenations in knocking over of «an intestinal intoxication» and in struggle against a multiorgan inconsistency at an abdominal sepsis.
Intestinal insufficiency - the major component of a vicious circle at a sepsis as translocation of bacteria and their toxins from intestines in a belly cavity and in portal system supports inflammatory reaction, aggravating infringement of a metabolism. Thus infringements practically all functions of a gastrointestinal tract - barrier, metabolic, immunoprotection and endocrinic are observed. Conservative treatment of a surgical sepsis includes: the directed antibioticotherapia, correction electrolytic balance, AAC, hemoreologycal, and also an oxygen mode of blood with use of methods of an oxygenotherapy and AVP, hyperbaric oxygenation; intravenous infusions of glucose, albuminous preparations, blood; a hormonetherapy, application antihistamine preparations and vitamins, cardiotropic medicines and hepoprotectors. It is necessary to bring to a focus to value and features of an immunotherapy of a sepsis. To note the role recombinant interleycine - 2 (roncoleycin), antibodies, and others imunomodulation preparations in treatment of a sepsis and septic endotoxicosis. To disassemble indications to carrying out extracorporeal methods hemocorrection: a hemodialysis, hemofiltration, hem and lymphosorbtion, plazmopheresis, ultrafiltrations and extracorporal membranic oxygenations. To note expediency of a combination of various methods detoxication with UFO blood, etc. methods of quantum therapy.
Tasks for independent work
Efferent therapy in complex treatment of edotoxicosis.
Immunotherapy of a sepsis.
Role of the primary purulent center in development of a sepsis.
Radical surgical treatment of the purulent centers at sick of a sepsis.
TESTS
1. The local signs of septic wounds are as follows:
1. Copious purulent exudate.
2. Scanty purulent exudate.
3. Marked local hyperaemia.
4. Dirty-grey wound tissues.
5. Pronounced local oedema.
Choose the right combination of answers:
A. 1,3, 5. B. 4, 5. С. 2, 4, 5. D. 2, 4. E. 2, 5.
2. The common clinical signs of sepsis are as follows:
1. Fever.
2. Dizziness.
3. Adynamia.
4. Bradycardia.
5. Rigors.
6. Profuse perspiration.
Choose the right combination of answers:
A. 4, 5. B. 2, 4, 5. С. 2, 3,5. D. 1,2, 3. E. 1,3,5, 6.
3. The typical signs of sepsis are as follows:
1. Fever.
2. Rigors.
3. Primary focus.
4. Bacteraemia.
5. Jaundice.
Choose the right combination of answers:
A. 1,2, 3. B. 2, 4, 5. С. 1,4, 5. D. 3, 4, 5. E. 2, 3,4,5.
4. The septic fever may be of the following types:
1. Remittent.
2. Hectic.
3. Intermittent.
4. Inaccurate.
5. Continual.
Choose the right combination of answers:
A. 1, 2, 3, 5. B. 3, 4, 5. С. 1, 2, 4. D. 1, 3, 5. E. 1,2, 3,4, 5.
5. Suppurative absorption fever is characterized by the following signs:
1. Extensive primary purulent focus.
2. Evident in all types of the inflammation.
3. Specific causative agent.
4. Rapid exhaustion of patient.
5. Resolution with elimination of the purulent focus.
Choose the right combination of answers:
A. 1, 2, 3. B. 1, 3, 5. С. 3, 4, 5. D. 1, 3, 4. E. 1,2,4,5.
6. The major signs of bacterial toxic shock are as follows:
1. Fever.
2. Bradycardia.
3. Rigors.
7. What methods of treatment would you apply for intoxication:
1. Blood transfusion.
2. Detoxication.
3. Complete bed rest.
4. Antibacterial therapy.
5. Immunotherapy.
Choose the right combination of answers:
A. 1, 2, 3, 4. B. 2, 3, 4, 5. С. 3, 4, 5. D. 4, 5. E. 1,2,3,4,5.
8. The initial therapy of primary focus in sepsis may be as follows:
1. Surgical debridement of the wound.
2. Proteolytic enzymes.
Answers
1 - C, 2 - E, 3 - A, 4 - D, 5 - E, 6 - A, 7 - E, 8 - A.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
VARICOSE VEINS IN THE LOWER LIMB. CHRONIC LYMPHOVENOUS FAILURE. THROMBOPHLEBITIS (classification, clinic, diagnostics, treatment)
Составитель: доцент Ю.И.Ломаченко
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
Definitions.
Thrombophlebitis is inflammation and clotting in a vein.
Deep vein thrombosis is blood clotting in the deep veins.
Classification and Etiology
Thrombosis may affect superficial veins (superficial thrombophlebitis) or deep veins (deep vein thrombosis). Prolonged venous thrombosis may lead to chronic venous insufficiency, in which there is edema, pain, stasis pigmentation, stasis dermatitis, and stasis ulceration. Thrombosis is virtually always accompanied by phlebitis, thus the terms thrombosis and thrombophlebitis are used interchangeably. Thrombosis may occur on the basis of coagulation abnormalities that may be familial or related to an underlying malignancy.
Iliofemoral thrombophlebitis refers to extensive thrombosis of the involved extremity that has developed a milky white color. Phlegmasia cerulea dolens indicates a massive venous thrombosis, in which the leg is often blue. It often leads to venous gangrene and death due to underlying disease (eg, widespread malignancy).
Other eponyms describe thromboses in specific anatomic areas: pelvic vein, mesenteric vein, portai vein, renal vein, and jugular-mesenteric vein thromboses.
Endothelial injury can expose collagen, causing platelet aggregation and tissue throm-boplastin release that, when stasis or hypercoagulability is present, trigger the coagulation mechanism. Many factors may contribute to venous thrombosis: injury to the endo-thelium of the vein, eg, from indwelling catheters, injection of irritating substances, thromboangiitis obliterans, and septic phlebitis; hypercoaguiability associated with malignant tumors, blood dyscrasias, oral contraceptives, and idiopathic thrombophlebitis; and stasis in postoperative and postpartum states, varicose thrombophlebitis, and the thrombophlebitis that complicates prolonged bed rest of any chronic illness, heart failure, stroke, and trauma. Prolonged immobilization with the legs dependent while traveling (especially on long flights) is a risk factor, even in normal persons. Strenuous exercise of muscles in the affected extremity (eg, arm) is also a risk factor.
Septic phlebitis is possible whenever a septic process is present in the extremity distal to or at the ievel of the venous obstruction. Septic thrombi may form separately from the infectious focus or may occur in contiguity with the inflammatory area as part of a cellulitis.
Pathophysiology
Most venous thrombi begin in the valve cusps of deep calf veins. Tissue thromboplastin is released, forming thrombin and fibrin that trap RBCs and propagate proximally as a red or fibrin thrombus, which is the predominant morphologic venous lesion (the white or platelet thrombus is the principal component of most arterial lesions). Anticoagulant drugs (eg, heparin, the coumarin compounds) can prevent thrombi from forming or extending. Anti-platelet drugs, despite intensive study, have not proved effective for prevention.
Symptoms and Signs
Symptoms of acute thrombophlebitis arise over hours to 1 or 2 days. The disease is usually self-limited and lasts 1 to 2 wk, after which the acute process subsides and painful symptoms disappear.
In superficial thrombophlebitis, a thrombosed superficial vein can be palpated as a Hnear, indurated cord; it may be associated with variable inflammation manifested by pain, tenderness, erythema, and warmth and may need to be differentiated from acute secondary lymphedema with infection. Palpation of a superficial cord in the leg reflects occlusion of a superficial vein; it is seldom due to deep vein thrombosis.
Deep vein thrombosis (DVT) may be asymptomatic or may manifest over the involved area as combinations of tenderness, pain, edema, warmth, skin discoloration, and prominent superficial veins. DVT involving the popliteal, femoral, and iliac segments may be tender, with a hard cord palpable over the involved vein in the femoral triangle in the groin, medial thigh, or popliteal space. With iliofemoral venous thrombosis, dilated superficial collateral veins usually appear over the leg, thigh, and hip areas and lower abdomen.
Because at least three main veins drain the lower leg, thrombosis in one does not obstruct venous return, and there is no swelling, cyanosis of the skin, or dilated superficial vein. The patient complains of soreness or of pain on standing and walking that is usually relieved by rest with the leg elevated. On examination, deep calf tenderness can be elicited, but the pain of DVT is often difficult to differentiate from muscle pain. Pain from muscular causes will be absent or minimal on dorsiflexion of the ankle with the knee flexed but maximal on dorsiflexion of the ankle with the knee extended or during straight-leg raising (Homans' sign); thus, this test is unreliable for DVT. Loss of peripheral arterial pulses occasionally accompanies massive DVT, but venous thrombosis can also be secondary to acute arterial occlusion.
Chronic venous insufficiency in the leg after DVT manifests as edema and dilated superficial veins. The patient may complain of fullness, aching, or tiredness in the leg or may have no discomfort. Symptoms occur during standing or walking and are relieved by rest and elevation. There is no tenderness over the deep veins to indicate an acute thrombophlebitis, but a history of DVT should be elicited. Stasis syndrome occurs if edema is not controlled by an elastic support. With time, skin pigmentation appears on the medial and sometimes the lateral aspect of the ankle and lower leg. Further complications include stasis dermatitis and stasis uiceration in these areas. Patients with chronic venous insufficiency may develop varicose veins, which are secondary to DVT, are often mild, and function as collateral vessels. They should not be excised unless severe.
Diagnosis
Superficial thrombophlebitis is diagnosed by the symptoms and by finding a swollen, tender, superficial venous cord on examination.
Physical examination usually can differentiate acute arteria! from deep venous obstruction. In > 50% of cases, acute DVT cannot be diagnosed by clinical findings alone; Homans' sign should not be relied on for the diagnosis, and edema may be due to other causes. Specific limb findings (eg, edema, dilated superficial veins), evidence of pulmonary embolism, and the overall clinical setting, including risk factors, permit the physician to estimate the likelihood of DVT. The diagnosis can be confirmed by noninvasive testing or by venography if necessary. Duplex ultrasonography is diagnostic in most cases in which thrombus involves the iliac, femoral, or popliteal veins. If the diagnosis is in doubt, a venogram should be obtained. Pulmonary embolism can be sought with lung scan or pulmonary arteriogram. If overlooked, DVT may lead to death from pulmonary embolism, but use of anticoagulants without having demonstrated an intravascular thrombus on ultrasonography, venography, or lung scan risks serious hemorrhage.
Plethysmography, as with ultrasonography, can be used with acceptable accuracy to diagnose thrombotic obstruction of major proximai veins of the extremities or chronic venous insufficiency. It cannot detect DVT of the calf. Plethysmography is noninvasive and relatively inexpensive, requires minimal patient cooperation, and can be performed well by a trained technician. It is frequently used with duplex ultrasonography, and this combination enhances the accuracy of diagnosis. Patients may be treated if the results of either test are positive. If the results are negative and DVT is still suspected, venography should be done.
Prognosis
DVT is usually benign but can cause lethal pulmonary emboli or chronic venous insufficiency. Superficial thrombophlebitis alone, even when recurrent, causes neither of these serious complications, although nonlethal pulmonary emboli rarely originate in superficial veins.
Although superficial thrombophlebitis and DVT are more common in patients with cancer, the mechanism is obscure. Most clinically recognized episodes of DVT are not associated with cancer. However, when malignancy is the only risk factor in a patient with superficial thrombophlebitis or DVT, the malignant process is almost invariably advanced.
Treatment
Superficial thrombophlebitis requires no specific therapy other than relief of discomfort. Warm compresses over involved veins and NSAIDs are helpful. Hospi-talization is unnecessary, and antibiotics are not needed.
For DVT, the objectives of therapy are to prevent pulmonary embolism and chronic venous insufficiency. When acute DVT is diagnosed, the patient may be hospitalized initially. However, because of advances in heparin therapy, selected patients with DVT can be treated at home, reducing or eliminating hospitalization. The foot of the bed is elevated 6 in, and the patient heparinized; in either setting, bathroom or commode privileges can then be permitted. Drugs such as phenylbutazone or corticosteroids are not indicated routinely, and antibiotics should be used only for a specific infection. Warm moist packs are comforting but optional in patients without arterial insufficiency.
Low inol wt heparin is followed soon by oral warfarin, with the dosage adjusted to achieve an INR between 2 and 3. Duration of anticoagulant therapy depends on the patient. A single episode of thrombophlebitis subsiding clinically in 3 to 6 days in a young, active patient free of risk factors may require only 2 mo of therapy, but a patient with a demonstrable pulmonary embolus and persistent risk factors may require 6 mo of therapy. After >= 2 episodes of DVT, oral anticoagulant prophylaxis should be continued indefinitely. The value of antithrombotic drugs (eg, snake venoms, platelet antiaggre-gates, thrombolytic compounds) has not been established.
Thrombolytic therapy: Thrombolytic therapy using tissue plasminogen activator or urokinase in tandem with anticoagulants is effective for acute DVT of the popliteal and more proximal veins. The best results occur when the DVT has been present for < 48 to 72 hr. Complete or partial dissolution of thrombi usually occurs within 24 to 48 h. Successful treatment restores venous anatomy and thus may prevent valvular damage and resulting chronic venous insufficiency. Before thrombolytic therapy is used, the diagnosis must be confirmed by venography. The contraindications and adverse effects, especially bleeding, and the details of treatment and monitoring must be understood.
When edema subsides, the patient should be measured for a firm below-knee elastic stocking (providing 30 to 40 mm Hg pressure) to control the edema that will occur with ambulation. The stocking should be worn while the patient is ambulatory to prevent the postphlebitic sequelae of chronic venous insufficiency: edema, pain, stasis pigmentation, and subsequent stasis dermatitis and stasis uiceration. When these complications occur, treatment with an Unna's paste boot or bed rest with elevation and compression dressings will heal most ulcers. Antibiotics are usually indicated only when the ulcer is surrounded by severe acute cellulitis. Wet NaCI dressings may help to loosen superficial exudate and slough. Large refractory or recurrent ulcers may have to be excised, the incompetent perforating veins ligated, and the area covered with a split-thickness skin graft.
TESTS
1. The complications of lower limb thrombophlebitis are commonly due to:
1. Superficial vein thrombosis.
2. Superficial vein dilatation.
3. Femoral artery thrombosis.
4. Lower limb deep vein thrombosis.
Choose the right combination of answers:
A. 1,2. B. 2. С. 3,4. D. 4.
2. Thrombophlebitis is seen in -
a) Carcinoma ovary
b) Carcinoma breast
c) Carcinoma testes
d) Carcinoma stomach
3. Treatment of post thrombophlebitis involves the following methods:
1. Anticoagulants.
2. Antibiotics.
3. Bypass of the occluded vessel.
4. Insertion of a probe into the affected vessel's lumen.
5. Ligation and removal of the affected vein.
Choose the right combination of answers:
A. 1,2, 3. B. 1,4. С. 1,3, 5. D. 2, 5. E. 1, 2.
4. To assess the potency of venous valves, the following methods are used:
1. Trials by fingers and tourniquets signal.
2. Rheovasography.
3. Doppler ultrasonography.
4. Infrared thermography.
5. Contrast phlebography.
Choose the right combination of answers:
A. 1,2, 3. B. 1, 3, 5. С. 1,2, 3,4, 5. D. 2, 3, 4. E. 2, 3, 4, 5.
5. The causes of acute vein insufficiency are as follows:
1. Vein thrombosis.
2. Deep vein thrombophlebitis.
3. Obesity.
4. Varicose veins.
5. Traumatic venous injury.
Choose the right combination of answers:
A. 1, 3, 5. B. 1, 2, 4, 5. С. 2, 3, 4. D. 2, 3, 5. E. 1,2,5.
6. Preventive measures in post surgery deep vein thrombophlebitis include the following:
1. Antibacterial therapy.
2. Lower limbs bandaging pre- and postoperatively.
3. Prolonged postoperative bed rest.
4. Prevention of prolonged immobilization after surgery.
5. Intake of vasodilators.
Choose the right combination of answers:
A. 1,2. B. 4, 5. С. 2, 3,5. D. 2, 4. E. 1,3, 5.
7. The signs characteristic of acute deep vein thrombosis are as follows:
1. Acute local pain (in the affected limb).
2. Cutaneous pallor or cyanosis.
3. Fever.
4. Hyperaemia.
5. Pronounced swelling of the limbs.
Choose the right combination of answers:
A. 1,4. B. 1,2, 5. С. 1,3, 5. D. 2, 4. E. 3, 5.
8.Migrating thrombophlebitis is associated with cancer of-
a) Liver
b) Lung
c) Kidney
d) Pancreas
9. The most common vein to get thrombosed is the
a) Long saphenous
b) Short saphenous
c) Both
d) Posterior tibial
Answers
1 – D
2 – A,B,D
3 – A
4 – B
5 – B
6 – D
7 – B
8 – B, D
9 – D
References
Gostischev V. K. General surgery / The manual. – M.: GEOTAR-MED, 2003. – Charter XI. – P.150-191.
Moukonin A.A., Golub A.V. Venous and lymphatic disorders: Textbook for foreign students. – Smolensk: Smolensk State Medical Academy, General Surgery Department. – 2005. – 5p.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
CHRONIC ARTERIAL OCCLUSIVE DISEASES IN THE LOWER LIMB – AORTOILIAC DISEASE, DISEASE OF THE FEMORAL AND DISTAL ARTERIES (classic buerger disease, thromboangiitis obliterans). GANGRENE OF THE LOWER LIMB.
Составитель асс. А.А.Безалтынных
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
Basic information
Necrosis is the death of tissues of part or a whole organ of the living body.
Causes of necrosis are as follows:
• physical;
high or low temperatures;
radiation or electrical energy;
chemicals;
• Mechanical;
• pressure on or crushing of tissues.
These types of injury directly lead to necrosis of tissues. Local circulatory disorders (e.g. thrombosis, embolism or vascular occlusion) often result in indirect necrosis. The condition is accompanied by abnormal innervation when the nerves are damaged (e.g. leprosy, syringomyelia).
Necrosis can be:
coagulative, or dry (burns, dry gangrene);
colliquative, or wet (alkaline burns, wet gangrene).
The signs of necrosis become obvious within 4 to 6 hours after tissue death. The necrotic tissue undergoes rejection and, if located on the surface of an organ, an ulcer develops. Extensive necrosis with widespread tissue decay results in systemic absorption of toxic products, which, in turn, leads to intoxication.
GANGRENE
Necrosis due to primary blood circulatory disorders is referred to as gangrene.
Causes:
extensive crushing;
severe pressure on tissues;
vascular injuries;
organ compression (e.g. POP bandage);
volvulus with compression of the vessels;
leaving the tourniquet on a limb for a long time;
vascular thrombosis and embolism;
obliterating endarteritis;
obliterating arteriosclerosis.
Most commonly acute and chronic arterial occlusion lead to gangrene.
Dry gangrene is caused by fast dehydration of the necrotic tissues without bacterial contamination.
This results in tissue mummification. In wet gangrene, colliquative tissue necrosis occurs, which is usually complicated by an ichorous infection, with subsequent disintegration of the devitalised tissue and severe intoxication. The tissue debris is dirty-green or black in colour and smells very offensive.
Gangrene resulting from acute ischaemia of an organ is accompanied by severe ischaemic pain that is normally felt below the level of vascular occlusion. The colour of the limb changes very fast from pale to marble-bluish; it becomes cold and skin sensations disappear.
In dry gangrene, the gradual drying up of the necrotic area is followed by a clear-cut demarcation between the intact and necrotic areas. The skin becomes black, which is accompanied by minimum, if at all, intoxication. In wet gangrene the patient's condition is generally severe from the very onset (fever, tachycardia, chills, thirst, and dehydration) because of absorption of ichorous tissue disintegration products into circulation.
Over the areas of necrosis (often in the foot and the lower third of the leg) the skin becomes bluish with dark-red patches and haemorrhagic blisters. The extremity is oedematous, enlarged, and dirty-greyish tissues with offensive odour are visible (see fig. 126, colour inset).
Once the signs of necrosis appear, the limb is to be immobilised and an aseptic dressing applied.
Types of surgical treatment.
The treatment of necrosis depends on its cause. The common strategy of the management of all types of necrosis is the removal of the necrotic tissue, or necrectomy.
Necrectomy requires that several parallel incisions be done in the necrotic area without anaesthesia and an antiseptic dressing be applied. This contributes to the removal of the degenerated necrotic tissues and, therefore, reduces the intoxication of the body.
Necrectomy can be performed with a scalpel or scissors (mechanical necrectomy), proteolytic enzymes (chemical necrectomy), physical factors -ultrasound or laser rays (physical necrectomy).
It is advisable:
• in progressive wet gangrene, to undertake above-knee amputation (without waiting for tissue demarcation) without delay;
• in dry gangrene, to first allow the demarcation line appear and then amputate the limb above it within the intact area.
ARTERIAL OCCLUSION (ACUTE AND CHRONIC ARTERIAL INSUFFICIENCY)
Examining the patient with arterial diseases the surgeon has to consider a number of peculiarities:
The examination must occur in a warm room;
It is required that the symmetrical sites of the j limbs be inspected.
Skin color is compared on both limbs. Pale or violet-bluish discoloration acquired on moving the limb from the horizontal position to the vertical one strongly suggests deficient circulation. The skin is usually dry and scaly, and the nails are deformed, thickened and brittle; a loss of hair and muscle atrophy may also be observed.
The feeling of the arteries shows a weak or absent pulse. On the lower limb the pulse is to be felt on the femoral artery (below the middle of the Poupart's ligament), popliteal artery (in the popliteal fossa with the leg Hexed in the knee joint and the muscles maximally relaxed), dorsalis pedis artery (between the first and second metatarsal bones) and tibialis posterior artery (behind the medial malleolus). Pulsation on the upper limb will be evaluated on the subclavian, humeral and radial arteries.
Diagnostic procedures (investigations).
To assess the severity of arterial circulatory disorder special tests are performed.
Oppel test. Have the patient lie supine with his/her leg raised at an angle of 45°. The appearance of paleness on the sole (the plantar ischaemic sign) serves as the evidence of arterial circulation insufficiency.
Samuel's test. Have the patient lie in the position as described above and do 20 to 30 flexions in the ankle joint. The appearance of paleness on the sole is also a sign of arterial circulation insufficiency.
Moshkovich's test. Have the patient lie supine raise his/her leg and apply a tourniquet for 5 minutes. The period needed for the skin to regain hyperaemia following the removal of the tourniquet is normally 5 to 30 seconds whereas that in arterial occlusion is as long as 3 to 5 minutes.
The above-mentioned tests can only be diagnostic at initial, or compensated, stages of the disease. If intermittent claudication appears, the diagnosis is easy to make (the sub- and decompensation stages of circulatory failures).
Special methods are used to assess the severity of circulatory disorders, monitor pathologic progression and the efficacy of therapy. These are primarily as follows:
1. Thermometry, the technique of measuring skin temperature at symmetrical limb areas using an electric thermometer. A reduction in temperature by 0,5— 0,7°C strongly suggests deficiency in the blood flow.
2. Oscillograph, recording oscillations produced by changes in electrical potentials caused by vibrations of an artery. A decrease in vibration amplitude indicates deficient circulation.
Impedance rheovasography, the technique to register the resistance produced by pulsating limb arteries as a result of their filling. In health, the rheographical index is as high as 0.8-1.0; its reduction being evident of deficiency in the arterial circulation.
Doppler ultrasound, the method of listening to the arterial blood flow with the velocity detector (Doppler probe) to recognize arterial occlusion or stenosis.
Capillaroscopy, microscopical examination of the capillary vessels of the skin or nail beds. In occlusive arterial diseases the capillaries become convoluted, winding and constricted.
Arteriography, the visualisation of arteries by means of X-rays after injection of radio-opaque material. In obliterating atherosclerosis, the vessels with the «eaten up» internal contours, as well as areas of the constricted, or occluded, lumen are seen. In endarteritis, the arterial lumina are markedly narrowed, often over wide areas. Thrombosis/thromboembolism cause obstruction of the artery,
ACUTE ARTERIAL OCCLUSION
Suits from the sudden arrest of the blood flow in an artery and is the commonest cause of gangrene.
The factors that contribute to arterial occlusion include trauma, the excessive pressure from a tourniquet, intra-operative ligation of the artery, thromboembolism (i.e. the obstruction of a vessel, mainly by thrombus and occasionally by air, fat).
Arterial embolism results in ischaemia of the limb, the severity of which depends on the size of the thrombosed vessel, the level of obstruction, the capacity of the collateral circulation as well as the duration of the problem (the time lag between the moment of occlusion and the reporting time).
In thromboembolism of a major artery, the sign of acute organ ischaemia (e.g. the limb) is observed. Thromboembolism causes the following pathogenic changes:
obstruction of a main vessel;
acute distension of the vessel above the area of obstruction;
reflex spasm of all the arterial network of the limb — the obstructed vessel, its branches and collaterals beneath the area of obstruction;
formation of a sequel thrombus beneath the area of obstruction because of a decrease in blood flow and defects of blood coagulation and anticoagulation systems.
To verify the diagnosis and identify of the level of occlusion special investigations are applied: cutaneous thermometry, oscillograph, rheography and angiography.
According to V. Saveliev, the clinical course of thromboembolism of the major vessels divides into three stages:
• stage 1 - ischaemia causing functional disorders. This lasts a tew first hours. The clinical picture includes (I) acute pain in the limb affected, pale and cool skin, absent pulse on the peripheral arteries. It is noteworthy that pain and touch senses usually remain intact, active joint motions are slightly limited. The restoration of blood supply to the limb at this stage leads to a full functional recovery;
stage 2 — structural changes — includes such signs as absent pain and touch sensations, markedly limited active and passive joint movements, muscular oedema and contractures, bluish discolouration of the skin. This stage lasts for 12 to 24 hours. The restoration of blood supply within the above-mentioned period, can save the limb although its functions are, as a rule, either partially or fully lost;
stage 3 — necrosis — is characterised by the development of gangrene. It follows within 24 to 48 hours after embolisation. At this stage, due to gangrene virtually all forms of sense and movement will be lost, while resume of the blood flow in the vessel can occasionally reduce the level of the demarcation line, hence the level of amputation.
The staging of ischaemia helps choose the therapeutic modality:
stages I and 2 require radical treatment - restoration of the arterys patency (i.e. restoration of the blood flow);
stage 3 precludes the aforementioned therapy as the necrosis of an extremity is a life-threatening condition and thus calls for urgent options, of these the amputation of the limb affected being the mainstay.
The clinical features of the disease, leg pain particularly, may readily be identified the moment embolisation has occurred. The severe ischaemic pain, which results not only from occlusion but also from the reflex spasm of collateral vessels, is of sudden onset and of persistent duration. Occasionally, it can produce shock. The pain is mostly often located at the distal parts of the limb; it sometimes appears at the area of occlusion and spreads distally later on. Alternatively, the patient may present with numbness sensation, paraesthesia (tingling), while coolness to touch and pain come on thereafter. This suggests that the incomplete occlusion of the artery by an embolus precedes the complete one due to secondary thrombosis that causes limb ischaemia.
The incidence of the subacute course of thromboembolism of a major artery is as high as ten percent.
The patients with arterial thromboembolism are usually those with serious cardiac disease, which accounts for the severity of their condition.
Physical examination yields helpful clinical signs as follows:
1. Vital signs:
increased pulse rate;
low blood pressure (a sign of impending shock);
labial and mucosal cyanosis;
fast breathing.
2. Skin:
a change in the skin colour, which becomes cyanotic, pale or even white with bluish patches («the marble skin») that resemble those of the cadaver:
coolness to touch is more pronounced at the peripheral areas; skin temperature is reduced by 2-3 °C as compared to that of the intact side;
both pain and touch sensations checked with a needle are diminished. The inability of the patient with their eyes closed to distinguish between being pricked by a sharp object and touched by a blunt one indicates the loss of both pain and touch sensations. This suggests irreversible damage to the tissues as the circulation in the limb fails to maintain the viability of tissues.
3. Pulses:
• absent lower limb pulse is a typical sign.
4. Neurologic signs. It should be emphasized that neurological signs
(numbness sensation and paraesthesia with subsequent loss of all kinds of sensation) become visible very fast. The pain can shortly be followed by motor deficit of various degrees (finger and toe paralyses).
The combination of pulselessness with paresthesias, acute pain, pallor and palsy are therefore diagnostic of acute arterial ischaemia.
If measures are not taken to restore circulation, the signs of acute ischaemia progress and gangrene, which is usually dry ensues.
Treatment. The first aid in arterial thromboembolism includes:
analgesia and cardiac medications;
transport immobilisation of the limb either by a standard or an improvised splint;
application of ice packs to the affected limb;
immediate transportation of the patient to the surgical unit.
The management of the patient with arterial thromboembolism must be individualised depending on the location of the embolus; the stage of disease and its duration.
The preoperative treatment should start with conservative measures. Failure of ischaemia to subside and (hat of pain to relieve and touch sensations to recover within 2 hours of the therapy is an indication for surgery.
The conservative treatment is applicable:
at the initial stages of the disease (i.e. within 6 hours from its onset of disease);
in critically-ill patients;
in embolism of small arteries (i.e. those of the foreleg and forearm);
in obscure clinical picture;
as a method additional to surgery. Jt involves the following:
Anticoagulation therapy (heparin, indirect anticoagulants) and fibrinolytic agents (streptokinase, streptodecase, urokinase) to prevent formation of clots and lyse the the preformed ones;
Antispasmodic therapy to eliminate the vascular spasm (vasodilators, novocain block, papaverin, carbacholin);
Improvement of collateral circulation (Bernard's current; vacuum apparatus applied to the limb).
Surgical treatment simplies radical operations (i.e. embolectomy arterioplasty and vascular shunting) to restore the patency of arteries, whereas alliative ones are performed to improve the collate -"al circulation without restoring the patency of the ain vessel (e.g. sympathectomy). The gangrenesnt limb is subject to amputation.
CHRONIC ARTERIAL OCCLUSION
Chronic arterial occlusion is a condition caused (he gradual narrowing of an artery with the re-ant ischaemia of the limb.
Causes of chronic ischaemia of the limb include following:
Thromboangiitis obliterans (Indarterilis Buerger's disease) and Raynaud's disease. Thromboangiitis is the inflammation of the entire wall and connective tissue surrounding medium - sized arteries and views especially of the legs of young and middle-aged men.
Raynaud's disease has a vasospastic origin and affects mainly the upper limbs.
Obliterating artheriosclerosis that results from artheriosclerotic narrowing and occlusion of the vascular lumina.
It is chronic arterial insufficiency that underlies each of these diseases and produces the ischaemic syndrome. The diagnosis is based on the degree of the arterial insufficiency and its progression rate.
History:
pain (it is usually the earliest complaint);
intermittent claudication: severe pain in the legs, tension and weakness on walking which makes the patient stop. The symptoms increase as walking proceeds until further progress is impossible (being the chief but late symptom, it indicates pronounced disorder in the limb circulation, even though most patients associate it with the beginning of their disease).
The severity of the syndrome correlates directly with the degree of ischaemia:
degree I (the pain follows the walking of 500 m);
degree II (the pain is evident on walking 200 m);
degree III (the pain appears after walking 20-30 m or at rest);
degree IV (the signs indicative of necrosis, or gangrene).
The clinical stages of chronic arterial insufficiency are as follows:
Stage I, or compensation History:
fatigability, a feeling of pressure and pain in the gastrocnemii muscles on walking;
coolness in the feet, intermittent claudication on walking 200-500 m, numbness and tingling sensation at the finger and toe tips, muscular weakness;
past medical history indicative of heavy tobacco smoking, long exposure to cold and frequent stress.
Physical examination of the limbs:
• minimum physical signs: hair loss, skin pallor, coolness to touch mostly confined to the fingers and toes, diminished peripheral pulses, «white patches» on pressing the feet.
Stage II, or subcompensation, is characterised by transient ischaemia History:
• a feeling of cold fingers and toes; intermittent claudication more pronounced than at stage I;
transient ischaemia (subsides on resting);
effectiveness of conservative therapy. Physical examination:
pallor and coolness of the foot skin. Stage III, or decompensation History:
• severe pain at the fingers or toes, sole, dorsum of the foot and occasionally in the leg, both on walking and at rest, presumably nocturnal, which makes the patient sit up in bed with their legs on the floor and therefore interferes with their night sleep.
Physical examination:
dry and pale skin with bluish patches of ulceration (i.e. foci of necrosis) and oedema on one of the toes and fingers;
thickened and brittle nails;
muscle atrophy;
absent arterial pulse on the feet.
Stage IV, or gangrene History:
persistent and unbearable pain. Physical examination:
marked oedema and cyanosis with bluish black discolouration of the whole foot;
wrinkling of the skin (which suggests dry gangrene);
superimposed infection (which leads wet gangrene).
OBLITERATING ARTERIOSCLEROSIS
Obliterating arteriosclerosis, which is a local presentation of generalised atherosclerosis, often produces chronic deficiency of arterial blood supply to the lower limbs and is manifested by ischaemia of the anatomic sites. The major arteries - bifurcation of the aorta, and iliac, femoral and the popliteal arteries - are most commonly involved. In contrast, the upper limb vessels may hardly ever be affected.
History:
The risk factors include the following:
age over 50 years;
heavy tobacco smoking;
coronary heart disease (e.g. myocardial infarction);
cerebrovascular disease;
hypertension;
metabolic disorders (e.g. diabetes mellitus, hypercholesterolemia, vitamin deficiency);
history of long exposures of the feet to cold;
stress.
Clinical picture:
• patients tend to look old for their age;
femoral pulses are often absent;
the areas of necrosis on the foot may not be present.
Diagnostic studies:
angiography shows jagged and defective arterial walls with proximal occlusion of the arteries.
X-ray films help detect calcifications of the vessels.
Treatment:
vasodilating agents;
anticoagulant therapy (indicated in thrombosis),
• health resort therapy.
Occlusion of main artery is an indication for reconstructive surgical procedures (e.g. bypass graft) while gangrene invariably requires amputation of the limb affected.
ENDARTERITIS OBLITERANS
The disease starts with the involvement of the small vessels of the lower limbs; occasionally, those of the upper limbs may also be affected.
History
The risk factors are usually as follows:
age under 40 years;
frequent psychological stress;
heavy tobacco smoking;
rarely, history of
coronary heart disease;
cerebrovascular disease;
hypertension;
diabetes mellitus;
history of long exposures of the feet to cold frostbites.
Clinical picture:
Pulsation in the foot, and rarely thigh, is reduced or absent. In spite of the pressure of pulsation on one of the arteries of the foot or the popliteal pulse, necrosis appears over the toes.
Diagnostic studies:
• angiogram demonstrates smooth vascular walls and narrowing of the peripheral arteries.
In thromboangiitis obliterans, apart from the characteristic features of endarteritis, there is evidence of phlebitis or thrombophlebitis. The progression of the disease may often lead to wet gangrene.
Treatment:
analgesics;
nonsteroidal anti-inflammatory drugs;
antihistamines;
vasodilating agents, including those that payse transmission across the synapses;
female sex hormone therapy (synoestrol, folliculin); physiotherapy (ultra-high frequency current; Of the surgical methods, operations on the sym-Bernard's current; electrophoresis with drug pathetic nervous system are commonly performed preparations); (lumbar, thoracic and periarterial sympathectomy).
health resort therapy. Amputation takes priority in gangrene.
KEY QUESTIONS FOR HOMEWORK:
1. The complications of lower limb thrombophlebitis are commonly due to:
Superficial vein thrombosis.
Superficial vein dilatation.
Femoral artery thrombosis.
Lower limb deep vein thrombosis.
Choose the right combination of answers:
A. 1,2 B. 2 C. 3,4 D. 4
2. The typical signs of obliterating endarteritis are as follows:
Creeping sensation.
Chilly sensation in the feet.
Local hair falling.
Intermittent claudication.
Thickening nails.
Choose the right combination of answers:
A. 1,2 B. 3,4,5 C. 1,3 D. 2,4 E. 1,2,3,4,5
3. The characteristic signs of lower limb arterial thromboembolism are as follows:
1. Slowly progressing pain.
2. Sudden acute pain.
3. Bluish discolouration of the skin.
4. Skin pallor
5. The limbs' coolness to touch.
Choose the right combination of answers:
A. 1,2,3 B. 2,3,4 C. 4,5 D. 2,4,5
4.The causes of lymphatic circulatory disturbance are as follows:
1. Lymphatic vessel hypoplasia.
2. Erysipelas.
Chronic lymphadenopathy (tuberculosis, syphilis).
Vascular constriction by tumours or scars.
Atherosclerosis obliterans.
Choose the right combination of answers:
A. 1,2 B. 1,2,3,4 C. 2,3,4,5 D. 3,4,5 E. 1,3,4
5. Treatment of post thrombophlebitis involves the following methods:
1. Anticoagulants.
2. Antibiotics.
3. Bypass of the occluded vessel.
4. Insertion of a probe into the affected vessel's lumen.
5. Ligation and removal of the affected vein.
Choose the right combination of answers:
A. 1,2,3 B. 1,4 C. 1,3,5 D. 2,5 E. 1,2
6. To assess the potency of venous valves, the following methods are used:
Trials by fingers and tourniquets signal.
Rheovasography.
Doppler ultrasonography.
Infrared thermography.
Contrast phlebography.
Choose the right combination of answers:
A. 1,2,3 B. 1,3,5 C. 1,2,3,4,5 D. 2,3,4. E. 2,3,4,5.
7. The causes of pulmonary embolism are as follows:
Obliterating thrombosis of superficial veins.
Thrombus of the femoral artery.
Floating thrombus of the vena cava.
4. Diffuse thrombus of the skin and femoral veins.
5. Thrombus of the sapheno-femoral anastomosis.
Choose the right combination of answers:
A. 1,2,5 B. 2, 3,4 C. 2,3 D. 3,4,5 E. 3,4
8.The agents for pathogenic treatment of obliterating endarteritis are as follows:
Desensitizors.
Corticosteroids.
Vasodilators.
Platelet aggregation inhibitors.
Antibiotics.
Choose the right combination of answers:
A. 1,2,3 B. 2, 3,4 C. 2,4 D. 1,3, 4 E. 2,3
9.The risk groups of obliterating endarteritis are as follows:
Children.
20-40 year-old men.
50-60 year-old women.
Smokers.
Patients after frostbite.
Choose the right combination of answers:
A. 1,5. B. 1,2,3. C. 2,3,5.D. 2,4,5. E. 2,4.
10. The causes of acute vein insufficiency are as follows:
Vein thrombosis.
Deep vein thrombophlebitis.
Obesity.
Varicose veins.
Traumatic venous injury.
Choose the right combination of answers:
A. 1,3,5. B. 1,2,4,5. C. 2,3, 4. E. 1,2,5.
11.Preventive measures in post surgery deep vein thrombophlebitis include the following:
Antibacterial therapy.
Lower limbs bandaging pre- and postoperatively.
Prolonged postoperative bed rest.
Prevention of prolonged immobilization after surgery.
Intake of vasodilators.
Choose the right combination of answers:
A. 1,2. B. 4, 5. C. 2,3,5. D. 2.4. E. 1,3, 5.
12.The signs characteristic of acute deep vein thrombosis are as follows:
Acute local pain (in the affected limb).
Cutaneous pallor or cyanosis.
Fever.
Hyperaemia.
Pronounced swelling of the limbs. Choose the right combination of answers:
A. 1,4. B. 1,2,5. C. 1,3,5. D. 2,4. E. 3,5.
13.The causes of gangrene are as follows:
Major vessel embolism.
Arterial injuries.
Arterial thrombosis.
Frostbite.
Bum.
Choose the right combination of answers:
A. 1,2. B. 1,3,4. C. 2,4,5. D. 1,2,3,4,5.
14.Common causes and risk factors of moist gangrene are as follows:
Acute circulatory defect in the limbs.
Obesity.
Putrid wound infection.
Defective perfusion of the viscera (the bowel, lungs).
Obliterating endarteritis.
Choose the right combination of answers:
A.1,2,3,5. B.1,3,4,5. C. 1,2,3,4. D. 1,2,4,5. E. 1,2,3,4,5.
15.Dry gangrene is characterized by:
Inclination to putrid infection.
Demarcation line.
Pronounced intoxication.
Absence of intoxication.
5. Mummification of necrotic tissues.
Choose the right combination of answers:
A. 1,2. B. 2, 3. C. 1,3. D. 1,4. E. 2, 4, 5.
16.The clinical signs of limb moist gangrene are as follows:
Oedema and local skin discolouration.
Intoxication.
Delimitation of necrotic areas.
Offensive smell.
Absence of the demarcation line.
Choose the right combination of answers:
A.1.2. B.1,3,4, 5. C.2,4. D.1,2,4, 5. E.2, 3.
17.The appropriate treatment of limb moist gangrene with severe intoxication and fever may be as follows:
Necrectomy.
Limb bandaging with antiseptics.
Intra-arterial injection of antibiotics.
Local hyperbaric oxygenation.
Amputation of the affected limb.
Choose the right combination of answers:
A. 1,2. B. 2,3. C. 1,2,3,4. D. 3,4. E. 5.
18.The appropriate surgery for varicose ulcers may be as follows:
Ulcer dissection.
Autodermic plastics.
Secondary suturing.
Pathogenic treatment.
Grafting of the ulcer surface with jump graft.
Choose the right combination of answers:
A. 1,2. B. 3,4. C. 2,4,5. D. 2, 3. E. 1,2,4,5.
19.The causes of varicose ulcers are as follows:
Venous circulatory defect.
Arterial circulatory defect.
Lymph circulatory defect.
Spinal or neural.
Diabetes mellitus.
Choose the right combination of answers:
A.1,2,3. B.2,3,4. C.1,2,3,4. D.1.2,3,5. E. 1.
FURTHER READING
1. Oxford Textbook of Surgery. - http://med-lib.ru/english/index.shtml
2. Short Practice of Surgery / Edited by R.C.G.Russell, Norman S. Williams, Christopher J.K. Bulstrode. – 24 th Edition. – Chapter 68, chapter 71. – P. 1153-85, 1219-41.
3. Bell, P.R.F., Jamieson, C.W. and Ruckley, C.V. The Surgical Management of Vascular disease, W.B. Saunders, London, 1992.
4. Galland, R.B. and Clyne, C.A.C. Clinical problems in vascular surgery, Edward Arnold, London.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
INFLAMMATARY DISEASES OF THE SKIN AND SUBCUTANEOUS (erysipelas, cellulites, abscess, furuncles and furunculosis, carbuncle)
Составитель: доцент Ю.И.Ломаченко
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
ERYSIPELAS
A superficial cellulites with marked lymphatic vessel involvement caused by group A (or rarely group С or G) -hemolytic streptococci.
An interdigital fungal infection of the foot may provide a nudes for infection. The legs are the most frequent anatomic location.
Symptoms, Signs, and Diagnosis
The lesion is well demarcated, shiny, red, edematous, indurated, and tender, vesicles and bullae sometimes develop. The face (often bilaterally), arms, and legs are the most common sites, although not in that order. Patches of peripheral redness and regional lymphadenopathy occasionally occur. High fever, chills, and malaise are common. Erysipelas may be recurrent and may result in chronic lymphedema.
The characteristic appearance suggests the diagnosis. The causative organism is difficult to culture from the lesion but may occasionally be cultured from blood. Staining bacteria by direct immunofluorescence may also identify the causative organism, but the diagnosis is usually based on clinical morphology. Erysipelas of the face must be differentiated from herpes zoster, angioneurotic edema, and contact dermatitis; erysipelas of the arm or hand, from the rare erysipeloid.
Treatment
Penicillin V or macrolide antibiotics (erythromycin) should be given for >= 2 wk. In acute cases, penicillin G should be given parenteraly and than should be replaced by oral therapy after 36 to 48 h. Local discomfort may be relieved by cold packs and analgesics. A fungal nidus may require long-term antifungal therapy (itraconazole or terbinafine) to prevent recurrence.
CELLULITIS
Diffuse, spreading, acute inflammation within solid tissues, characterized by hyperemia, WBC infiltration, and edema without cellular necrosis or suppuration.
Etiology
Streptococcus pyogenes (group A-hemolytic streptococcus) is the most common cause of superficial cellulitis; diffuse infection occurs because streptokinase, DNase, and hyaluronidase - enzymes produced by the organism - break down cellular components that otherwise would contain and localize the inflammation. Group В, С, D, or G -hemolytic streptococci are less common causes. Staphylococcus aureus occasionally produces a superficial cellulitis typically less extensive than that of streptococcal origin and usually only in association with an open wound or cutaneous abscess. Superficial cellulitis caused by other organisms, primarily aerobic gram-negative bacilli, occurs rarely (generally in special circumstances). With granulocytopenia, diabetic foot ulcers, or severe tissue ischemia, aerobic gram-negative bacilli may be responsible.
Cellulitis occurring after animal bites may be caused by unusual bacteria from dogs and cats. Immersion injuries in fresh water may result in cellulitis caused by Aeromonas hydrophila in warm salt water, Vibrio vulnificus may cause cellulitis.
Symptoms and Signs
Infection is most common in the lower extremities. A cutaneous abnormality (e.g., skin trauma, ulceration, tinea pedis, dermatitis) often precedes the infection; areas of lymphedema or other edema seem especially susceptible. Scars from saphenous vein removal for cardiac or vascular surgery are common sites for recurrent cellulitis, especially if tinea pedis is present. Frequently, however, no predisposing condition or site of entry is evident. The major findings are local erythema and tenderness, frequently with lymphangitis and regional lymphadenopathy. The skin is hot, red, and edematous, often with an infiltrated surface resembling the skin of an orange. The borders are usually indistinct, except in erysipelas, a type of cellulitis in which the raised margins are sharply demarcated. Petechiae are common, large areas of ecchymosis, rare. Vesicles and bullae may develop and rupture, occasionally with necrosis of the involved skin. Systemic manifestations (fever, chills, tachycardia, headache, hypotension, delirium) may precede the cutaneous findings by several hours, but many patients do not appear ill. Leukocytosis is common but not constant.
Diagnosis
The diagnosis usually depends on the clinical findings. Unless pus has formed or an open wound is present, the responsible organism often is difficult to isolate, even on aspiration or skin biopsy. Blood cultures are occasionally positive. Serologic tests, especially measurement of rising titers of anti-DNase B, confirm a streptocqecal cause but are usually unnecessary.
Although cellulitis and deep vein thrombosis usually are easily differentiated clinically, many physicians confuse these entities when edema occurs in the lower extremities.
Course and Prognosis
Local abscesses form occasionally, requiring incision and drainage. Serious but rare complications include severe necrotizing subcutaneous infection and bacterernia with metastatic foci of infection. Even without antibiotics, most cases of superficial cellulitis resolve spontaneously; however, recurrences in the same area are common,
sometimes causing serious damage to the lymphatics, chronic lymphatic obstruction, marked edema, and, rarely, elephantiasis. With antibiotics, such complications are uncommon. Symptoms and signs of superficial cellulitis usually resolve after a few days of antibiotic therapy.
Treatment
For streptococcal cellulitis, penicillin is the drug of choice. For severe infections, which require hospitalization, parenteral introduction of drug is indicated. In penicillin-allergic patients, macrolides are effective for mild infections, and lincosamides (parenteral clindamycin) for severe infections. For penicillin-allergic patients or those with suspected methicillin-resistant S. aureus infection, vancomycin is the drug of choice. When pus or an open wound is present, results of a Gram stain should dictate antibiotic choice. Immobilization and elevation of the affected area help reduce edema, and cool, wet dressings relieve local discomfort.
ABSCESS (BOIL)
This is a localized accumulation of pus in different tissues or organs resulting from suppurative tissue disintegration and cavity formation unlike an empyema, which involves the accumulation of pus into natural body cavities and cavities of hollow organs.
The agents of infection are normally staphylococci in the form of a monoculture or in association with other microbes – E. Coli, proteus, streptococcus, bacterioides etc.
The infectious agents normally enter the organism from outside (exogenic infections), but can also invade the body from within (endogenic) – as for instance, when the organisms enter from neighboring or distant organs, metastatic abscesses in cases of sepsis. Abscesses can result from the injection into tissues of concentrated solutions of drugs – 25% solutions of magnesium sulphate, 24% solutions of cordiamin, 50% solutions of analgin etc. The development of suppurative inflammation leads to tissue disintegration and sometimes necrosis with rejection of the dead tissues – sequestration. Sequestra can subsequently dissolve when acted upon by enzymes. The form of the abscess cavity can be a simple one or complex with several pockets. The abscess wall is initially covered with purulent fibrinous deposits and fragments of necrotic tissues. Then an inflammation zone develops at the periphery leading to the formation of the pyogenic membrane made up of connective tissue.
An abscess that has resulted from a suppurative or aseptic inflammation can have different outcomes: spontaneous opening (burst) outside (abscess of the subcutaneous fatty layer, abscess of the muscles, mastitis, paraproctitis etc.), burst opening of an abscess into a closed cavity (abdominal, pleura, in a joint space etc.). An abscess can also open into a hollow cavity that has a connection to the outside (the intestinal lumen, the urinary bladder etc.). Under favourable conditions an abscess cavity decreases in size after the pus has evacuated, collapses and heals up by scarring; when evacuation is not complete the process can develop into a chronic one with formation of a fistula at the site where it burst.
Superficially located abscesses are marked by redness, swelling, pain, local rise in temperature, functional disorders and sometimes fluctuations can be elicited. The sites of infection may vary in size. The characteristics of the pus contained in an abscess cavity (consistency, colour and odour) depend on the type of causative agent involved: foul-smelling odour, dirty grey colour of pus is characteristic of ichorous strains; thick yellowish green pus – for staphylococcus; a bluish-green colour and sweetish smell – pseudomonas bacilli etc.
General clinical features of an abscess are: a rise in body temperature from subfebrile to high, general malaise, weakness, loss of appetite and headache. The peripheral blood picture shows leucocytosis with neutrophilia and a shift of the leukocyte count to the left. ESR is raised.
Signs of intoxication that occur in cases of serious abscesses can result from the absorption of toxic products from the focus of infection (suppurative resorptive fever), as well as from the development of sepsis.
An abscess has to be differentiated from haematoma, cysts and tumor degenerations. Diagnostic puncture can play a very important role here: when pus is obtained in this procedure it not only helps to establish the diagnosis in unclear cases but also can be sent for bacteriologic analysis – to isolate the agent and to determine its sensitivity to antibiotics.
The presence of gas – producing bacterial strains lead to the accumulation of gas in the abscess cavity, so-called gaseous abscess. Percussion over such an abscess gives a tympanic sound; X-ray films show the presence of gas bubbles with horizontal fluid levels beneath them (it is often observed in abscesses caused by agents of ichorous infections).
Treatment of an abscess is by incision, evacuation and drainage of the abscess cavity. Cold tuberculous abscesses are not to be incised since there is always the danger of causing superinfections by suppurative strains. Small abscesses with well-formed capsules have to be removed in whole without first opening them.
An abscess has to be incised using the shortest: surgical approach based on the anatomic and topographic peculiarities of the organ. Not infrequently an abscess is opened along a needle: the abscess is initially punctured with a needle, then the incision is made along the needle into the abscess cavity. The incision has to be made as much as possible towards the lower poles in order to create better conditions for drainage.
In order to reduce contamination of the surrounding tissues during the process of incision, the surgical field is well isolated by gauze or napkins and after a small incision into the cavity an electric suction machine is used to evacuate the pus. After the pus has been suctioned, the incision is increased, the cavity is explored by using the finger, breaking in the process the lacunae, and tissue sequestra are removed. All manipulations should be done carefully, so as not to destroy the pyogenic membrane. The abscess cavity is washed with an antiseptic solution, and then drained with one or several plastic or PVC tubes, or gauze swabs soaked with some proteolytic enzymes and antiseptics are packed into the cavity for drainage purposes. If drainage through the main incision is not adequate, another one is made on the opposite side – counter-aperture. Treatment of abscesses after incision and drainage is identical to that for treating infected wounds.
General therapeutic measures include body fortifying therapies, blood and plasma transfusions, and prescription of antibiotics taking into consideration the sensitivity results of the microbiologic analysis, specific therapeutic modalities (immunization with staphylococcal anatoxin, specific anatoxin etc.).
FURUNCLES
Acute, tender, perifollicular inflammatory nodules resulting from infection by staphylococci.
The condition often occurs in healthy young persons. Clustered cases may occur among teenagers living in crowded quarters with relatively poor hygiene or among contacts of patients infected with virulent strains.
Symptoms and Signs
Furuncles occur most frequently on the neck, breasts, face, and buttocks but are most painful when on skin closely attached to underlying structures (e.g., on the nose, ear, or fingers). The initial nodule becomes a 5- to 30-mm pustule that discharges a core of necrotic tissue and sanguineous pus. Furuncles may recur. Material for culture should be obtained from patients with single furuncles on the nose or central face, from patients with multiple furuncles, and from immunosuppressed patients.
Treatment
Treatment is incision and drainage or application of liquid soap containing either chlorhexidine gluconate with isopropyl alcohol or 2 to 3% chloroxylenol, which may be prophylactic but is not therapeutic. A single furuncle is treated with intermittent hot compresses to allow the lesion to point and drain spontaneously. A patient with a furuncle in the nose or central facial area and patients with multiple furuncles should be treated with systemic antibiotics. Usually a penicillinase-resistant penicillin (amoxicillin/clavulanic acid) or cephalosporins (cephalexin) are required. For recurrent furuncles, oral antibiotic therapy continuously for 1 to 2 months may be advisable. Patients with recurrent furunculosis should be evaluated for predisposing factors, including obesity, diabetes, occupational or industrial exposure to inciting factors, and nasal carriage of S. aureus.
CARBUNCLES
A cluster of furuncles with subcutaneous spread ofstaphylococcal infection, resulting in deep suppuration, often extensive local sloughing, slow healing, and a large scar.
Carbuncles occur most frequently in males and most commonly on the nape of the neck. Although carbuncles occur in healthy persons, diabetes mellitus, debilitating diseases, and old age are predisposing factors. Carbuncles develop more slowly than single furuncles and may be accompanied by fever and prostration. Treatment is the same as for clusters of furuncles.
TESTS
1. Therapeutic measures in furuncles are as follows:
1. Cleansing the surrounding skin with ethyl alcohol.
2. Pressing necrotic masses out and bandaging with 70% alcohol.
3. Injection of penicillin and novocain around the affected area.
4. Administration of oral sulphonamides.
5. Local ultraviolet irradiation.
Choose the right combination of answers:
A. 1,3,4,5. B. 1,2. С. 1,2,4,5. D. 3, 5. 3,4,5. E. 1, 2.
2. The therapies of erythaematous erysipeloid localized in the shin are as follows:
1. Moist bandaging with furacillin.
2. Antibiotics IM.
3. Desensitization (dimedrol, calcium chloride).
4. Local ultraviolet irradiation.
5. Warm bath with the potassium permanganate.
Choose the right combination of answers:
A. 1, 2, 3. B. 2, 3, 4. С. 2, 3, 5. D. 1, 2, 3, 5. E. 1,2,3,4,5.
3. The clinical signs characteristic of carbuncle are as follows:
1. Tender infiltrate.
2. Non-tender infiltrate.
3. Skin necrosis and pus pustules.
4. Necrosis with small haemorrhagic blisters.
5. Regional lymphadenopathy.
Choose the right combination of answers:
A. 1,3, 5. B. 2, 3, 5. С. 2, 4, 5. D. 1,3, 4. E. 1,4, 5.
4. The clinical stages of erysipelas are as follows:
1. Erythaematous.
2. Bullous.
3. Phlegmonous.
4. Suppurative.
5. Necrotic.
Choose the right combination of answers:
A. 1,2, 3,4. B. 2, 3,4, 5. С. 1, 2, 3, 5. D. 1, 3, 4, 5. E. 1,2, 3,4, 5.
5. Phlegmon of soft tissues in the stage of softening requires one of the following:
A. Local application of cold.
B. Extensive incision and drainage.
C. Puncture with subsequent bacteriologic culturing. D.Warm compression.
E. Injection of novocain and antibiotics.
Choose the correct answer.
6. A boil is due to staphylococcal infection of -
a) Hair follicle
b) Sweat gland
c) Subcutaneous tissue
d) Epidermis
7. A carbuncle is treated by -
a) Incision and drainage
b) Cruciate incision and deroofing
c) Antibiotics alone
d) Wide excision
8. Cellulitis is infection of -
a) Hair follicles
b) Subcutaneous spaces
c) Nail bed
d) Any of the above
9. Treatment of spreading streptococcocal cellulitis is-
a) Erythromycin
b) Penicillin
c) Tetracycline
d) Chloramphenicol
10. Following is true about erysipelas except –
a) Streptococcal infection
b) Contagious and infectious
c) Margins are raised
d) Common in tropics
11. Erysipelas is caused by -
a) Staph aureus
b) Staph albus
c) Strep pyogenes
d) Hemophilus
12. Commonest cause of cellulitis is
a) Staphylococcus
b) Streptococcus
c) E. coli
d) Hemophilus
13. Which is not true of carbuncle -
a) Infective gangrene of subcutaneous tissue
b) Caused by staphylococcus
c) Diabetics are more prone
d) Caused by streptococcus
e) Pencillin and excision of necrotic tissue treatment of choice
ANSWERS:
1 - A
2 - B
3 - A
4 - C
5 -B
6 - A
7 - A, D
8 - B
9 - B
10 - B, D
11 - C
12 - B
13 - B
References
Gostischev V. K. General surgery / The manual. – M.: GEOTAR-MED, 2003. – Charter XI. – P.150-191.
Moukonin A.A., Golub A.V. Soft tissue infection: Textbook for foreign students. – Smolensk: Smolensk State Medical Academy, General Surgery Department. – 2005. – 9p.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
INFLAMMATORY DISEASES OF FINGERS. ACUTE AND CHRONIC OSTEOMYELITIS (classification, clinical features, diagnostics, treatment)
Составитель: доцент Ю.И.Ломаченко
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
Paronychia
Infection of the area of the lateral nail fold typically is due to superficial trauma (e.g., hangnails, nail biting, manicuring, dishwashing). Paronychia in children often is the result of finger sucking. Although typically starting as a cellulitis, progression to abscess formation is not uncommon. Infection that spreads to the proximal nail edge is termed an eponychia.
Felon
The distal palmar phalanx is compartmentalized by tangentially oriented fibrous septa. These septa result in a closed compartment at the distal phalanx, which helps prevent the proximal spread of infection. Infection typically is due to direct inoculation of bacteria by penetrating trauma but may be caused by hematogenous spread and by local spread from an untreated paronychia.
Infection results in edema and increased pressure within the closed compartment. This, in turn, can impair venous outflow and lead to a local compartment syndrome and myonecrosis. Invasion of the bone leads to osteomyelitis.
Infectious tenosynovitis
Tendon sheathis consist of a visceral layer adherent to the tendon and a parietal layer. Notably, the flexor tendon sheath of the thumb is continuous with the radial bursae, while the flexor tendon sheath of the fifth digit is continuous with the ulnar bursae. In 80% of individuals, communication exists between the radial and ulnar bursae. The tenosynovial coverings of the second, third, and fourth digits do not communicate with either the radial or ulnar bursae in most individuals. Infection within a tendon sheath, as in other infections of the hand, usually is the result of direct inoculation of bacteria from penetrating trauma.
A common cause of penetrating trauma occurs when one person strikes another in the mouth, resulting in a fight bite. With the hand clenched in a fist, laceration of the skin on the dorsum of the hand by a tooth may involve the tendon sheath or tendon, surrounding soft tissue, and underlying bone.
Infection also can occur by hematogenous spread, with Neisseria gonorrhoeae the offending agent in many cases. Infection typically follows the course of the tendon sheath, which results in spread of infection into the radial or ulnar bursae, depending on the primary tendon sheath involved. Elevated pressure within the tendon sheath due to infection may impair nutrient flow to the tendon. Tendon necrosis and/or impaired function are disastrous sequelae of untreated elevated tendon sheath pressure.
Deep fascial space infection
The deep fascial spaces of the hand are potential spaces and consist of the dorsal subaponeurotic space, subfascial web space, midpalmar space, and thenar space. The dorsal subaponeurotic space lies dorsal to the extensor tendons of the hand. The subfascial web space is contiguous with the dorsal subcutaneous space of the digits. The midpalmar space is demarcated by the palmar interosseous muscles dorsally and the flexor tendons of the third, fourth, and fifth digits ventrally. Lastly, the thenar space consists of the area between the adductor pollicis muscle dorsally and the flexor tendon of the second digit ventrally.
These compartments are susceptible to infection by direct penetrating trauma, spread from a neighboring compartment, or hematogenous seeding. Due to the dorsal location of the hand lymphatics, erythema and swelling commonly appear over the dorsum of the hand, even when the injury is of palmar origin.
Mortality/Morbidity: Infections of the hand (especially dominant hand infections) can be devastating and frequently require admission for antibiotic therapy and/or surgical intervention.
History:
Paronychia
Recent trauma to lateral nail fold
History of nail biting, manicuring, or dishwashing
In children, history of finger sucking
Erythema and pain in early stages, followed by frank abscess formation with increased pain
May relate history of spontaneous drainage of pus
Felon
Recent trauma to finger pad
Pain, typically throbbing in nature
Swelling, pressure, and erythema
Presence and/or progression from paronychia
Infectious tenosynovitis
Recent penetrating trauma to hand
Gonococcal infection, particularly disseminated infection
Pain, especially with passive extension of finger
Edema of entire finger
Variable history of fever
Deep fascial space infection
Recent penetrating trauma to hand
Recent or untreated tenosynovitis
Palmar blister (may result in subfascial web space abscess)
Pain and edema of hand
Pain with movement of fingers
Variable history of fever
Physical:
Paronychia
Edema, erythema, and pain along lateral edge of nail fold
May have extension to proximal nail edge (eponychium)
Frank abscess formation possible
Felon
Painful, tense, and erythematous finger pad
Pointing of abscess possibly present
Signs typically limited to area distal to the distal interphalangeal joint due to
anatomic constraints
Evidence of penetrating trauma
Infectious tenosynovitis
The 4 cardinal signs, include the following:
Tenderness along the course of the flexor tendon
Symmetric edema of involved finger
Pain on passive extension (believed by some authors to be the most important sign)
Flexed resting posture of finger
All 4 signs possibly not present early in the course of infection
May have associated lymphangitis, lymphadenopathy, and fever
Deep fascial space infections:
All possibly presenting with lymphangitis (identified dorsally), lymphadenopathy, and fever
Dorsal subaponeurotic abscesses: Result in swelling and pain on the dorsum of the hand and pain with passive movement of the extensor tendons (difficult to distinguish from dorsal subcutaneous infection)
Subfascial web space infections: Present with pain and swelling on the dorsum and palmar surfaces of the hand (because the subfascial space is contiguous with the dorsal subcutaneous space, tracking of infection from the former to the latter results in a collar button abscess named for its hourglass shape)
Midpalmar space infections: Present with pain, swelling, loss of palmar concavity, pain with movement of the third and fourth digits, and dorsal swelling secondary to the tracking of infection dorsally along the lymphatics
Thenar space infections: Result in marked swelling of the thumb-index web space, flexed and abducted resting posture of the thumb, and pain with passive adduction
Causes:
Paronychia
Staphylococcus aureus and Streptococcus species are most common in acute cases.
Atypical mycobacteria and fungi may be offending agents in chronic cases and in patients who are immunocompromised.
Anaerobes may be involved in the pediatric population due to finger sucking.
Felon: S. aureus is the most common causative organism, but gram-negative organisms have been identified.
Infectious tenosynovitis
S. aureus and Streptococcus species commonly are isolated; however, some authors feel that N. gonorrhoeae should be considered a possible pathogen until excluded by culture data.
Eikenella corrodens is observed in infections caused by human bites.
Pasteurella muttocida and Capnocytophaga infections caused by cat and dog bites can progress rapidly to septic shock and death.
Deep fascial space infections
S. aureus and Streptococcus species are isolated most commonly.
Organisms mentioned for infectious tenosynovitis also apply to deep space infections. This may be the result of local spread from infected neighboring tendon sheaths.
Lab Studies:
Paronychia and felons: These often require no laboratory tests since the diagnosis is made clinically.
Infectious tenosynovitis and/or deep fascial space infections
As the infected spaces are drained and d6brided in the operating room, preoperative lab tests often are requested by the hand surgeons, but the diagnosis is made clinically.
Cultures are obtained in the operating room.
Imaging Studies:
X-rays
Since trauma often is a contributing factor in most hand infections, plain films are useful in excluding fractures and retained foreign bodies, if radiopaque.
Х-rays help identify subcutaneous or subfascial gas formation, if present.
X-rays may indicate osteomyelitis.
Emergency Department Care:
Paronychia
If no frank abscess or fluctaance is noted along the lateral nail edge, frequent hot soaks and a short course of antibiotics may result in resolution of the infection. If pus is present, perform incision of the area.
Perform a digital nerve block using lidocaine without epinephrine.
Using a scalpel blade or an needle, elevate the lateral nail fold at the site of the abscess to allow for drainage of pus.
As with any abscess, incision and drainage is the cornerstone of therapy for felons. A small wick is left in the incision to allow for continued drainage.
If pus has tracked beneath the nail, remove an adjacent longitudinal section of the nail to promote drainage.
Removal of the entire nail plate typically is not indicated unless the subungual abscess results in a floating nail.
After drainage and wick placement, dress the finger appropriately.
Update tetanus booster status as needed.
Felon
If frank abscess formation is present or the finger pad is tense, incision and drainage is indicated.
Incision and drainage is similar to that for a paronychia. This should not be undertaken lightly, since improper placement of the incision can lead to scarring, sensory loss, unnecessary pain, instability of the finger pad, and spread of infection into the adjacent tendon sheath.
Although many approaches have been described, such as the fish-mouth or hockey stick incisions, most authors recommend a digital nerve block as initial treatment followed by a longitudinal incision over the area of greatest fluctuance.
To avoid penetration of the tendon sheath, the incision should not extend to the distal interphalangeal crease.
Using a hemostat, bluntly dissect the wound to promote drainage.
Irrigate the cavity copiously and loosely pack with a gauze wick.
After irrigation and loose packing of the wound, apply a dry gauze dressing and overlying splint.
Update tetanus booster status as needed.
Infectious tenosynovitis and/or deep fascial space infections: ED care consists of making the correct diagnosis, providing pain relief, initiating antibiotic therapy, elevating and immobilizing the hand, and promptly consulting an experienced hand surgeon for definitive treatment. Experienced surgeons in the operating room should perform the incision and drainage.
Consultations:
Prompt consultation with an experienced hand surgeon is indicated for patients with evidence of infectious tenosynovitis, deep fascial space infections, or osteomyelitis.
Pharmacotherapy:
Antibiotics
The goals of therapy are to eradicate the infection and prevent complications. Antibacterial therapy must cover all likely pathogens in the context of the clinical setting. First-generation cephalosporins, lincosamides, combinations of aminopeniciliins with beta-lactamase inhibitor are considered. Vancomicin - potent antibiotic directed against gram-positive organisms and active against Enterococcus species. Useful in treatment of septicemia and skin structure infections. Indicated for patients who cannot receive or have failed to respond to penicillins and cephalosporins or for those who have infections with resistant staphylococci (MRSA),
Antitoxin (toxoid) is used to induce and boost active immunity.
Tetanus toxoid - Used to induce active immunity against tetanus in selected patients. Immunizing agents of choice for most adults and children >7 у are tetanus and diphtheria toxoids. Necessary to administer booster doses to maintain tetanus immunity throughout life.
Do not use toxoid to treat actual tetanus infections or for immediate prophylaxis of unimmunized individuals (use instead tetanus antitoxin, preferably human tetanus immune globulin)!
Further Inpatient Care:
Patients with evidence of infectious tenosynovitis or deep fascial space infections require inpatient treatment consisting of parenteral antibiotics and definitive incision and drainage by an experienced hand surgeon.
Inpatient splinting and occupational therapy for range of motion is essential to preserve function.
Further Outpatient Care:
Paronychia
Instruct the patient to soak the affected finger 3-5 times per day in warm water.
If a wick was placed, the patient usually can remove it easily after 24 hours if it has not fallen out already.
Schedule follow-up care with the primary care doctor or at the ED for 48 hours after initial incision.
Antibiotics, if prescribed, should be continued for 3-5 days.
Felon
Reevaluate the wound 48 hours after initial incision.
At this time, remove the packing and irrigate the wound.
If continued drainage is present, loosely repack the wound and schedule another follow-up appointment in 24 hours.
If no further drainage is present, repacking is unnecessary.
Instruct the patient to keep the wound clean by washing it twice daily with warm, soapy water followed by a clean gauze dressing.
Continue antibiotics for 5-7 days.
Complications:
Paronychia
Subungual abscess
Osteomyelitis of the distal phalanx
Development of a felon
Chronic infection
Paronychia
Most resolve in 2-4 days.
Chronic infections are likely fungal infections.
Felon
Osteomyelitis of the distal phalanx
Skin pulp necrosis
Sinus tract formation
Septic joint
Tenosynovitis
Inappropriate incision and drainage technique, resulting in sensory loss, tendon injury, spread of infection, or instability of the finger pad
Infectious tenosynovitis
Tendon destruction
Functional disability
Extension of infection to deep fascial space
Deep fascial space infection
Functional disability
Tendon destruction
Sepsis
Hand loss
Prognosis:
Paronychia
Most resolve in 2-4 days.
Chronic infections are likely fungal infections.
Felon: The prognosis is good, with healing in 1-2 weeks.
Infectious tenosynovitis and/or deep fascial space infection: These have a fair prognosis, depending on the extent of tissue destruction, bony involvement, preexisting vascular insufficiency, and systemic complications (e.g., bacteremia, sepsis).
OSTEOMYELITIS
SHORT-CUT of pathogenesis of hematogenous osteomyelitis
In classical hematogenous osteomyelitis of childhood, organisms in bloodstream gain access to bone by way of the nutrient artery and pass through branches of this vessel to the metaphysis;
- terminal vessels enter small, bone-lined channels on metaphyseal side of the epiphyseal plate;
- these channels have a blind end, and each terminates in the last hypertrophic cartilage cell of epiphyseal plate;
- on reaching the end of the tunnel, capillary inside this channel must turn 180 deg and exit through the same passage by which it entered;
- it is in this area of sluggish circulation, in tunnels whose walls are essentially impermeable, that bacteria lodge and hematogenous osteomyelitis begins;
- once the process starts, thrombosis of small terminal vessel and exudate seal the entrance to channel;
- in depths of this bone tunnel the organisms begin to proliferate.unimpeded by the host defenses that are unable to reach them;
- after the infection is established in one channel, it extends into metaphysis and involves other channels;
- hordes of PMNs are mobilized in metaphysis, and cellular destruction occurs at a rapid rate;
- in adolescents, infection usually begins in metaphysis because of tendency for sluggish & turbulent blood flow in capillary-sinusoid loops adjacent to growth plate & absent or nonfunctioning phagocytes;
- bacteria that localize to this area proliferate and easily obstruct blood flow, resulting in infarction and creation of environment conducive to further bacterial proliferation;
- pus in the metaphysial area expands under pressure and travels up the marrow cavity or passes out of the cortex through the many small metaphyseal openings;
- in certain areas such as the hip, where epiphyseal plate is situated w/in joint capsule, early joint involvement by infection is common;
- at knee, the joint is usually spared, and infections beginning in the distal femoral or proximal tibial metaphysis usually spread along shaft of the bone moving away from the joint;
- stripping of the periosteum from the shaft by pus stimulates intense osteoblastic response;
- new immature bone is formed as response to periostea) stripping, and, in severe cases, the entire shaft may be encased in a sheath of new bone referred to as an involucrum;
- where a major portion of the shaft has been deprived of blood supply, resulting sequestrum lies within the involucrum;
- openings in the involucrum, called cloacae, may permit escape of pus from bone may be fulminant, w/ overwhelming sepsis & death;
- septicemia can cause bacterial seeding to other bones, leading to multiple sites of osteomyelitis;
- if disease is treated early w/ appropriate antibiotics, septicemia is controlled, and there may be only limited bone damage.
Osteomyelitis is a difficult-to-treat infection of bone and bone marrow, it is progressive and results in inflammatory destruction of the bone, bone necrosis, and new bone formation. Bacterial osteomyelitis causes substantial morbidity worldwide, despite continued progress toward understanding its pathophysiology and optimal management.
The approach to osteomyelitis depends upon the route by which bacteria gained access to bone, bacterial virulence, local and systemic host immune factors, and patient age. While imaging studies and nonspecific blood tests may suggest the diagnosis, an invasive technique is generally required to identify the causative pathogens. Antibacterial regimen selection has been largely guided by knowledge of the relative activities and pharmacokinetics of individual drugs, supported by data from animal models.
Definitive therapy often requires a combined medical and surgical approach. Newer microvascular and distraction osteogenesis techniques and the use of laser Doppler allow more complete surgical resection of infected material while maintaining function. Despite recent advances, aggressive medical and surgical therapy fails in many patients with osteomyelitis. More accurate diagnostic methods, better ways to assess and monitor the effectiveness of therapy, and novel approaches to eradicate sequestered bacteria are needed.
History of the Procedure: Osteomyelitis has been well known since antiquity.
Problem: Osteomyelitis results in inflammatory destruction of the bone, bone necrosis, and new bone formation. Three major categories of osteomyelitis exist, based upon pathogenic mechanisms of infection, as follows:
• Osteomyelitis following hematogenous spread of infection
• Osteomyelitis secondary to a contiguous focus of infection
• Osteomyelitis associated with vascular insufficiency
Three different subtypes of osteomyelitis are known: acute osteomyelitis, subacute osteomyelitis, and chronic osteomyelitis.
Frequency: The overall prevalence of acute osteomyelitis is 2 cases per 10,000 children. Neonatal prevalence is approximately 1 case per 1000 children. The annual incidence in patients with sickle cell anemia is approximately 0.36%.
The prevalence of osteomyelitis after foot puncture may be as high as 16% (30-40% in patients with diabetes).
Excluding the axial skeleton, lower extremity osteomyelitis accounts for 90% of osteomyelitis cases and is much more common than upper extremity osteomyelitis, which accounts for 10% of extremity cases.
The most common bones involved in osteomyelitis in descending order are as follows:
Tibia (50%)
Femur (30%)
Fibula (12%)
Humerus (3%)
Ulna (3%)
Radius (2%)
The prevalence of chronic osteomyelitis is 2 cases per 10,000 people.
Most studies support the idea that incidence is similar in developed countries. In
developing countries, incidence is higher due to higher incidence of puncture wounds, contaminated injuries, and less wound care.
Epidemiology of vertebral osteomyelitis
It is primarily a disease of adults; the majority of patients are older than 50 years. As a general rule, the incidence increases progressively with each successive decade of life. Men are affected approximately twice as often as women in most case series; the reason for this male predominance is not clearly understood.
It is difficult to obtain reliable information of the overall incidence of vertebral osteomyelitis. However, most authorities believe that the overall incidence of vertebral osteomyelitis has steadily increased in recent years for 3 primary reasons: increasing rates of nosocomial bacteremia due to intravascular devices and other forms of instrumentation, increasing age of the population, and increasing injection drug use.
Etiology: While normal bone is resistant to infection, a number of conditions can
predispose one to development of osteomyelitis, including the following:
Large inoculation of an organism
Trauma leading to bone damage or infarction.
Presence of a foreign body
Illnesses compromising host defense
A single pathogenic organism is almost always recovered from the bone. The most common bone isolates are Staphylococcus species, the most common gram-negative organism is Pseudomonas aeruginosa, and the most common anaerobe is Peptostreptococcus species. However, in immunocompromised patients, other organisms, including fungi and mycobacteria, also must be considered. Commonly isolated organisms in osteomyelitis can be summarized as follows:
Hematogenous osteomyelitis (monomicrobial infection)
Infants (<1 y)
Group В Streptococcus
Staphylococcus aureus
Escherichia coli
Children (aged 1-16 у)
S. aureus
Streptococcus pyogenes
Haemophilus influenzas
Adults (> 16 у)
S. aureus
Coagulase-negative Staphylococcus species
Gram-negative bacilli
Paeruginosa
Serratia marcescens
Contiguous focus osteomyelitis (polymicrobial infection)
S. aureus
Coagulase-negative Staphylococcus species
Spyogenes
Enterococcus species
Gram-negative bacilli
Anaerobes
Diabetic foot osteomyelitis (polymicrobial Infection)
S. aureus
Streptococcus species
Enterococcus species
Proteus mirabilis
Р.aeruginosa
Anaerobes
Pathophysiology: The pathogenesis of osteomyelitis is multifactorial and poorly understood. Some important factors include the following:
Virulence determinants of the organisms
Underlying disease and the immune status of the host
Type and location of the bone
It is clear that bacterial cells adhere to nucleated cells, platelets, and a variety of components of the extracellular bone matrix collagen and noncollagenous proteins.
Cellular and molecular pathogenesis
Cellular and molecular techniques provide new methods for determining the relative importance of the many potential virulence factors by facilitating study of the interaction between the host immune response and potential bacterial virulence factors. As an example, S aureus, which is an important cause of both hematogenous and contiguous focus osteomyelitis, produces a large number of extracellular and cell-associated factors that may contribute to virulence, including the following:
• Bacterial adherence: Bacteria adhere to bone by expressing receptors for the components of bone matrix including fibronectin, laminin, collagen, and bone sialoglycoprotein. Adherence appears to play a central role in the early stages of S. aureus-induced osteomyelitis or arthritis. Expression of adhesins permits attachment of the pathogen to cartilage and synovial membrane. Strains positive for collagen adhesin are also associated with the production of high levels of immunoglobulin G(IgG) and interleukin (IL)-6. Bone infection has been speculated to possibly be prevented by an adhesin-derived vaccine.
• Proteolytic activity: Potential proteolytic activity present in normal joints is inhibited in the absence of infection. However, this protective effect may be lost with infection. In an in vitro model of adult chondrocytes inoculated with S. aureus, for example, overall protein synthesis was reduced by 84%, with an increase in the release of collagenase and gelatinase.
• Resistance to host defense mechanisms: The ability of microorganisms to resist host defense mechanisms at both the cellular and matrix levels presents difficulties in the treatment of osteomyelitis. S aureus can survive intracellularly in cultured osteoblasts. Furthermore, the presence of arachidonic acid metabolites such as prostaglandin E2, which is a strong osteoclast agonist, decreases the bacterial inoculum needed to produce infection. Once the microorganisms adhere to bone, they express phenotypic changes that make them resistant to antimicrobial treatment.
S. aureus organisms express a 42-kd protein, protein A, which is bound covalently to the outer peptidoglycan layer of their cell walls. Protein A binds to the Fc portion of IgG on polymorphonuclear leukocytes, interfering with opsonization and phagocytosis of S aureus. This interference has been demonstrated in vitro and in animal models of subcutaneous abscess and peritonitis.
S. aureus also secretes 2 toxins, exotoxin and toxic shock syndrome toxin (TSST)-1, which exert a profound effect on the immune system when administered parenterally. The toxins act as superantigens and suppress plasma cell differentiation. They also stimulate production of cytokines, such as IL-1, interferon-gamma, and tumor necrosis factor (TNF)-a. Animals infected with strains of S aureus isogenic for TSST-1 developed frequent and severe arthritis. Staphylococcal enterotoxin and TSST-1 subvert the cellular and humoral immune system, which may determine whether a local infection is eliminated or develops into osteomyelitis or septic arthritis.
• Nitric oxide: The increased turnover of bone in osteomyelitis suggests that the balance between bone formation and resorption is altered, an effect that may be mediated by nitric oxide. Greatly increased levels of nitric oxide and bone resorption have been recorded in the septic skeleton. This response may be driven by the increased levels of cytokines, enterotoxin, and TSST-1, which may stimulate nitric oxide production by endothelial, macrophage, and mesenchymal cells such as osteoblasts. Thus, while low concentrations of nitric oxide are typically thought to inhibit osteoclastic bone resorption, this response may be lost when cytokine and nitric oxide levels increase greatly in skeletal inflammatory disease. Adjunctive local treatment of osteomyelitis with nitric oxide synthetase inhibitors could be beneficial.
Routes of infection
As noted above, osteomyelitis develops via 3 major routes: hematogenous, contiguous focus spread, and vascular insufficiency.
• Hematogenous osteomyelitis: Hematogenous osteomyelitis is predominantly encountered in children; 85% of patients with hematogenous osteomyelitis are younger than 17 years, accounting for 20% percent of the total cases of osteomyelitis. In one study of 659 cases of S aureus osteomyelitis occurring in Denmark from 1959-1988, the number of hematogenous osteomyelitis cases declined, especially in children, and cases of vertebral osteomyelitis, more common in adults, increased. In children, the bone infection usually affects the long bones, while in adults, the lesion is usually located in the thoracic or lumbar vertebrae.
• Contiguous focus osteomyelitis without generalized vascular insufficiency: Osteomyelitis secondary to contiguous foci of infection accounts for at least one half of all cases and has increased in incidence. The organisms may be directly inoculated into the bone at the time of trauma, spread by nosocomial contamination during perioperative or intraoperative procedures, or extend from an adjacent soft tissue infection.
• Contiguous focus osteomyelitis with generalized vascular insufficiency: The primary cause of vascular insufficiency in patients with osteomyelitis is diabetes mellitus. The small bones of the feet, talus, calcaneus and distal fibula, and tibia are commonly involved. The patients in this group are aged 35-70 years. The infection frequently is initiated by a portal of entry for organisms, such as infected nail beds, cellulitis, or atrophic skin ulceration.
Diminished arterial blood supply has traditionally been considered to be the major predisposing factor for contiguous focus osteomyelitis with generalized vascular insufficiency in patients with diabetic foot. However, neuropathy now appears to be an equally important factor. Identifiable neuropathy as a complication of diabetes mellitus is present in approximately 80% of patients with foot disease. Neuropathy can cause foot ulceration through 3 main mechanisms, as follows:
• Decreased sensation leads to mechanical or thermal injuries in the unaware patient that can develop into skin ulcerations.
• Motor neuropathy affecting the intrinsic muscles of the foot predisposes affected persons to gait disturbances and foot deformities, such as hammertoe - and clawtoe deformity and Charcot foot. These anatomic alterations can lead to a maldistribution of weight and elevated focal pressure over the bony prominences. Subsequently, the increase in pressure where the foot contacts the ground or rubs against shoes can lead to skin ulceration.
• Autonomic neuropathy interferes with sweating; the resultant dry, cracked skin allows entry of microorganisms into the soft tissue.
A higher rate of nasal and skin colonization with S aureus, defects in host immunity, and impaired wound healing are all important factors in diabetic foot infection. Superficial fungal skin infections, which are common in patients with diabetes, also can facilitate bacterial entry through macerated or broken skin. Pathological differences based on age
Basic differences exist in the pathology of osteomyelitis in infants, children, and adults. In infants, small capillaries cross the epiphyseal growth plate and permit extension of infection into the epiphysis and joint space. This is a newly well-understood condition referred to as septic osteomyelitis in infants. The cortical bone of neonates and infants is thin and loose, consisting predominantly of woven bone, which permits escape of the pressure caused by infection but promotes rapid spread of the infection directly into the subperiosteal region. A large sequestrum is not produced because extensive infarction of the cortex does not occur; however, a large subperiosteal abscess can form. In children older than 1 year, infection presumably starts in the metaphyseal sinusoidal veins and is contained by the growth plate. The joint is spared unless the metaphysis is intracapsular. The infection spreads laterally where it breaks through the cortex and lifts the loose periosteum to form a subperiosteal abscess.
In adults, the growth plate has resorbed, and the infection may again extend to the joint spaces, as in infants. In addition, the periosteum is firmly attached to the underlying bone; as a result, subperiosteal abscess formation and intense periosteal proliferation are observed less frequently. The infection can erode through the periosteum, forming a draining sinus tract.
STAGING
Cierny-Mader classification
The Cierny-Mader system is a good model for the diagnosis and treatment of long bone osteomyelitis, since it permits stratification of infection and the development of comprehensive treatment guidelines for each stage.
The Cierny-Mader classification is based upon the anatomy of the bone infection and the physiology of the host. The stages are dynamic and may be altered by therapy outcome or change in host status. The classification is determined by the condition of the disease process itself, regardless of its etiology, region, or chronicity. The anatomic types of osteomyelitis are medullary, superficial, localized, and diffuse.
Stage 1, or medullary osteomyelitis, denotes infection confined to the intramedullary surfaces of the bone. Hematogenous osteomyelitis and infected intramedullary rods are examples of this anatomic type.
Stage 2, or superficial osteomyelitis, is a true contiguous focus infection of bone; it occurs when an exposed infected necrotic surface of bone lies at the base of a soft tissue wound.
Stage 3, or localized osteomyelitis, usually is characterized by a full-thickness cortical sequestration that can be removed surgically without compromising bony stability.
Stage 4 or diffuse osteomyelitis is a through-and-through process that usually requires an intercalary resection of the bone to arrest the disease process. Diffuse osteomyelitis includes those infections with a loss of bony stability either before or after debridement surgery.
CLINICAL PICTURE
Clinical: The clinical presentation and location of osteomyelitis differ in infants, children, and adults. In infants, medullary infection may spread to the epiphysis and joint surfaces through capillaries that cross the growth plate. In contrast, in children older than 1 year, the growth plate is avascular and infection is confined to the metaphysis and diaphysis. The joint is spared unless the metaphysis is intracapsular. Thus, cortical perforation at the proximal radius, humerus, or femur enables the infection to migrate to the elbow, shoulder, or hip joint, respectively, regardless of the age of the patient.
Hematogenous osteomyelitis
In hematogenous osteomyelitis, local symptoms referable to bones are more frequently absent in neonates than in children. In adults, soft tissue findings may be more prominent than bony involvement.
In infants, local findings that may lead the clinician to suspect osteomyelitis are usually absent in neonates. When they develop, local findings can include decreased motion of a limb and edema (pseudoparalysis) and joint effusion adjacent to the bone infection (present in 60-70% of cases).
Systemic symptoms are frequently present in S. aureus osteomyelitis but may be absent when other pathogens are involved.
Children with hematogenous osteomyelitis, in contrast with neonates, typically have the following systemic symptoms:
Abrupt fever
Irritability
Lethargy
Refusal to use the affected limb
Local signs of inflammation present for 3 weeks or less
While this is the classic presentation, signs of systemic toxicity other than minimal temperature elevation are absent in 50% of children with osteomyelitis.
In adults, acute clinical presentations of fever, chills, swelling, and erythema over the involved bones are usually seen in acute hematogenous osteomyelitis.
Vertebral osteomyelitis is usually hematogenous in origin but may be secondary to trauma. A preceding history of urinary tract infection or injection drug use often is present. Other sources of infection include skin and soft tissue, respiratory tract, infected intravascular device site, endocarditis, dental infection, or unknown sources.
The patient usually presents with vague symptoms and signs consisting of dull, constant back pain and spasm of the paravertebral muscles. Localized pain and tenderness of the involved bone segments is present in at least 90 percent of cases. The pain is usually insidious and slowly progresses over 3 weeks to 3 months.
Contiguous focus osteomyelitis without vascular compromise
Common predisposing factors for contiguous focus osteomyelitis include surgical reduction and internal fixation of a fracture, open fractures, and chronic soft tissue infections. This form of osteomyelitis is biphasic in its age distribution. The infection occurs in younger persons secondary to trauma and related surgery and in older adults from decubitus ulcers.
The infection usually manifests within 1 month after inoculation of the organisms from trauma, surgery, or a soft tissue infection. Affected patients typically present with low-grade fever, pain, and drainage. Loss of bone stability, bone necrosis, and soft tissue damage frequently occur, making this form of osteomyelitis difficult to treat.
Contiguous focus osteomyelitis with vascular compromise
Osteomyelitis in patients with vascular compromise, who are often diabetic, can be difficult to diagnose. Patients can present with an apparently localized process including an ingrown toenail, a perforating foot ulcer, cellulitis, or a deep space infection. Concurrent peripheral neuropathy often alters the patient's perception of pain. Fever and systemic toxicity are frequently absent.
Physical examination commonly reveals diminished dorsal pedis and posterior tibia pulses, poor capillary refill, and decreased sensation.
Chronic osteomyelitis
The hallmark of chronic osteomyelitis is the presence of dead bone (the sequestrum). Involucrum (reactive bony encasement of the sequestrum), local bone loss, persistent drainage, and/or sinus tracts are other common features of chronic disease.
The patient with chronic osteomyelitis commonly presents with chronic pain and sinus formation with purulent drainage. Fever is usually low grade or absent. The chronic infection usually does not progress or does so slowly. If a sinus tract becomes obstructed, the patient can present with a localized abscess and/or soft tissue infection.
Prospects of halting the infection are reduced when the integrity of surrounding soft tissue is poor or the bone is unstable due to an infected nonunion or an adjacent septic joint. Squamous cell carcinoma at the site of tissue drainage and amyloidosis are rare complications of chronic osteomyelitis.
INDICATIONS for surgical intervention
Successful management of osteomyelitis requires aggressive pursuit of the diagnosis and early antimicrobial and surgical therapy. If acute osteomyelitis is not treated optimally, the risk is high of developing chronic osteomyelitis, which is significantly less amenable to treatment.
Staging and classification systems may be used in determining appropriate treatment for osteomyelitis.
Surgical intervention is indicated in the following situations:
The patient has not responded to specific antimicrobial therapy within 48 hours.
Evidence exists of a persistent soft tissue abscess.
Concomitant joint infection is suspected or diagnosed.
In adults with hematogenous osteomyelitis, a thorough intramedullary reaming and unroofing is usually performed with or without bone grafting. Soft tissues are reapproximated, and the limb is protected by external means (brace or cast) until the structural integrity of the bone is reestablished by normal remodeling.
Contraindications: Contraindications to debridement of infected bone are limited and include the following:
In acute osteomyelitis in infants, the infection usually responds well to medical therapy alone. Surgery should be reserved for nonresponsive cases.
Suspicion of malignancy or presence of secondary bone infection with malignancy should not be treated with debridement alone. Tumor workup and biopsy should be performed first. If infection cannot be eradicated or tumor is not resectable, amputation is indicated.
Massive debridement is not recommended in the presence of sickle cell disease; usually a mixture of infection and avascular necrosis is present that may improve after good reperfusion. Massive debridement may produce very large defects that may not be easily amenable to reconstruction surgeries.
The use of a tourniquet is not recommended by many authors due to the acute bacteremic phase after the tourniquet is released and toxemia.
Local anesthesia is generally ineffective and should be avoided due to the change in the local PH of the tissue that prevents the metabolism of the local anesthetics to the active ingredients.
The general condition of the patient should not be considered a contraindication to urgent surgery. Delaying surgery may lead to further deterioration.
CLINICAL RECOGNIZING
Lab Studies:
Routine laboratory test findings are usually nonspecific. These include CBC, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), renal and hepatic profile, and bone profile.
Complete blood count: Leukocytosis is common in acute osteomyelitis but not in chronic osteomyelitis.
Erythrocyte sedimentation rate
The ESR is usually elevated but may be in the reference range. In a patient with a high ESR initially, monitoring the ESR may be useful in detecting a relapse. In patients with a foot ulcer and diabetes mellitus, an ESR greater than 100 mm/h is highly specific but insensitive for a diagnosis of osteomyelitis.
Although ESR is associated with low sensitivity and specificity, it is widely employed. In the patient without a prior history of osteomyelitis, the ESR is most helpful when infection is unlikely. For example, in patients with low-back pain but without historical clues to suggest vertebral osteomyelitis (eg, recent urinary tract infection), a normal ESR is a reassuring finding. Conversely, an elevated ESR suggests the need for further evaluation.
C-reactive protein
CRP, like ESR, is an acute-phase reactant. Although said to be more specific for infection than ESR, it is also relatively insensitive and nonspecific.
The primary difference between these tests is that the CRP has a shorter half-life than the ESR. Measuring in vitro clumping of venous leukocytes (leukergy) may more closely correlate with severity of infection than the ESR.
Renal and hepatic profile: Whether leukergy, which reflects altered surface expression of leukocyte adhesion molecules, will be useful for managing osteomyelitis is not known. This test is not routinely available.
Efforts have been made to develop serologic assays to diagnose osteomyelitis caused by S aureus. Patients with osteomyelitis mount a vigorous antibody response, but the utility of detecting antibodies to cell wall components such as peptidoglycan or teichoic acid has been limited by the presence of such antibodies in uninfected, healthy persons. In a preliminary study, serum antibodies to S aureus exoproteins differentiated 3 cases of S aureus osteomyelitis from 4 cases caused by other organisms. Another limitation of serology is that it is unlikely to be developed for nonstaphylococcal disease. However, highly specific assays for staphylococcal osteomyelitis would be very useful. At present, serology cannot be recommended clinically, and such tests are available only for research purposes.
Blood culture results are positive in 50% percent of cases of acute osteomyelitis. A positive blood culture result in a patient with radiological findings consistent with osteomyelitis obviates the need for biopsy to obtain the specific microbiologic diagnosis.
Imaging Studies:
Plain films: Plain radiographs are relatively inexpensive, may be used to make the diagnosis, help in interpreting and choosing other studies, and allow one to exclude other conditions (eg, gas in the soft tissues). In uncomplicated acute infection, the triad of soft tissue swelling, bone destruction, and periosteal reaction is fairly specific for osteomyelitis and is sufficient to warrant a course of therapy (empiric until the microbiologic diagnosis has been established).
Plain films are generally insensitive for the diagnosis of acute osteomyelitis. This is in part due to the 2-3 weeks required for bone changes to be evident on plain films, although changes may be seen at this time on the other imaging modalities. Furthermore, in complicated situations, bone changes may not be distinguishable from those due to another process, such as a Charcot joint, fractures, or cancer. Thus, the diagnosis of acute osteomyelitis cannot be excluded if the plain film findings are negative. Further testing should be performed because early therapy is essential to reduce the formation of necrotic bone and the development of chronic osteomyelitis.
The primary findings are different in chronic osteomyelitis, which is characterized by bone sclerosis, periosteal new bone formation, and sequestra. It is difficult to distinguish active from inactive infection.
CT scan: This modality is used to evaluate an area in which focal findings are
present on examination and plain films findings are negative. The CT scan (with
and without contrast) is very accurate for detecting cortical destruction,
intraosseous gas, periosteal reaction, and soft tissue extension.
MRI: This study is an alternative to CT scan and is especially useful in evaluating a patient for osteomyelitis in the vertebrae and in the infected foot. In vertebral osteomyelitis, findings on T1-weighted images include decreased signal intensity in the disk and adjacent vertebral bodies and loss of endplate definition. Findings on T2-weighted images include increased signal intensity in the disk and adjacent vertebral bodies. With gadolinium, there is enhancement of the disk, adjacent vertebral bodies, and involved paraspinal and epidural soft tissue.
MRI provides useful anatomic detail in planning for surgical debridement, since it may show abscesses that need drainage, and can reduce the risk of operating on bland cellulitis. MRI also can be used to delineate soft tissue/epidural involvement and spinal cord impingement that cannot be seen on nuclear medicine images.
When evaluating the foot for osteomyelitis, MRI is as specific or more specific and more sensitive than technetium bone scan. In one series in which bone biopsy was used as the criterion standard, the sensitivity was 72% for MRI, 68% for bone scan, and 45% for indium white blood cell scan.
MRI cannot be used in patients with certain metal implants. In addition, false-positive results can occur with bone infarct or fracture or in healed osteomyelitis. Differentiating cancer from osteomyelitis may be difficult with MRI.
MRI for diabetic foot ulcers
The diagnosis of osteomyelitis in diabetic foot ulcers is often missed because of 2 major factors, most cases occur in ulcers not exposing bone and most have no evidence of inflammation on physical examination. In comparison, osteomyelitis was present in all patients in whom bone was exposed in one series.
MRI is the imaging procedure of choice for osteomyelitis in diabetic foot ulcers, being more accurate than the other modalities (95% versus 50-70% for plain films, bone scan, and indium scan in one series). Two clinical factors also may be useful in these patients, probing the ulcer and ulcer size.
Ultrasonography: Ultrasound findings consistent with osteomyelitis include fluid collection adjacent to the bone without intervening soft tissue, elevation of the periosteum by more than 2 mm, and thickening of the periosteum. Ultrasound also may improve the yield from fine needle biopsies.
Scintigraphy: Multiple different nuclear medicine imaging procedures are available to evaluate for osteomyelitis, including bone scan, indium-labeled leukocyte scan, and bone marrow scan.
Three-phase bone scan
The 3-phase bone scan uses technetium Tc 99m bound to phosphorus as the tracer, which accumulates in areas of increased osteoblast activity (reactive new bone formation and increased blood flow). The images obtained are immediate (flow), 15 minute (blood pooling), and 4 hour (bone imaging). The scan findings are different in cellulitis and osteomyelitis. Cellulitis results in increased activity in the first 2 phases and normal or diffusely increased activity in the third phase. In comparison, osteomyelitis results in intense uptake in all 3 phases.
The 3-phase technetium bone scan is the test of choice in evaluating for acute osteomyelitis if the plain film findings are normal. In this situation, it has an estimated sensitivity and specificity of almost 95% and findings generally are positive in 2-3 days of infection. However, any process that results in increased bone turnover appears as a hot spot that is indistinguishable from osteomyelitis. These false-positive findings can occur with posttraumatic injury, following surgery, diabetic feet, septic arthritis, noninfectious inflammatory bone disease, cancer, healed osteomyelitis, and Paget disease.
Indium-labeled leukocyte scan: Indium-labeled leukocyte scanning uses white blood cells labeled with radioactive indium as the tracer. It accumulates at sites of inflammation or infection and in the bone marrow. It is not specific for bone. Since it accumulates in marrow, it is less sensitive for imaging those areas with red marrow (eg, the axial skeleton). The indium scan also can be used for the diagnosis of osteomyelitis at sites of fracture nonunion. Two prospective studies found a sensitivity and specificity of 91% and 97%, respectively, in this setting. Indium scans have better sensitivity and specificity than bone scans in diabetic feet, but the specificity is poor, especially in the hindfoot.
Bone marrow scan: The bone marrow scan uses technetium Tc 99m-labeled sulfur colloid as the tracer. It is taken up by the reticuloendothelial system, including the bone marrow, spleen, and liver. It allows one to image the marrow instead of the bone. Its main use is in conjunction with the indium-tagged white blood cell scan to evaluate for suspected osteomyelitis in the axial skeleton, where the presence of marrow decreases the accuracy of the indium scan.
Gallium citrate scanning: Gallium citrate scanning uses radioactive gallium citrate as the tracer. It acts as an analog of calcium and iron and attaches to transferrin to accumulate at sites of inflammation. Gallium imaging is the most sensitive and specific radionuclide scanning technique for vertebral osteomyelitis. A typical positive test result reveals intense uptake in 2 adjacent vertebrae with loss of the intervening disk space. In one study of 41 patients with suspected vertebral osteomyelitis, increased gallium uptake was detected in all of the 39 patients with biopsy-proven osteomyelitis.
Dual tracer scans: Dual tracer examinations combine an inflammation imaging tracer (indium or gallium) with an "anatomic" tracer (either technetium bone scan or technetium sulfur colloid marrow scan), with images being collected either sequentially or simultaneously. Sequential studies combine the sensitivity of the bone scan (if findings are negative, no further imaging is done) with the specificity of the indium scan. Simultaneous studies combine the sensitivity and specificity of the indium scan and the bone scan to provide the anatomic detail needed to localize the infection to bone or soft tissue.
Other: Radiolabeled antigranulocyte antibodies are being investigated in an
attempt to find a more accurate tracer for localizing infection.
Other Tests:
Extended field of view ultrasound in musculoskeletal disorders: With the advent of high-resolution linear array transducers (7.5 MHz and 10 MHz), interest in musculoskeletal ultrasonography has continued to develop. Ultrasonography has been applied in the evaluation of infectious processes such as osteomyelitis, cellulitis, and subcutaneous abscesses. Extended field of view ultrasonography combines the convenience of a real-time scanner with the spatial advantages of a static B-mode scanner. Detailed examination of surfaces of cortical bone and cartilage has application in the evaluation of rheumatologic diseases for periarticular erosions, trauma for radiographically occult fractures, congenital hip dysplasia, and early osteomyelitis.
Diagnostic Procedures:
Bone biopsy: The criterion standard for the diagnosis of osteomyelitis is open bone biopsy with histopathologic examination and cultures. Histopathologic features indicating osteomyelitis include necrotic bone with extensive resorption adjacent to an inflammatory exudate. Needle biopsy is commonly used to obtain bone for histopathologic analysis. However, the incidence of sampling error is not negligible, with the sensitivity and specificity of this technique being 87% and 93%, respectively. Sensitivity of needle biopsy is particularly low in the postoperative or posttrauma patient.
If the clinical suspicion is strong and blood culture results and the needle biopsy findings are negative, the needle biopsy should be repeated or an open biopsy should be performed. In patients with compromised vasculature, a bone sample can be obtained at debridement for the histopathologic diagnosis of osteomyelitis.
Accurate cultures can be obtained only if the bone biopsy is performed through uninvolved tissue. In addition, cultures of the sinus tract are useful if S aureus and possibly Salmonella species are cultured. The presence of other common organisms does not predict those that will be found on bone biopsy.
Probing a diabetic foot ulcer
In a recent report, the detection of bone when probing a diabetic foot ulcer with a sterile probe was highly accurate in ruling in osteomyelitis. Seventy-five patients with 76 ulcers were studied, with the criterion standard for the diagnosis of osteomyelitis being histopathologic examination of bone resected at debridement. Contiguous osteomyelitis was present in 50 of the 76 ulcers. Of these, bone was palpable by probe in 33. The sensitivity and specificity were 66% and 85%, respectively, giving a positive predictive value of 89% and a negative predictive value of 56% in this population. These patients had a very high rate of osteomyelitis (61%); thus, the high positive predictive value is not likely to be applicable to ulcers with a lower risk of complicating osteomyelitis.
The size of a diabetic foot ulcer also may be helpful. In one series, osteomyelitis was present in 94% of ulcers greater than 2 cm2 in area. Thus, in a diabetic patient with a foot ulcer, either probing of bone or ulcer area above 2 cm2 is associated with about a 90% chance of having underlying osteomyelitis. Further noninvasive testing is unlikely to improve the accuracy of diagnosis.
Histologic Findings: Acute osteomyelitis presents as a suppurative infection with acute inflammatory cells, accompanied by edema, vascular congestion, and small vessel thrombosis. In early acute disease, the vascular supply to the bone is compromised by infection extending into the surrounding soft tissue. When both the medullary and periosteal blood supplies are compromised, large areas of dead bone (sequestra) may be formed. Within this necrotic and ischemic tissue, the bacteria can be difficult to eradicate even after an intense host response, antibiotic therapy, or both.
Pathologic features of chronic osteomyelitis include necrotic bone, the formation of new bone, and polymorphonuclear leukocyte exudation joined by large numbers of lymphocytes, histiocytes, and occasional plasma cells.
Host defense and mesenchymal cells, mainly the polymorphonuclear leukocytes, macrophages, and the osteoclasts, release proteolytic enzymes that break down organic elements in the dead bone. Because of lost blood supply, dead bone appears whiter than living bone. Cancellous bone is absorbed rapidly and may be completely sequestrated or destroyed in 2-3 weeks, but necrotic cortex may require 2 weeks to 6 months for separation. After complete separation, the dead bone is slowly eroded by granulation tissue and absorbed.
New bone formation is another characteristic feature of osteomyelitis. New bone forms from the surviving fragments of periosteum, endosteum, and the cortex in the region of the infection and is produced by a vascular reaction to the infection. New bone may be formed along the intact periosteal and endosteal surfaces and also may arise when the periosteum forms an encasing sheath of live bone (involucrum) surrounding the dead bone. Involucrum is irregular and is often perforated by openings through which pus may track into the surrounding soft tissues and eventually to the skin surfaces through a sinus tract. The involucrum can gradually inaease in density and thickness to form part or all of a new shaft.
New bone increases in amount and density for weeks or months according to the size of the bone and the extent and duration of infection. Endosteal new bone may proliferate and obstruct the medullary canal. After host defense, removal or surgical removal of the sequestrum, the body, especially in children, may fill the remaining cavity with new bone. However, in adults, the cavity may persist or the space may be filled with fibrous tissue. The surviving bone in the osteomyelitis field usually becomes osteoporotic during the active period of infection. Osteoporosis is the result of the inflammatory reaction and disuse atrophy. After the infection subsides, bone density increases partially from reuse. It may be difficult to distinguish between the old living bone and the newly formed bone as time passes. All traces of osteomyelitis can disappear in children and, to a lesser extent, in adults.
TREATMENT
Medical therapy: A single pathogenic organism is almost always recovered from the bone. The most common bone isolates are staphylococci, the most common gram-negative organism is P aeruginosa, and the most common anaerobe is Peptostreptococcus species. However, in immunocompromised patients, other organisms must also be considered, including fungi and mycobacteria.
Hematogenous osteomyelitis in children usually can be treated with antibiotic therapy alone. However, it is vital to identify a pathogen in order to select the optimal antibiotic therapy. Mismanagement with inappropriate antibiotic(s) encourages disease extension, necrosis, and sequestra formation. A bone biopsy for culture is necessary unless the patient has positive blood cultures along with radiographic findings consistent with osteomyelitis. After cultures are obtained, empiric antibiotics should be selected to cover the most probable pathogens.
Once the etiologic organism is identified, the antibiotic regimen should be modified, if needed, based upon susceptibility patterns. The patient should be treated for 4-6 weeks with appropriate antimicrobial therapy, dating from the initiation of therapy or following the last major debridement surgery. If the initial medical management fails and the patient is clinically compromised by a recurrent infection, medullary and/or soft tissue debridement is necessary in conjunction with another 4- to 6-week course of antibiotics. Oral antibiotics can be used in pediatric hematogenous osteomyelitis. However, the child should receive 7-14 days of IV antibiotics or continue to receive IV antibiotics until systemic improvement occurs prior to changing to an oral regimen. The latest reports suggest the use of IV antibiotics for 3-4 days; this usually is enough for the systemic manifestations to improve. In order to undergo oral therapy, the patient must be compliant and have close outpatient follow-up care. Absorption and activity of the orally administered antibiotic should be monitored using serum cida! levels. High doses of the quinolone class of antibiotics can cause articular cartilage damage in young animals, generating some concern about the long-term use of these agents in infants and children. Thus, under most circumstances, children with osteomyelitis should not be treated with a quinolone.
Surgical therapy: Surgical management of contiguous focus osteomyelitis can be very challenging. The principles of treating any infection are equally applicable to the treatment of infection in bone. These include adequate drainage, extensive debridement of all necrotic tissue, obliteration of dead spaces, stabilization, adequate soft tissue coverage, and restoration of an effective blood supply.
The number and nature of the required surgical procedures increases with the severity of the infection, which can be divided into 4 categories, as follows:
Category 1 - Removal of necrotic tissue by extensive debridement
Category 2 - Dead space obliteration with flaps, antibiotic beads, and bone grafts
Category 3 - Provision of soft tissue coverage of the bone
Category 4 - Stabilization of bone by external or open reduction and internal fixation
Category 1
Debridement surgery is the foundation of osteomyelitis treatment. It is the most commonly performed procedure and may need to be repeated multiple times. The goal of debridement is to reach healthy, viable tissue, but even when all necrotic tissue has been adequately debrided, the remaining bed of tissue must be considered contaminated with the responsible organism. Debridement should be direct, atraumatic and executed with reconstruction in mind. All dead or ischemic hard and soft tissue is excised unless a noncurative procedure has been chosen. Surgical excision of bone is carried down to uniform haversian or cancellous bleeding, known as the paprika sign.
Category 2
Adequate debridement may leave a large bony defect (dead space). Appropriate management of dead space created by debridement surgery is mandatory in order to arrest the disease and to maintain the integrity of the skeletal part. The goal of dead space management is to replace dead bone and scar tissue with durable vascularized tissue. Local tissue flaps or free flaps may be used to fill dead space. An alternative technique is to place cancellous bone grafts beneath local or transferred tissues where structural augmentation is necessary. Careful preoperative planning is critical for conservation of the patient's limited cancellous bone reserves. Open cancellous grafts without soft tissue coverage are useful when a free tissue transfer is not a treatment option and local tissue flaps are inadequate.
Complete primary or delayed primary wound closure should be performed whenever possible. Suction irrigation systems are not recommended because of the high incidence of associated nosocomial infections and the unreliability of the apparatus. Healing by secondary intent is also discouraged since the scar tissue that fills the defect may later become avascular. Antibiotic-impregnated acrylic beads can be used to sterilize and temporarily maintain dead space. The beads are usually removed within 2-4 weeks and replaced with a cancelious bone graft. The most commonly used antibiotics in beads are vancomycin, tobramycin and gentamicin. Local delivery of antibiotics (amikacin, clindamycin) into dead space also can be achieved with an implantable pump.
Category 3
Adequate coverage of the bone by soft tissue is necessary to arrest osteomyelitis. Most soft tissue defects are closed primarily, but small soft tissue defects may be covered with a split thickness skin graft. In the presence of a large soft tissue defect or an inadequate soft tissue envelope, local muscle flaps and free vascularized muscle flaps may be placed in a 1- or 2-stage procedure.
Local and free muscle flaps, when combined with antibiotics and surgical debridement of all nonviable osseous and soft tissue for chronic osteomyelitis, have a success rate ranging from 65% to 100%. Local muscle flaps and free vascularized muscle transfers improve the local environment by supplying blood vessels, which are critical for host defense, antibiotic delivery, and osseous and soft tissue healing.
Category 4
If movement is present at the site of infection, measures must be taken to achieve permanent stability of the skeletal unit. Stability can be achieved with plates, screws, rods, and/or an external fixator. One type of external fixation allows bone reconstruction of segmental defects and difficult infected nonunions. The Ilizarov external fixation method uses the theory of distraction histogenesis, in which bone is fractured in the metaphyseal region and slowly lengthened. The growth of new bone in the metaphyseal region pushes a segment of healthy bone into the defect left by surgery. The Ilizarov technique is used for difficult cases of osteomyelitis when stabilization and bone lengthening are necessary. It also can be used to compress nonunions and correct malunions, and in a small group of patients for reconstruction of difficult deformities that result from osteomyelitis. However, this technique is labor intensive and requires an extended period of treatment, averaging 9 months in the device. The Ilizarov pins usually become infected, and the device is painful. Infected pseudoarthrosis with segmental osseous defects can be treated by debridement and microvascular bone transfers. Vascularized bone transfer is also useful for the treatment of infected segmental osseous defects of long bones that are more than 3 cm in length. Vascularized bone transfers can be placed after 1 month without clinical evidence of infection.
Loss of bone stability, bone necrosis, and soft tissue damage frequently occur in contiguous focus osteomyelitis. Surgical debridement of infected bone and soft tissue provides specimens for culture and hastens eradication of the infection. Other steps in the surgical management of contiguous focus osteomyelitis should be tailored to the specific anatomy of the bone infection. When osteomyelitis is characterized by a full thickness, cortical sequestration, patients usually can be treated with removal of the dead infected bone (bone saucerization). Bone grafting may be necessary to augment structural support. These patients may require external fixation for structural support while the bone graft incorporates. Complex reconstruction of both bone and soft tissue is frequently necessary. In some cases, osteomyelitis progresses to an infection involving the entire diameter of the bone. These patients often require an intercalary resection of the bone in order to arrest the disease process. Since this advanced stage of osteomyelitis involves an entire through-and-through section of bone, a loss of bony stability occurs either before or after debridement surgery. As a result, treatment often must be directed toward establishing structural stability and obliterating debridement gaps by means of cancellous bone grafts or the Ilizarov technique. Vascularized bone grafting is the other possible treatment modality.
Preoperative details: In addition to routine preoperative preparations, supportive therapy is needed; infants and children must be well hydrated and fever must be controlled before the patient undergoes general anesthesia. Patients who are medically compromised should be stabilized and supported. Diabetes should be controlled as much as possible, but this should not delay drainage because the presence of infection makes the blood sugar level refractory and difficult to control. Most of the systemic manifestations of osteomyelitis improve dramatically after drainage and debridement.
Intraoperative details: Position the patient in the most accessible position to drain the infected areas. Prepare all containers and swabs, and prepare the requests before scrubbing. Prepare containers for tissue cultures. Prepare for Gram stain, aerobic culture and sensitivity, anaerobic culture and sensitivity, fungal culture and sensitivity. (Acid-fast bacillus [AFB] stain and culture and sensitivity are recommended.) Incision should be generous for ease of access to the infected bone. Decompression may release intrameduilary or subperiosteal pus. All necrotic soft tissue, bone, and devitalized tissue must be removed. Infected loculations must be broken and thorough washing with as much as 2-4 L of isotonic sodium chloride solution is essential.
Complete debridement of all the devitalized bone and soft tissue, regardless of the size of the wound created, is essential for cure. Immobilization of the bone by cast or external fixations is a must.
Revascularization procedures are the best means of fighting recurrent infection; those involving local pedicle muscle flaps and myocutaneous flaps are now the ones most frequently used to fill the space created by surgery. Local muscle flaps are limited by the availability of adjacent muscle but are very useful because the vascular supply is kept intact. Myocutaneous flaps have the advantage of providing vascular supply to both the muscle and the overlying skin. Increasingly, microsurgically transplanted muscle flaps (ie, free-flaps) are being used in areas such as the distal tibia where no appropriate muscle exists.
Complex orthopedic techniques are necessary to repair very large bone defects that would otherwise be considered untreatable except by amputation. In the Ilizarov technique, the resection of diseased tissue and bone creates a gap partially filled by a weli-vascularized bone segment. Transfer of the bone graft leads to progressive local generation of new bone.
Postoperative details: Dramatic improvement is the usual course after debridement, but patients require attention to prevent complications related to their original medical conditions, such as diabetes and heart failure. IV fluids, IV antibiotics, and suitable analgesics are required for the first few days after surgery. Intensive care unit (ICU) admission for respiratory support and blood gases and renal function monitoring should be considered for patients who have septicemia.
The wound should be dressed daily, and early sitting and mobilization (affected limb must be immobilized) should be encouraged.
If no Improvement occurs within 48 hours, a second look debridement and dressing under general anesthesia is indicated.
Follow-up care: The patient must be compliant with care and have close outpatient follow-up. The first visit is usually a week after discharge and consists of a general examination for evaluation of improvement. Local examination and documentation of pain, wound condition, tenderness, swelling, and discharges from wounds should be made in all visits, Repeat CBC, CRP, ESR, and plain radiographs to evaluate the progression and behavior of the infection.
The cast should be removed when infection is eradicated, which is usually determined by good reduction in the level of CRP, ESR, or both. The shoulder, elbow, and wrist should not be immobilized more than 3, 4, and 5 weeks, respectively.
Physiotherapy is an essential part of follow-up care; isometric exercises should be started early, and once the cast is removed, active and passive range of motion exercises are suggested.
CHRONIC OSTEOMYELITIS
Chronic osteomyelitis is prolonged inflammation of bone marrow, almost invariably due to infection.
This was once the almost inevitable outcome of acute haematogenous osteomyelitis; today, antibiotics will normally prevent this progression and now the most common causes of chronic osteomyelitis are open fractures and surgery.
Causative organisms
Chronic osteomyelitis is always a mixed infection. The common organisms include:
Staphylococcus aureus
Escherichia coti
Streptococcus pyogenes
Proteus spp.
Pseudomonas spp.
In the presence of a foreign implant, a common opportunist is Staphylococcus epidermidis.
Pathology
The infection may remain focussed in a discrete region, or more commonly spread along the shaft of a long bone.
Necrotic bone is found in cavities - sequestrum - containing pus and walled of with vascular tissue and sclerotic new bone - involucrum.
The sequestrum acts as a haven for bacteria, permitting continued infection until the bone is passed through a draining sinus or removed surgically.
The infection may follow a relapsing and remitting course; the sinuses may close off for weeks or months, only to reopen as pus reaccumulates.
The sclerotic involucrum is more brittle than normal bone and is liable to pathological fractures.
Clinical features
The patient will have a history of osteomyelitis, and will present with:
recurrent pain, pyrexia, redness and swelling
reopening of the sinus
The overlying tissues are often thickened and puckered where they are tethered to the bone.
Any discharge is foul and seropurulent. There may be excoriation of surrounding skin.
Diagnostic imaging
Plain radiographs show bone resorption at the site of infection with thickening and sclerosis of surrounding bone. The thickened bone may resemble a bone tumour. Sequestrae are necrotic and appear abnormally radio-dense. A sino-gram may help estimate the extent of the abscess.
Radioisotope scans using 99m-Tc diphosphonates show increased uptake at the sites of osteomyelitis. Indium- labelled leukocytes are more specific for infection.
CT and MRI are essential for surgical planning as they allow visualisation of the extent of infection and tissue destruction.
Investigations
During a flare-up of chronic osteomyelitis the ESR and white blood cell count may be elevated.
Discharging pus should be cultured to determine the organisms and their sensitivity.
Treatment
There are three principles of treatment:
antibiotic therapy
local treatment of the sinus
surgery
Surgery should be postponed until there are significant symptoms combined with clear evidence of a sequestrum.
Sulphan blue is injected preoperatively; this stains all vital tissue green, leaving dead tissue unstained. Under antibiotic cover, the surgeon removes all dead i.e. unstained -tissues and bone.
There are several strategies to prevent reinfection and promote healing:
double lumen tubes are left in the lumen and antibiotic solution is introduced and aspirated 4 hourly; this is continued until the aspirate is sterile (3-6 weeks) and then the tube is gradually removed
the cavity may be packed with gentamicin beads
the cavity may be packed with multiple small bone grafts
a muscle flap with an intact blood supply may be laid into the cavity
Antibiotic therapy
Chronic osteomyelitis is rarely cured by antibiotic therapy alone. Their role is twofold:
to prevent the spread of infection to healthy bone
to control acute flares of infection
Sensitivity determination of the pathogens is essential. It is also important that the drugs are non-toxic with long term use and that they penetrate bone well. Good examples are clindamycin and cephalosporins.
Local treatment
The discharging sinus may be painless and only require simple dressing.
Excoriation can be prevented with colostomy paste.
An acute abscess may be treated temporarily by incision and drainage.
Complications
septicaemia / pyaemia
septic arthritis
direct spread of infection
deformity or alteration in growth rate due to damage to the growth plate
amyloidosis
PRIMARY-CHRONIC OSTEOMYELITIS
1. Chronic Sclerosing Osteomyelitis:
• chronic sclerosing osteomyelitis (of Garre) has dense sclerotic
• appearance and often no associated lucency on radiographs;
• lesion usually involves the entire circumference of the bone and is much more widespread than a stress fracture;
• thinner linear sclerotic appearance of a stress fracture should be characteristic enough to distinguish the two lesions;
• serial radiographs generally show little or no change within a short time in sclerosing osteomyelitis;
• typical stress fracture, however, has a rapidly evolving course over several weeks;
2. Brodie's abscess
• A Brodie's abscess is a localised pyogenic abscess cavity arising in the metaphysis of one or more long bones - in particular the tibia and the femur.
• This condition develops insidiously, often with no prior symptoms.
• The abscess cavity is lined with granulation tissue and there is a surrounding reactive bone sclerosis.
• In established infection treatment involves excision and sequestrectomy
TESTS
1. Felon in the form of cuff-link is as follows:
A. Thecal with spreading of process to the hand.
B. Subcutaneous with spread of in the epidermis.
С Paronychia.
D. Osteal felon with spread of process to the joint.
E. Aritcular felon.
Choose the correct answer.
2. The types of early felon that require puncturing both for diagnosis and treatment are as follows:
A. Cutaneous.
B. Subcutaneous.
C. Tenosynovitis.
D. Paronychia.
E. Osteal.
Choose the correct answer.
3. The risk of suppurative spreading onto the forearm is high in the following felons:
1. The I finger.
2. The II finger.
3. The III finger.
4. The intravenous finger.
5. The V finger.
Choose the right combination of answers:
A. 1,3. B. 2, 3, 4. С. 1,5. D. 2, 5. E. 1, 2, 3, 4, 5.
4. Subungual felon requires the following surgeries:
1. Oval incision by Klapp.
2. Perforation of the nail.
3. Semi-oval incisions.
4. Resection of the nail bed.
5. Removal of the nail plate.
Choose the right combination of answers:
A. 1,4, 5. B. 2, 3,4. С. 2, 4, 5. D. 3, 4, 5. E. 1, 3, 5.
5. The clinical signs of paronychia are as follows:
1. Swelling of the cutaneous margin.
2. «Floating» nails.
3. Secretion of pus from under the cutaneous margin.
4. Suppurative fistula.
5. Extensive contracture of finger.
Choose the right combination of answers:
A. 1,2, 3. B. 1,3. С. 3,4, 5. D. 2, 4. E. 1,3,4.
6. The local signs of tenosynovitis are as follows:
1. Throbbing pain.
2. Swelling of the entire finger.
3. The finger is extensively straightened out.
4. Fixation of the finger.
5. Painful sensation along the tendon on palpation with a probe.
Choose the right combination of answers:
A. 1, 2. B. 1, 2, 3. С. 1, 3, 4. D. 1, 3, 4, 5. E. 1,2,4,5.
7. The cross (V-form) hand phlegmon is characterized by the following clinical signs:
1. Tenderness.
2. Hand dysfunction.
3. Localization of suppurative exudate in proximal area of the palm.
4. Localization of suppurative exudate in the distal areas of the palm.
5. Extensive contracture of fingers.
Choose the right combination of answers:
A. 1,2, 3. B. 1,2, 4. С. 2, 3,4. D. 1,2, 4, 5. E. 1, 2, 3,5.
8. The local signs of middle space phlegmon are as follows:
1. Tension of the skin being in the centre of the palm.
2. Fluctuation.
3. Tenderness.
4. Swelling of the dorsal hand surface.
5. Finger flexion.
Choose the right combination of answers:
A. 1,2. B. 1,4. С. 1,3, 5. D. 1,3,4. E. 1, 3, 4, 5.
9. The bones that are commonly affected in haematoge-nous osteomyelitis are as follows:
1. The femur.
2. The ischium.
3. The vertebrae.
4. The tibia.
5. The brachium.
Choose the right combination of answers:
A. 1,4. B. 2, 3, 5. С. 1,4, 5. D. 2, 4, 5. E. 1, 3, 4.
10. The common age of patients with haematogenous osteomyelitis is:
1. 1-10 years.
2. 11-20 years.
3. 21-30 years.
4. 31—40 years.
5. 41-50 years.
Choose the right combination of answers:
A. 1. B. 2. С. 1,2, 3. D. 1,2. E. 3, 4, 5.
11. Bone sequestration is typical of which of the followius types of osteomyelitis:
1. Brodie's abscess.
2. Post-traumatic osteomyelitis.
3. Ollier's osteomyelitis.
4. Garre's osteomyelitis.
5. Haematogenous osteomyelitis.
Choose the right combination of answers:
A. 1,2, 5. B. 2, 3,4. С. 2, 4, 5. D. 2, 5. E. 3, 5.
12. In acute haematogenous osteomyelitis, X-ray findings are evident:
A. Within 3 days.
B. Within 3 months.
C. Within 10-15 days.
D. Within 20-30 days.
E. Within 30-40 days.
Choose the correct answer.
13. The following are distinctive signs of Brodie's abscess:
1. Cavity with sequestrum.
2. Cavity without sequestrum.
3. Mucous exudates.
4. Purulent exudates.
5. Diffuse osteosclerosis.
Choose the right combination of answers:
A. 1,4. B. 2, 4, 5. С. 2, 4. D. 1, 3, 5. E. 1, 4, 5.
14. The following are distinctive signs of Garre's osteomyelitis:
1. Metaphyseal cavity.
2. Bone thickening.
3. Sequestrum.
4. Albuminous exudates.
5. Osteosclerosis.
Choose the right combination of answers:
A. 1,4. B. 1,2, 3. С. 3,4, 5. D. 2, 4. E. 2, 5.
15. Sequestra are formed in the following types of osteomyelitis:
1. Brodie's abscess.
2. Haematogenous osteomyelitis.
3. Garre's osteomyelitis.
4. Tumorous osteomyelitis.
5. Post-traumatic osteomyelitis.
Choose the right combination of answers:
A. 1,2,5. B. 2, 3,4. С. 2, 4, 5. D. 2, 5. E. 3, 5.
16. The major signs of chronic haematogenous osteomyelitis are as follows:
1. Tendency to relapsing.
2. Muscular atrophy.
3. Suppurative fistulas
4. Sequestral box with sequestrum inside
5. Osteosclerosis
Choose the right combination of answers:
A. 1,2, 4. 5. B. 1,3, 4, 5. С. 1,2, 3,4, 5. D. 2, 4, 5.
17. The characteristics of chronic haematogenous osteomyelitis are as follows:
1. The diaphyses of long bones are more frequently affected.
2. The metaphyses and epiphyses of long bones are more frequently affected.
3. Muscular atrophy is only rare.
4. Muscular atrophy is common.
5. Lesions of neighbouring joints are uncommon. Choose the right combination of answers:
A. 1,3,5. B. 2, 3,5. С. 1,2, 5. D. 4, 5. E. 1,4, 5.
18. The clinical signs suggestive of advanced acute hae-matogenous osteomyelitis are as follows:
1. Skin hyperaemia.
2. Bone deformation.
3. Positive fluctuation sign.
4. Skin necrosis.
5. Suppurative fistulas.
Choose the right combination of answers:
A. 1, 2, 5. B. 1, 3, 5. С. 3, 4, 5. D. 2, 3, 5. E. 1,4,5.
19. The aetiologies of osteomyelitis are as follows:
1. E. coli.
2. Staphylococcus spp.
3. Drumstick bacillus.
4. Corynebacterium diphtheriae.
5. Proteus mirabilis.
6. Streptococcus spp.
Choose the right combination of answers:
A. 1,3, 5, 6. B. 1,2, 5, 6. С. 2, 4, 5, 6. D. 1, 3, 4, 6. E.2, 3, 5, 6.
20. The surgical procedures indicated for acute haematog-enous osteomyelitis are as follows:
1. Incision of phlegmon.
2. Incision of phlegmon with incision of the periosteum.
3. Trepanation along the affected bone.
4. Resection of the affected bone.
5. Decompression drainage of the bone canal.
Choose the right combination of answers:
A. 1,3,4. B. 2,4, 5. С. 2, 3,5. D. 1, 3, 5. E. 2, 5.
21. The most effective methods after radical sequestrecto-my are as follows:
1. Filling with plaster.
2. Myoplasty.
3. Prolonged flow washing.
4. Tamponade.
5. Plastics with collagen sponge and antiseptics.
Choose the right combination of answers:
A. 1,2, 3. B. 2, 3, 4. С. 3,4, 5. D. 2, 3, 5. E. 1, 3, 5.
22. The appropriate extension of the surgery in chronic osteomyelitis may be as follows:
1. Fistula excision.
2. Bone perforation.
3. Sequestrectomy.
4. Phlegmon incision.
5. Bone cavity plastics.
6. Prolonged active flowing drainage
Choose the right combination of answers:
A. 2, 3, 4, 5. B. 1, 2, 5, 6. С. 1, 3, 5, 6. D. 3, 4, 5, 6. E. 1,3,4,6.
23. The most common chronic complications of chronic osteomyelitis are as follows:
1. Liver cirrhosis.
2. Renal amyloidosis.
3. Endocarditis.
4. Myocardial dystrophy.
5. Chronic anaemia.
Choose the right combination of answers:
A. 1,2. B. 2, 3. C.2,5. D. 1,4. E. 1,5.
24. The most adequate preparations and methods of immune and antibacterial therapy of acute osteomyelitis are as follows:
1. Lincomycin hydrochloride.
2. Ampiox.
3. Antibiotics IM.
4. Prodiogiosane.
5. Bacteriophages.
Choose the right combination of answers:
A. 2, 4, 5. B. 1, 2, 4, 5. С. 1, 4, 5. D. 1, 2, 4, 5. E. 1,2, 3,4, 5.
ANSWERS.
1 - B
2 - C
3 - C
4 - C
5 - A
6 - E
7 - A
8 - E.
9 - A
10 - D
11 - E
12 - C
13 - C
14 - E
15 - D
16 - B
17 -A
18 - B
19 - B
20 - C
21 - D
22 - C
23 - C
24 - E
References
Gostischev V. K. General surgery / The manual. – M.: GEOTAR-MED, 2003. – Charter XI. – P.150-191.
Moukonin A.A., Golub A.V. Soft tissue infection: Textbook for foreign students. – Smolensk: Smolensk State Medical Academy, General Surgery Department. – 2005. – 9p.
Moukonin A.A., Golub A.V. Osteomyelitis: Textbook for foreign students. – Smolensk: Smolensk State Medical Academy, General Surgery Department. – 2005. – 22p.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
HIDRADENITIS SUPPURATIVE. LYMPHANGITIS, LYMPHADENITIS. ACUTE MASTITIS. (classification, clinical features, diagnostics, treatment).
Составитель: доцент Ю.И.Ломаченко
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
HYDRADENITIS SUPPURATIVE
Hydradenitis is a suppurative inflammation of the apocrine sweat glands. Examination of the patient reveals a painful swelling often in the axilla, and rarely in the inguinal and perianal regions – the areas where the apocrine sweat glands are located. The personal history reveals the presence of some predisposing factors: increased sweating, poor hygiene, the use of depilator and the shaving of the axillary region.
The disease is marked by sudden onset with the appearance of a small painful nodule, which increases in size up to 1–2 cm in diameter and sharply protrudes above the surrounding skin level.
Examination reveals a violet-red swelling. When several sweat glands are involved, they coalesce to form a firm infiltration, which can occupy the whole axillary fossa. Single nodules are superficial and fixed to the skin. After 10–15 days the center of the swelling softens up, fluctuation is noticeable, and some thick milky pus starts to discharge from the burst area. Once the pus is evacuated, healing starts with the formation of a scar. The disease tends to recur.
When the surrounding subcutaneous fatty layer gets involved in the process, a phlegmon develops, and when the lymph nodes are involved – lymphadenitis.
Unlike furuncle, the infiltration is devoid of follicular pustules or necrotic centers. Axillary hydradenitis is characterized by deep-seated infiltrations, enlarged lymph nodes, and the skin over the lesion is not firmly attached to it.
Hydradenitis is treated with antibiotics, and long-acting sulphanylamides. Immunization with staphy-lococcal anatoxin is prescribed. The hair in the axilla is shaved, the skin is cleaned with spirit, and smeared with a 3% solution of brilliant green. Ultrasound and ultraviolet irradiation are used as physical therapeutic measures.
In the case of an abscess formation, surgery has to be performed – incision and drainage. If long-term treatment of hydradenitis proves unsuccessful and there is fear of ensuing sepsis, the whole subcutaneous fatty layer of the axillary fossa is excised such as with a carbuncle.
ACUTE LYMPHANGITIS
Acute inflammation of the subcutaneous lymphatic channels, usually caused by S. pyogenes.
Symptoms, Signs, and Diagnosis
Streptococci most commonly enter the lymphatic channels from an abrasion, wound, or infection (usually cellulitis) on an extremity. Red, irregular, warm, tender streaks develop on an extremity and extend proximally from a peripheral lesion toward regional lymph nodes, which are typically enlarged and tender. Systemic manifestations (e.g., fever, shaking chills, tachycardia, headache) are common and often more severe than the cutaneous findings suggest; occasionally, they precede any evidence of significant local infection. Leukocytosis, sometimes marked, is usual.
Diagnosis is based on the symptoms and signs. As in cellulitis, isolation of the responsible organism is uncommon unless there is pus, an open wound, or bacteremia.
Course and Treatment
Bacteremia with metastatic foci of infection may occur, often with startling rapidity. Rarely, cellulitis with suppuration, necrosis, and ulceration develops along the involved lymph channels. Most cases respond rapidly to antibiotics.
LYMPHADENITIS
Inflammation of lymph nodes.
Etiology
Any pathogen - bacterial, viral, protozoal, rickettsial, or fimgal - can cause lymphadenitis. Lymph node involvement may be generalized, with systemic infection, or confined to regional lymph nodes draining a local area of infection. Generalized lymph node enlargement is common in infectious mononucleosis, cytomegaloviras infection, toxoplasmosis, brucellosis, secondary syphilis, and disseminated histoplasmosis. Regional iymphadenopathy is prominent in streptococcal disease, tuberculosis or nontuberculous mycobacterial disease, tularemia, plague, cat-scratch disease, primary syphilis, lymphogranuloma venereum, chancroid, and genital herpes simplex.
Symptoms, Signs, and Diagnosis
Lymph node enlargement from edema and WBC cellular infiltration, the major sign of lymphadenitis, may be asymptomatic or may cause pain and tenderness. With some infections the overlying skin is inflamed, occasionally with cellulitis; abscess formation may occur, and penetration to the skin will produce draining sinuses.
Lymphadenitis and its cause are usually clinically apparent. Occasionally, however, lymph node aspiration and culture or excisional biopsy is necessary.
Treatment
Treatment depends on the underlying cause. With resolution of the primary process, lymph node enlargement usually resolves, but firm, nontender Iymphadenopathy sometimes persists. Hot, wet dressings may help relieve symptoms of acutely painful lymph nodes. Abscesses require surgical drainage.
MASTITIS
Mastitis is an inflammatory condition of the breast, which may or may not be accompanied by infection. It is usually associated with lactation, so it is also called lactational or puerperal mastitis. It can occasionally be fatal if inadequately treated. Breast abscess, a localised collection of pus within the breast, is a severe complication of mastitis. These conditions form a considerable burden of disease and involve substantial costs.
Epidemiology
Incidence
Mastitis and breast abscess occur in all populations, whether or not breastfeeding is the norm. The reported incidence varies from a few to 33% of lactating women, but is usually under 10%. The incidence of breast abscess also varies widely, and most estimates are from retrospective studies of patients with mastitis. However, according to some reports, especially from developing countries, an abscess may also occur without apparent preceding mastitis.
Time of occurrence
Mastitis is commonest in the second and third week postpartum, with most reports indicating that 74% to 95% of cases occur in the first 12 weeks. However, it may occur at any stage of lactation, including in the second year. Breast abscess also is commonest in the first 6 weeks postpartum, but may occur later.
Causes of mastitis
The two principle causes of mastitis are milk stasis and infection. Milk stasis is usually the primary cause, which may or may not be accompanied by or progress to infection.
The efficient removal of milk as it is formed could largely prevent mastitis; infection when it occurred is not primary, but resulted from the stagnant milk providing a medium for bacterial growth.
Taking in to consideration the leukocytes and bacteria in milk from breasts with clinical signs of mastitis following classification was proposed:
Milk stasis
Non-infectious inflammation (or non-infectious mastitis)
Infectious mastitis.
It was found, in a randomised study, that milk stasis (<106 leukocytes and <103 bacteria) improved with continued breastfeeding alone; non-infectious mastitis (>I06 leukocytes and <103 bacteria) required treatment by additional expression of milk after a feed, and infectious mastitis (>106 leukocytes and >103 bacteria) was treated effectively only with both removal of milk and systemic antibiotics. Without effective removal of milk, non-infectious mastitis was likely to progress to infectious mastitis, and infectious mastitis to the formation of an abscess.
Milk Stasis
Milk stasis occurs when milk is not removed from the breast efficiently. This may occur when the breasts are engorged soon after delivery, or at any time when the infant does not remove the milk that is produced from part or all of the breast. Causes include poor attachment of the infant at the breast, ineffective suckling, restriction of the frequency or duration of feeds, and blockage of milk ducts.
Infection
Infecting organisms
The commonest organisms found in mastitis and breast abscess are coagulase-positive Staphylococcus aureus and Staphylococcus albus. Escherichia coli and Streptococcus (a-, p-, and non- haemolytic) are sometimes found, and the latter has in a few cases been linked to neonatal streptococcal infection. Rarely, mastitis has been recognised as a complication of typhoid fever and other salmonella infections. M. tuberculosis is another rare cause of mastitis. In populations where tuberculosis is endemic, M. tuberculosis may be found in about 1% of cases of mastitis and associated in some cases with tuberculous tonsillitis in the infant. Candida have been reported to cause fungal mastitis but mycoplasma and chlamydia have not.
Bacteria are often found in milk from asymptomatic breasts, in both industrialised and developing countries. The spectrum of bacteria is often very similar to that found on skin, for example, Staphylococcus epidermidis, diphtheroids, and alpha-haemolytic and non-haemolytic streptococci. Bacteriological studies are therefore complicated by the difficulty of avoiding contamination from skin bacteria. Despite careful techniques for collection, only 50% of milk cultures may be sterile, while others show "normal" colony counts from 0 to 2,500 colonies per ml..
Thus the presence of bacteria in the milk does not necessarily indicate infection, even if they are not contaminants from the skin. One way to distinguish between infection and simple bacterial colonisation of the milk ducts is to look for bacteria coated with specific antibodies. As with urinary tract infection, bacteria in breastmilk which are coated by immunoglobulins IgA and IgG demonstrate that a specific immune reaction to an infection has taken place. However, facilities for such an investigation are not routinely available in many situations.
Epidemic puerperal mastitis
Epidemic mastitis has been regarded as a hospital acquired disease caused by highly virulent strains of penicillin-resistant S. aureus. It has become rarer since the advent of antibiotics and the use of more powerful bactericides for cleaning hospitals; but it has also become rarer since practices which favoured milk stasis have become less widespread, such as restrictive feeding schedules, and interruption of feeding from a breast with a fissured nipple; and since infants in hospital have roomed-in with their mothers instead of staying in nurseries.
Route of infection
How infection enters a breast is uncertain. Several routes have been suggested: through the lactiferous ducts into a lobe; by haematogenous spread; and through a nipple fissure into the periductal lymphatic system. Nipple fissure has been reported with increased frequency in the presence of mastitis.
An association between Candida infection of the nipple and mastitis, particularly recurrent mastitis, has often been noted. Mastitis due to Candida has occasionally been reported, particularly in diabetic
women, but is extremely rare. It is more likely that nipple fissure resulting from candidiasis could provide an entry point for bacterial infection. It is also possible that, when nipples are painful and damaged as a result of Candida, a woman may use the breast less efficiently, leading to milk stasis. However, candidacies often follows antibiotic treatment, and it may occur as an indirect consequence of mastitis rather than being a predisposing factor.
Deep burning breast pain occurring during and after feeds is often attributed to Candida infection of the mammary ducts, but recently S. aureus has been identified as a pathogen in cases of deep pain as well as of nipple fissure. Deep pain could be due to infection in the mammary ducts, but whether there is any connection with mastitis is unclear.
Predisposing factors
There are a number of factors which it has been suggested might increase the risk of mastitis. Evidence exists for some, but most remain anecdotal. Their importance is likely to be small compared with that of breastfeeding technique: good attachment and effective milk removal.
Pathology and clinical features
Non-infectious mastitis
When milk is not removed from part or all of a breast, milk production slows and eventually ceases. However, this process takes some days and may not be complete for 2-3 weeks. In the meantime the accumulated milk may cause an inflammatory response.
The inflammation is responsible for the signs and symptoms of mastitis. Part of the breast is painful, red, swollen, and hard. Usually only one breast is affected. The woman often has a fever and feels ill. However, it was observed that one third to one half of women with mastitis had local signs only.
Infectious mastitis
Infective mastitis results if milk stasis remains unresolved, and the protection provided by the immune factors in milk and by the inflammatory response is overcome. Fresh human milk is not normally a good medium for bacterial growth, and for infection to occur conditions must be present which prevent the breast from destroying and eliminating bacteria. The natural direction of the flow of milk along the ducts, when removed efficiently, would be expected to wash any organisms down and out of the breast. Inefficient milk removal, resulting in accumulation of milk, creates the conditions favorable to bacteria! growth, and the anti-infective processes may be overwhelmed.
The signs and symptoms of infectious mastitis are, as discussed above, impossible to distinguish from non-infectious mastitis. Part of usually one breast becomes red, painful, swollen and hard, and there may be general symptoms of fever and malaise. An accompanying sign may be a nipple fissure. Infectious mastitis has been classified by different authors in several ways. First according to its site: superficial mastitis occurring in the dermis and intramammaiy mastitis located either in the glandular tissue itself, (parenchyma’s) or in the connective tissue of the breast (interstitial). Second, according to the epidemiological patterns: epidemic or sporadic.
Cell counts and bacterial colony counts are useful to distinguish between infectious and non-infectious mastitis. Culture of the breastmilk may help to determine the infecting organism, if there is one, and its antibiotic sensitivity.
If culture is not possible as a routine, it can be done selectively:
- For hospital-acquired, or severe or unusual cases;
- If there is no response to antibiotics within two days;
- If there is recurrent mastitis;
Recurrent mastitis may be due to delayed or inadequate treatment of the initial condition or uncor-rected poor breastfeeding technique. Sometimes recurrence is associated with candidiasis. Occasionally there is an underlying breast condition which causes persistently poor drainage of part of a breast, such as a ductal abnormality, a cyst or tumour, which should be identified and treated accordingly.
Breast Abscess
A lactating breast, as any other infected tissue, localises infection by forming a barrier of granulation tissue around it. This becomes an abscess capsule, which is filled with pus.
There is a severely painful swollen lump, with redness, heat, and oedema of the overlying skin. In neglected cases the lump may be fluctuant, with skin discoloration and necrosis. Fever may or may not be present. To confirm the diagnosis, pus can be aspirated with a syringe and wide bore needle. The differential diagnosis of breast abscess includes galactocele, fibroadenoma, and carcinoma.
Prevention
Mastitis and breast abscess are largely preventable, if breastfeeding is managed appropriately from the beginning to prevent situations which give rise to milk stasis, and if early signs such as engorgement, blocked duct and nipple soreness are treated promptly. This is needed as part of normal maternity care, and as an ongoing part of both facility based and community care for women and children.
Control of infection
While appropriate management of breastfeeding is fundamental for the prevention of mastitis, reduction of the risk of infection it is also important, especially in the hospital setting.
Thorough and frequent hand washing by both health workers and mothers is necessary. Health workers should wash their hands after every contact with a mother or infant, or with any possible source of pathogenic organisms. Plain soap is adequate to remove surface organisms, but for health workers in frequent contact with body fluids, an anti-microbial hand washing product is more effective, provided it is in contact with the skin for at least 10 seconds per wash. It was showed that additional hand disinfection at the bedside of breastfeeding mothers in hospital reduced the incidence of mastitis from 2.8% to 0.66%.
Treatment
Blocked duct
Treatment requires improved removal of milk, and avoiding any obstruction to milk flow.
Mastitis
If despite all efforts at prevention, mastitis occurs, it must be treated promptly and adequately. If treatment is delayed or incomplete, recovery is less satisfactory. There is an increased risk of breast abscess and relapse.
The main principles of treatment of mastitis are:
SUPPORTIVE COUNSELLING
Mastitis is a painful and frustrating experience, and it makes many women feel very ill. In addition to effective treatment and control of pain, a woman needs emotional support. She may have been given conflicting advice from health professionals, she may have been advised to stop breastfeeding, or given no guidance either way. She may be confused and anxious, and unwilling to continue breastfeeding.
She needs reassurance about the value of breastfeeding; that it is safe to continue; that milk from the affected breast will not harm her infant; and that her breast will recover both its shape and function subsequently. She needs encouragement that it is worth the effort to overcome her current difficulties.
She needs clear guidance about all measures needed for treatment, and how to continue breastfeeding or expressing milk from the affected breast. She will need follow up to give continuing support and guidance until she has recovered fully.
EFFECTIVE MILK REMOVAL
This is the most essential part of treatment. Antibiotics and symptomatic treatment may make a woman feel better temporarily, but unless milk removal is improved, the condition may become worse or relapse despite the antibiotics.
ANTIBIOTIC THERAPY
Antibiotic treatment is indicated if either:
- cell and bacterial colony counts and culture are available and indicate infection, or
- symptoms are severe from the beginning, or
- a nipple fissure is visible, or
- symptoms do not improve after 12-24 hours of improved milk removal.
An appropriate antibiotic must be used. To be effective against Staphylococcus aureus a b-lactamase resistant antibiotic is needed. For gram-negative organisms, cephalexin or amoxicillin may be the most appropriate. If possible, milk from the affected breast should be cultured and the antibiotic sensitivity of the bacteria determined.
The chosen antibiotic must be given for an adequate length of time. 50-14 days is now recommended by most authorities. Shorter courses are associated with a higher incidence of relapse.
SYMPTOMATIC TREATMENT
Pain should be treated with an analgesic. Ibuprofen is considered the most effective, and it may help to reduce inflammation as well as pain. Paracetamol is an appropriate alternative.
Rest is considered essential and should be in bed if possible. As well as helping the woman herself, resting in bed with the infant is a useful way to increase the frequency of breastfeeds, and may thus improve milk removal.
Other measures which are recommended are the application of warm packs to the breast, which both relieves pain and helps the milk to flow; and ensuring that the woman drinks sufficient fluids.
Other Therapeutic Approaches
A number of other forms of treatment of mastitis are sometimes suggested, but there is little evidence of their effectiveness.
Breast Abscess
SURGICAL TREATMENT
If an abscess has formed, the pus must be removed. This can be done by incision and drainage, which usually requires general anesthesia, but it can also be done by aspiration, guided by ultrasound, if available. Ultrasound is a useful diagnostic tool for breast abscess, and a thoroughly performed, ultrasound guided aspiration of the pus may be curative. It is less painful and mutilating than incision and drainage, and can be done under local anesthesia, often as an outpatient.
Systemic treatment with antibiotics appropriate to the organisms' sensitivity is usually required in addition. However, antibiotics alone, without removal of pus, are unlikely to be of value. An abscess wall creates a barrier that protects the pathogenic bacteria from the body's defenses, and makes it impossible to achieve effective antibiotic levels in the infected tissue.
SUPPORT OF BREASTFEEDING
Whether breastfeeding continues or stops after an episode of mastitis or breast abscess, and how long it continues, depends partly on the counseling and help that a mother receives. If she is given adequate guidance and clinical and emotional support, she should recover fully, and experience no problems with subsequent lactations. If she receives poor guidance and support, she may never breastfeed again. However, if an abscess is extensive, and treatment delayed, the breast may not return to full milk production.
Safety of continuing to breastfeed
Maintaining lactation when a woman has mastitis or breast abscess is important both for her own recovery, and for her infant's health.
Stopping breastfeeding during an attack of mastitis does not help the mother to recover; on the contrary, there is a risk that it can make her condition worse.
Risk of infection to the infant
Many health workers are concerned about a possible risk of infection to the infant, especially if the milk appears to contain pus. They recommend manual expression, and discarding of the miik. However a number of studies have demonstrated that continuing to breastfeed is generally safe, even in the presence of S. aureus. Only if a mother is HIV-positive is it necessary for her infant to stop feeding from the affected breast until it has recovered.
Long term outcome
With timely, appropriate and adequate treatment of mastitis and breast abscess, recovery should be complete, and normal function of the breast can usually be expected with subsequent lactations.
However, delayed, inappropriate or inadequate treatment may result in relapse, more extensive lesions and even permanent tissue damage. Repeated episodes of mastitis may give rise to chronic inflammation and irreversible distortion of the breast.
Breast abscess may compromise future lactation in about 10% of affected women. A large abscess may require extensive resection of breast tissue which can result in disfigurement and sometimes a functional mastectomy.
Conclusion
Mastitis and breast abscess are common and largely preventable conditions, which occur in all populations and which put breastfeeding at risk. They are caused primariiy by inefficient removal of breast milk, but also by bacterial infection, which is probably secondary to rnilk stasis. Particularly virulent strains of bacteria may cause epidemics of puerperal mastitis in hospitals, when infants are kept in nurseries away from their mothers.
Improved breastfeeding practices, including early skin-to-skin contact between mother and infant, rooming-in, skilled help to ensure that an infant is well attached at the breast, and unrestricted and exclusive breastfeeding, are an efficient way to prevent both milk stasis and spread of infection. Health workers and the community as a whole need to understand this, in order to support women in the best practices.
Mothers need to know how to recognise early signs of mastitis, milk stasis and blocked ducts, what they can do at home to treat them and to prevent the condition from becoming worse. They need to know when to seek skilled help for the condition, and it is important that health workers or breastfeeding counsellors are available who understand the condition, and who can give appropriate and adequate help. Whenever possible breastfeeding should continue, both to improve milk removal and to help the condition to resolve, and for the benefit of the infant. If present, bacterial or other infection should be treated with an appropriate anti-microbial agent, but this should be in addition to, and not an alternative to techniques which ensure efficient removal of milk.
TESTS
1. Therapy of acute serous mastitis includes which of the following:
1. Incision.
2. Prevention of lactostasis.
3. Fixing the breast with scarf bandage.
4. Antibiotics.
5. Retromammary novocain block with antibiotics and proteolytic enzymes.
Choose the right combination of answers:
A. 1. B. 1, 2, 3. С. 3, 4, 5. D. 2, 3, 4, 5. E. 1, 2, 3, 4, 5.
2. The preferable direction and site of incision when opening retromammary abscess should be:
A. Radial; the upper quadrant of the breast.
B. Semi-oval; the lower edge of the breast.
C. Radial; the lower half of the breast.
D. Semi-oval; the upper edge of the breast.
E. Circular; around the nipple.
Choose the correct answer.
3. The clinical signs of axillary hydradenitis are as follows:
1. Dense painful node.
2. Follicular pustule.
3. Creamy pus.
4. Necrotic centre.
5. Dense infiltrate.
Choose the right combination of answers:
A. 1, 2, 5. B. 2, 3, 4. С. 2, 3, 5. D. 3, 4, 5. E. 1,3, 5.
4. Rettomammary abscess arises from –
a) Tuberculous rib
b) Infected hematoma
c) Chronic empyema
d) All of the above
5. Acute mastitis commonly occurs during -
a) Pregnancy
b) Puberty
c) Lactation
d) Infancy
ANSWERS: 1 - D, 2 - B, 3 - E, 4 - D, 5 - C
References
Gostischev V. K. General surgery / The manual. – M.: GEOTAR-MED, 2003. – Charter XI. – P.150-191.
Moukonin A.A., Golub A.V. Soft tissue infection: Textbook for foreign students. – Smolensk: Smolensk State Medical Academy, General Surgery Department. – 2005. – 9p.
Moukonin A.A., Golub A.V. Mastitis: Textbook for foreign students. – Smolensk: Smolensk State Medical Academy, General Surgery Department. – 2005. – 10p.
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
INFECTIONS OF THE WEB SPACE AND DEEP FASCIAL SPACE IN THE HAND AND THE FOOT. FASCIAL PIROGOV-PARON’S SPACE INFECTION
Составитель доцент Ю.И.Ломаченко
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
UNIT: SURGICAL INFECTIONS
Theme: INFECTIONS OF THE WEB SPACE AND DEEP FASCIAL SPACE IN THE HAND AND THE FOOT
KEY QUESTIONS FOR HOMEWORK:
Classification of phlegmon in palmar and dorsal hand infections.
Definition of phlegmon in palmar and dorsal hand infections.
Stages of the inflammation.
The agents of infection.
Local and general symptoms of hand phlegmon.
Infections of the subcutaneous tissues of the palm.
Thenar phlegmon.
Phlegmon of the hypothenar.
Commissural phlegmon.
Phlegmons of the mid palmar space.
Crossed or U-form phlegmon.
Subcutaneous phlegmon of the dorsum of the hand.
Subaponeurotic phlegmon of the dorsum of the hand.
Management of hand phlegmon.
Infections in the foot.
Principles of antimicrobial treatment.
Specific wound infections.
Classification of phlegmon in palmar and dorsal hand infections.
Suppurative diseases of the subcutaneous tissues: interphalangeal (commissural) phlegmon; supraaponeurotic phlegmon of the palm.
Suppurative diseases of the fascial and interstitial spaces: phlegmon of the mid palmar space; thenar phlegmon; hypothenar phlegmon; U-form phlegmon.
Suppurative diseases of the dorsal aspect (dorsum) of the hand: subcutaneous phlegmon, subaponeurotic phlegmon.
Definition.
The subaponeurotic space is an area beneath the extensor tendon on the dorsum of the hand and is dorsal to the interossei fascia.
Thenar phlegmon (thenar space abscesses) develop in the space palmar to the adductor pollicis muscle fascia and deep to the level of the FDS and FDP tendons of the index finger. These infections extend ulnarward to the fascial septum, connecting the third metacarpal to the palmar fascia.
The hypothenar space is bounded radially by the fascial septum connecting the palmar fascia to the fifth metacarpal and the fascia of the hypothenar muscles ulnarly.
The midpalmar space is located palmar to the third, fourth, and fifth metacarpals and below or dorsal to the flexor tendons of these fingers.
Fig. Topography of phlegmon in palmar and dorsal hand infections: 1 – subcutaneous; 2 – palmar supratendinous; 3 – subtendinous; 4 – thenar; 5 – hypothenar; 6 – dorsal subcutaneous; 7 – dorsal subfascial.
3. Phlegmon starts with the development of serous infiltration of the fatty layer (the initial stage of the inflammation - serous-infiltrating stage). The exudate quickly assumes a suppurative nature, areas of necrosis art formed, which later join together. Necrosis and the fatty dissolution lead to the formation of a phlegmonic abscess (the suppurative stage of the inflammation - purulent-necrotic stage).
4. The agents of infection are normally staphylococci in the form of a monoculture or in association with other microbes – E. Coli, proteus, streptococcus, bacterioides etc. The infectious agents normally enter the organism from outside. The development of acute pyogenic infections is preceded by minor skin injuries.
5. The clinical manifestations are comprised of local and general symptoms.
The local signs of hand phlegmon are: tissue oedema and hyperemia, hand dysfunction, increase in the local temperature and tenderness on palpation. Foci with the involvement of skin in the inflammatory process are characterized by the classical signs of inflammation – redness (rubor), caused by peristatic hyperemia, edema, swelling (tumor), pain (dolor), increase in local temperature (calor) and organ function disorder (functio laesa). The spread and manifestation of the inflammatory process determine the extent of the local clinical presentation. The local clinical signs of progressive suppuration are: zones or stripes of redness in the skin (lymphangitis), firm tender strings of induration along the superficial veins (thrombophlebitis), the appearance of firm tender indurations at the sites of the regional lymph nodes (lymphadenitis). There is always a correlation between the extent of the local presentation and the intensity of general clinical signs of intoxication: a progression of the inflammatory process is accompanied by the progress of both local and general signs of inflammation and intoxication.
The body's response to the inflammatory process is shown clinically as follows: a rise in body temperature, chills, agitation or alternatively weakness, and extreme cases mental confusion, sometimes unconsciousness, headaches, general malaise, fatigue, rapid pulse, extreme deviations in the blood picture, signs of liver and kidney function disorder.
6. Infections of the subcutaneous tissues of the palm are only associated with tenderness on palpation and some amount of smoothening of the palmar folds. Other signs of inflammation (hyperemia, pronounced oedema) are more prominent at the dorsum.
7. Thenar phlegmon (phlegmon of the ball of thumb – thenar eminence). This is accompanied by an extreme oedema of the thenar and the radial end of the dorsum of the hand. Severe pain on palpation, tense tissues, limitations in the mobility of the oedematous thenar tissues, smoothening of the palmar folds are all characteristic symptoms of thenar phlegmon. The purulent exudates can sometimes also spread along the first interosteal muscles on the dorsum. In other cases the connective tissue barriers that divide the thenar from the mid palmar space disintegrate as a result of the suppurative process causing phlegmon of the mid palmar cavity.
8. Phlegmon of the hypothenar is often accompanied by mild intoxication. Minimal oedema, hyperemia and tension in the tissues, tenderness on palpation over the hypothenar and an increase in pain upon moving the little finger are the characteristic features.
9. Commissural phlegmon is localized at the distal part of the palm. The entry points of infection are usually deep skin fissures and skin callosity over the area of the 2nd-4th carpophalangeal joints of the palm. This phlegmon is also known as corn abscess. Phlegmons are associated with extreme pain, oedema on both sides of the hand. Fingers adjacent to the area of infection are somewhat spread apart and bent in their interphalangeal joints; extension is painful as a result of the tension on the inflamed palmar aponeurosis. It is possible for the pus to spread directly through the oval fissure of the aponeurosis to the dorsal surface of the hand, involving in the process the tendons of the deep flexors, which are situated very closely. The spread of infection can also occur in the proximal direction along the canals of the vermiform muscles, involving in the inflammation process the mid palmar space.
10. Phlegmons of the mid palmar space are associated with the accumulation of pus in between the palmar aponeurosis and the thin fascial sheath covering tendons of the flexor digitorium or between the fascia covering the palmar sides of the interosteal muscles and the posterior surface of the tendons of the long flexor digitorium. The disease is accompanied by pronounced intoxication, high body temperature, headache, as well as changes in the peripheral blood picture. Phlegmons of the mid palmar space are diagnosed clinically by pain, tenderness, and loss of the normal concavity of the palmar aspect of the hand.
Examination of the hand reveals a swelling in the central palmar area, the skin is tense, skin folds are smooth and fluctuation is not possible to elicit. Palpation over the inflamed region may cause extreme pain. The whole hand is swollen and the palm intensely tender.The dorsum of the hand is very oedematous. The 2nd-5th fingers are slightly bent in the interpha-langeal joints, attempts at passive or active movement cause extreme stretching of the inflamed palmar aponeurosis, which results in pain increase. Delayed or irrational treatment of mid palmar space phlegmon may entail a complication with the abscess bursting into the thenar fissure and the pus spreading along the canals of the vermiform muscles on the dorsum.
11. Crossed or U-form phlegmon is the most severe form of suppurative hand inflammation. The disease results from a purulent tendovaginitis of the 1st or 5th finger with a spread of the purulent exudates to radial and ulna synovial sacs.
U-form phlegmon is accompanied by pronounced intoxication, high body temperature, headache, as well as body weakness. The hand is oedematous, bluish-violet in colour and palpation is extremely tender. The fingers are bent towards the palm, active movement is absent. Attempts at passive movement may cause extreme pain. By means of palpation the area of extreme tenderness is found to be around the projections of the 1st and 5th tendons and in the proximal parts of the hand, that is. at the site of the blunt ends of the radius and ulna synovial sacs. When the pus bursts into Pirogoff’s space, diffuse tenderness and oedema of the distal parts of the forearm may result. The suppurative inflammatory process can spread to the mid palmar space, fissures of the thenar or hypothenar in the case of tenobursitis of the 1st and 5th fingers. Subsequently the pus spreads through the canals of the vermiform muscles to the dorsum of the hand to form an extensive purulent-necrotic area.
Even with favourable resolution of U-type phlegmon the distant postoperative period is associated with limitations in the functions of the hand. Hence, it is very important to have a timely diagnosis and surgical treatment of this condition.
12. In subcutaneous phlegmon of the dorsum of the hand tissue oedema and hyperemia are of diffuse nature, and it is difficult to determine the demarcation line of the infection. Thorough palpation can help to assess the area of tissue softening. Subcutaneous phlegmon occurs, as a rule, secondary to damage to the skin covering of the dorsum of the hand.
13. Subaponeurotic phlegmon of the dorsum of the hand occurs as a result of infection penetrating deep under the aponeurosis in the case of stab wounds. In this kind of phlegmon a firm induration is observed which is associated with oedema and hyperemia of the dorsum. In suppurative affection of the palm there can be transmission of the infection to the dorsum through the lymphatic vessels or through the canals of the vermiform muscles. In such situations oedema of the dorsum that is normally present in palmar lesions is accompanied by skin hyperemia, and the appearance of a diffusely tender area on palpation.
14. Management of phlegmon is surgical. Surgical incision and drainage are indicated, taking care to avoid injury to the neurovascular structures.
Anaesthesia. Many procedures on the wrist and hand can be performed using local anaesthesia either proximally (scalene block, axillary block) or more distally (Bier's block, wrist block). In general, if a tourniquet is used for more than about 20 minutes it becomes uncomfortable and so a proximal block or general anaesthetic is preferred.
Tourniquet. The use of tourniquets dates to Roman times, but the device acquired its name from surgical application in eighteenth-century France (from tourner, meaning “to turn”). A bloodless field is essential for accurate surgery. Hand surgery is performed using an axillary or forearm pneumatic tourniquet. A well-padded tourniquet above the elbow, inflated to 75 mmHg pressure over the systolic blood pressure, is usually satisfactory. In the absence of proximal anesthetic blockade, the maximum tourniquet time a patient will tolerate is 30-60 min. Except in the presence of infections, the arm should be exsanguinated before tourniquet inflation; limb elevation may be used for partial exsanguination.
Incisions which cross a flexion crease may produce an uncomfortable and restrictive contracture. Therefore, surgical incisions should be planned to lie in neutral areas. Skin incisions can be linear, curved, or angled. They may be oriented in a longitudinal or transverse direction relative to the limb. Ideally, elective wounds are placed to lie in and about the soft tissue skin creases. Hand incisions are not made perpendicular to joint creases so that iatrogenic contracture and unsightly scars are prevented.
Microbiological analysis has the potential not only to isolate the causative agent, its pathogenic properties but also to determine the microorganism’s sensitivity to the antibacterial preparations.
The dressing and splint are frequently as important to the outcome as the operation. The generic position for hand immobilization includes splinting the wrist at about 30 degrees of extension, the MP joints at 70 degrees of flexion, and the IP joints at 0–5 degrees of flexion.
Subaponeurotic phlegmon of the dorsum of the hand. Incision and drainage can be carried out by a longitudinal incision between the extensor tendons.
Hypothenar phlegmon is drained by a longitudinal incision over the palmar aspect of the hypothenar eminence.
Thenar phlegmon is drained by a longitudinal incision over the palmar aspect of the thenar eminence.
One must obey the following three principles that the hand can function properly:
1. Elevation. The hand must be elevated in a high sling or roller towel, care being taken that the venous drainage is not occluded by too much elbow flexion.
2. Splintage. The wrist should be splinted initially in the position of safety — the ‘Edinburgh’ position described by James. Dressings must not be too tight.
3. Movement. As many joints as possible of the wrist and hand should be moved as early as possible. Rehabilitation should be planned so that the fewest possible joints and tendons are immobilized.
1,2- dissection of thenar phlegmon;
3 – dissection of the palmar space.
The projection of the palmar space is dotted.
15. Infections in the foot.
Infections in the foot can be considered to be minor and common, or major and fortunately rarer. With a significant proportion of the world's population remaining barefoot, minor skin trauma is a frequent cause of local infection. In the shod population poor shoe fitting has the same effect. The increased incidence of diabetes means that this is now a potent cause of major infections. With the combination of vascular insufficiency, neuropathy and poor cellular function, infection due to diabetes can be extremely difficult to treat.
A careful history and examination must be aimed at elucidating predisposing factors, assessing the extent of the infection, including evidence of more generalised spread. Even with relatively minor bacterial infections lymphatic spread is not uncommon. This leads to lymphangitis and involvement of regional lymph nodes. Investigations must be aimed at establishing the extent of the infection, the nature of the organism involved and any increased risk factors such as poor peripheral blood supply or diabetes. Wound swabs, culture of discharged material and skin scrapings or nail clippings can be helpful in identifying the organism. A full blood count, plasma viscosity, blood sugar and blood cultures can be helpful in determining the exact diagnosis and monitoring the benefit of treatment. Plain X-rays remain the baseline investigation of deeper infection, but newer investigation modalities such as magnetic resonance imaging (MRI) can give extremely helpful information on the deeper spread of infection and particularly address the issue of soft-tissue spread.
Basic principles of management involve rest, elevation, antibiotics and, where necessary, surgical debridement. Regular dressings are needed. Desloughing agents and dressings which keep the recovering granulation tissue moist are important.
Deeper infection may involve soft tissues only with abscess formation or can involve bones (osteitis or osteomyelitis). This type of infection can also involve localjoints (pyogenic arthritis). Any form of abscess needs to be drained urgently and the deeper tissues thoroughly debrided. If tissues are clearly not viable then an appropriate amputation should be planned. This should be undertaken at a level where there is a realistic chance of the wound healing.
Principles of antimicrobial treatment.
The use of antibiotics for established infection in wounds ideally requires the isolation of the bacterium and a determination of its sensitivity; this is the overriding first requirement, for after antibiotics are administered, the clinical picture may be confused, the patient no better, and the opportunity to make a precise diagnosis has been lost. However, it is unusual to have to treat wound infections with antibiotics. Only spreading infection or signs of systemic sepsis really justify them. Appropriate treatment must include drainage of pus and debridement if necessary.Presented with pus, or other material draining from a wound, the microbiologist can isolate the causative organisms and this may guide therapy. There are two approaches to treatment:
the use of a narrow-spectrum antibiotic to treat a known sensitive infection;
the use of broad-spectrum antibiotic combinations where the organism is not known or where it is suspected that there may be one, two or more, usually gut-derived bacteria responsible for the infection acting in synergy.
Alternatives are a cephalosporin, e.g. cefuroxime, with metronidazole (increasingly popular as gentamicin toxicity and monitoring of bevels are avoided), or monotherapy using a carbapenem or quinolone.
In surgical units with multiple resistant Pseudomonas or other Gram-negative species (such as Klebsiella) which have become ‘resident opportunists’, there may become a need for a rotation of antipseudornonal and anti-Gram-negative chemotherapy between the broad-spectrum penicibbins, e.g. azbocilbin 2 g i.v. 8-hourly and cephabosporins, e.g. ceftazidime 50-100 mg/kg per day, or cefotaxime 2 g 8-hourly.
The use of these routines, the monitoring of subsequent wound infection and the alternation of combinations of chemotherapy should be monitored by the infection control team. It should not be forgotten, in treating postoperative pyrexial infection, that a failure to respond to a very broad spectrum of these combined antibiotics requires a critical bedside review to exclude collections of pus and other causes of a raised temperature.
17. Specific wound infections.
Gas gangrene is caused by C. perfringens. The Gram-positive, spore-bearing bacilli are widely found in nature, particularly soil and faeces. Patients who are immunocompromised, diabetic or have malignant disease are at risk, particularly when anaerobic wound conditions are present with necrotic or foreign material. Wound infections are associated with severe local wound pain and crepitus (gas in the tissues which may also be noted on plain radiographs). The wound presents a thin, brown, sweet-smelling exudate, from which bacteria can be recognised on Gram staining. Oedema and spreading gangrene follow the release of collagenase, hyaburonidase, other proteases and a-toxin. Systemic complications with circulatory collapse and MSOF supersede without appropriate intervention. Patients are almost always immunocompromised.
Basic principles of management: 1) prophylaxis in patients at risk; 2) once established, barge doses of intravenous penicillin and aggressive debridement of affected tissues are required; 3) the use of hyperbaric oxygen.
TESTS
1. The cross (V-form) hand phlegmon is characterized by the following clinical signs:
1. Tenderness.
2. Hand dysfunction.
3. Localization of suppurative exudate in proximal area of the palm.
4. Localization of suppurative exudate in the distal areas of the palm.
5. Extensive contracture of fingers.
Choose the right combination of answers:
A. 1,2, 3. B. 1,2, 4. C. 2, 3,4. D. 1,2, 4, 5. E. 1,2, 3,5.
2. The local signs of middle space phlegmon are as follows:
1. Tension of the skin being in the centre of the palm.
2. Fluctuation.
3. Tenderness.
4. Swelling of the dorsal hand surface.
5. Finger flexion.
Choose the right combination of answers:
A. 1.2. B. 1,4. C. 1,3, 5. D. 1,3,4. E. 1,3,4, 5.
CLUES
A
E
ГОУ ВПО «Смоленская государственная медицинская академия
Федерального агентства по здравоохранению и социальному развитию»
МЕТОДИЧЕСКИЕ УКАЗАНИЯ ДЛЯ СТУДЕНТОВ
ПО ДИСЦИПЛИНЕ хирургические болезни
OSTEOARTHRITIS, ARTHRITIS, SYNOVITIS, GANGLION CYST. OSTEOCHONDROPATHIES: Osgood-Schlatter’s disease, Sheuermann-Mau’s disease, Legg-Calve-Pertes’ disease, Kienböck’s disease, Köhler’s-I and Köhler’s-II diseases. (Etiology, classification, clinical features, diagnostics, treatment)
Составитель: ассистент О.Г.Шахбазян
Методические указания утверждены на методическом совещании кафедры госпитальной хирургии (протокол № 2 от 6 октября 2008 г.)
Зав. кафедрой______________(проф. С.А.Касумьян)
2008 г.
Arthritis
2.1Arthritis - inflammatory disease of a joint
For an arthritis pains in a joint are characteristic, especially at movement, quite often there are restrictions of its mobility, the swelling, change of the form, sometimes a skin above a joint reddens and fever. Meet arthritis of one joint (monoarthritis) and many (polyarthritis). The arthritis can begin at once and be accompanied by strong pains in a joint (acut arthritis) or to develop gradually (a chronic arthritis). The reasons of arthritises: an infection, a trauma, an allergy, infringement of a metabolism, disease of nervous system, lack of vitamins.
2.2The reasons of development of an arthritis
The reason of development of arthritises can be bacteriemic, virus or fungoid infections of joints. Penetration of an infection into joints is usual occurs through vascular system from other part of an organism, it can occur at a trauma, a surgical intervention.
2.3Symptoms of an arthritis
Symptoms of an infectious arthritis are reddening, a swelling, sensation hurt at pressing, the general symptoms of an infectious disease - rise in temperature of a body, a fever, a pain in all body are often observed.
The arthritis can suddenly arise or gradually develop. At some people it is observed sharp ноющая or a dull ache. This pain as a dentagra. Movement in this joint is usually broken, though is sometimes observed stiffnes.
2.4Kinds of an arthritis
Depending on character of lesion the basic types of arthritises unite in two classes: an inflammatory arthritis and a degenerate arthritis.
To inflammatory arthritises concern:
Infective arthritis
Rheumatoid arthritis
Podagra
They are connected with an inflammation synovial environments - a thin film of the connecting tissue covering a joint from within.
To degenerate arthritises (osteoarthritis) concern:
1) osteoarthrosis;
2) A traumatic arthritis.
These diseases are connected with damage of the articulate cartilage covering the ends of bones in a place of their joint.
Osteoarthritis - the most widespread kind of arthritis. It is usually connected with ageing joints or the traumas which are taken place in the past. Often it proceeds nonsympthoms, is sometimes observed painful sensations and restrictions of mobility in joints. As a rule, osteoarthritis does not lead to serious consequences though at some people it is accompanied by a strong pain with restriction of physical opportunities. In rare cases osteoarthritis reaches a stage when walking becomes inconvenient.
Osteoarthritis is one of the most frequent reasons of physical inability at older persons. At 10 % of persons 55 years are more senior is diagnosed osteoarthritis than knee joints, and a quarter from them are deep invalids.
Intraarticulate introduction of glucocorticoids is the most widespread method of treatment osteoarthritis knee joints.
2.5Reactive arthritis
The name - speaks reactive arthritis, that these diseases are reaction to something, in this case on other diseases. Reactive arthritises are group of diseases of the joints connected with an infection. Thus the infection plays a role only the starting factor, the microbe-activator in joints is not present, the arthritis is a reaction of an organism to a microbe.
Reactive arthritis arises simultaneously or after various enough frequent, but quite good-quality infectious diseases. These are virus or bacteriemic infections of a nasopharynx, urinary tracts and genitals, a gastrointestinal tract.
Displays of reactive arthritis can be various. The patient tells, that 1-3 weeks prior to occurrence of articulate changes has transferred ARD, intestinal frustration or was speeded up and urodynia. The arthritis begins sharply, the temperature raises, the general condition worsens. Large joints of the bottom extremities - knee, talocrural, calcaneal, metatarsusphalanx and interphalanx, less often joints of hands are amazed. The arthritis begins with one joint is more often, and further within 1-2 weeks pathological process extends on other joints. Joints swell up a little. Pains very strong, function of joints is limited. Pains in a backbone are often marked.
Treatment of reactive arthritis is spent in three directions. The program of such treatment is defined by the doctor-expert.
The first direction - treatment of the center of infection. At arthritis’s on a background of diseases urinary and sexual systems treatment by antibiotics tetracicline groups - within 4-6 weeks, and also local treatment - massage of prostate is shown at prostatitis. At sick by arthritis’s after intestinal infections are applied levomycetin, gentamycin, which rates is shorter. Application sulfasalazin recently is recommended.
The second direction - suppression of activity of inflammatory process in joints. Preparations of the first of some - all spectrum of not steroid resolvents. In heavy cases and at insufficient efficiency NAIA apply hormones of a bark of adrenal glands intraarticulation and inside.
The third direction - rehabilitation which is spent usually after decrease acute displays of disease and is directed on restoration of functions of the amazed joints. Here the major importance is given to physiotherapy exercises, a physiotherapy and sanatorium treatment (a fangotherapy, hydrosulphuric baths, dirts, etc.).
The basic criteria of the differential diagnosis periarthritis, arthritis and arthrosis
Attributes |
Periarthritis (a dystrophic genesis) |
Arthritis |
Arthrosis (without sinovitis) |
Pains |
Only at is certain-the movements |
The spontaneous pains amplifying at movements |
Pains at any movements, spontaneous pains are absent |
Swelling |
Less painful, limited |
Morbid, diffuse |
No |
Deformation of a joint |
No |
More or less due to change of soft parts |
Expressed due to osteal growths |
Morbidity at palpation |
Local |
Diffuse, expressed |
Is absent or is poorly expressed |
Local above temperature |
Is absent or is poorly expressed |
It is expressed |
No |
Passive movements extremities |
In full |
Are limited |
In full or are poorly limited |
Active movements in a joint |
Are a little bit limited |
Are limited |
In full or are poorly limited |
Laboratory parameters of blood |
Normal |
Accelerated СОЭ, elevation level of a fibrinogen, ceromukoid, |
Normal |
Roentgenography of joints |
Sometimes calcyficates and periosthitis |
Narrowing of an articulate crack, bony rarefication epiphyses, erosion of articulate surfaces |
Narrowing of an articulate crack, subchondrial osteosclerosis, osteofites. |
2.6Arthrosis knee joint
Arthrosis knee joint the leading place in group arthroses lesions of joints of extremities belongs. Patients with arthrosis a knee joint constantly prevail among the patients visiting out-patient departments, but, unfortunately, it is not enough of them among those who is treated in our hospitals. Treatment in stationary conditions could give where greater effect, rather than out-patient therapy "on the job". Known to doctors more than 100 years this disease in a life carries the name " adjournment of salts".
Actually arthrosis can meet calcify (adjournment of salts of calcium) in soft parts of a knee - the copular device, places of an attachment of sinews, etc., but these calcify have the limited character and have no, as a rule, independent clinical value. On the foreground at gonarthrosis is degenerate-dystrophic process in gialine cartilage covering condyle of femoral and tibial bones acts. And pathological process begins with infringement of a circulation in fine osteal vessels after which there are changes in a cartilaginous integument of a joint.
Primary arthrosis knee joint develops on a usual vital background. People of advanced age, women more often, than men suffer. To development arthrosis knee joint people with the raised weight of a body, adiposity are obviously located. Secondary артроз a knee joint has in the basis a trauma of a knee joint (intraarticulate crisis of a hip and a tibial bone, damage of meniscuses, gemarthrosis) or the transferred disease (an arthritis various etiology, chondromatosis of joints, " the articulate mouse ", etc.). Duly adequate treatment of the listed processes can interfere with occurrence and development gonarthrosis. Complaints of the patient with arthrosis knee joint in the beginning are reduced to sensation of the certain constraint in a joint, to "tightening" under a knee, to pains in it after long walking. The majority of patients complains also of difficulties at walking in the mornings, after a dream or after more or less long sitting. " You miss, - it becomes easier ", - they mark. Eventually disease progresses, pains become persistent, constant, intensive; the pain is more often localized on the internal party of a knee. Many patients feel a crunch at movements in a knee joint. Restriction of bending and (or) extension gradually develops. The lameness Eventually progresses. In heavy cases of patients cannot move without assistance at all or without a support on a back of a chair, crutches, etc. In lying position the pain ceases, but sometimes patients suffer from Pains an datnight.
Survey of a knee joint in an initial stage of disease does not find out external changes. In the further it is possible to note deformation of a knee, rough contours of the bones forming a joint, contracture (incomplete extension or bending) and a curvature of an axis of a shin, as a rule, medialis. If to put a palm on a forward surface of a knee at flexion-extension movements investigating will feel a crunch in a knee joint of various intensity and duration. The same sensation of a crunch can be received, shifting patella lateral and medial in a cross-section direction (positive patella -condylar symptom).
Palpation a joint morbid zone, more often from the interior of a joint, at a level condyles a hip, tibia and an articulate crack comes to light. Quite often in a cavity of a knee joint collects effusion, i.e. joins synovitis. This condition is defined by a smoothness of contours of a knee joint due to evaginate tissues above patella and sideways from it and sensation of fluctuation at palpation evaginate two hands. Synovitis knee joint testifies to complication arthrosis aseptic inflammatory process and then we have the basis to designate such condition of a knee joint as " arthrosis -arthritis". The temperature at arthrosis -arthritis, as a rule, does not raise also analyses of blood do not show deviations from norm.
Subjectively sick define joined synovitis as new heavy feeling in a joint, stirring to bending of a knee. Apparently from the resulted data, clinical diagnostics gonarthrosis is simple, quite accessible. However in any case the X-ray inspection is necessary. It confirms and specifies the diagnosis, establishes a degree arthrosis changes, allows to watch dynamics of process during time and, at last, the roentgenography is necessary for exception of tumoral or any other process in the bones forming a joint. In an initial stage gonarthrosis radiological changes can either be absent, or to be rather insignificant. In later terms narrowing an articulate crack, a sclerosis subchondrial zones, a point of edges femoral condyles and tibia, sometimes adjournment of salts in surrounding soft parts comes to light. Radiological inspection of elderly and old people at many of them reveals the expressed changes described above.
In a complex of treatment arthrosis knee joint the positive role is played with medical gymnastics. It is spent by patients with the purpose of prophylaxis contracture, improvements of a circulation to extremities, increases of a muscle tone. It is very important to lead the first lesson of gymnastics in the morning before to rise on legs and to start to go. The complex of exercises should be received in a cabinet of physiotherapy exercises and to carry out it 3-4 times a day; especially it is important at transition from horizontal position in vertical. After work rest laying 30-45 minutes is recommended. Semispiritus warming compresses and warm (36-36оС) baths (it is possible with needles) before a dream finish house treatment. Its carrying out entirely depends on the patient, and it is necessary to convince it of importance of punctual performance of recommendations.
Treatment of gonarthrosis various kinds of a physiotherapy (diadinamic supplement currents, phonophoresis with hidrocortzon, an electrophoresis with novocain, a ultra-violet irradiation), Laser- and magnetotherapy, massage of a leg. The sanatorium therapy which can be spent on any resort if in the list of indications to treatment there is a reference to " diseases of organs of movement " is useful.
The addicting for intraarticulate introduction hydrocortizon and other steroid hormones has given a up the place to the weighed approach to treatment. To hormonal therapy competes, and in some cases and supplements its method of an intraarticulate oxygenotherapy. It consists in introduction in a cavity of a knee joint of gaseous medical oxygen. Correct treatment of intraarticulate crises, removal of the damaged meniscuses, restoration broken off ligament, removal of " the articulate mouse " are simultaneously prophylaxis gonarthrosis. However and at developing arthrosis because of these processes operative treatment can suspend development arthrosis and is essential facilitate a condition of the patient.
Medicamental treatment gonarthrosis, despite of universal application, posesses rather modest role. The decision of a problem arthrosis knee joint in the certain degree depends on its prophylaxis. A reasonable combination of work and rest, employment by the physical culture, allowing long years to keep a tone of vascular and muscular systems, dont increases in weight of a body, the duly reference behind the qualified help - here major factors of prophylaxis deforming arthrosis knee joint.
Arthrosis hip joint
Arthrosis hip joint (coxarthrosis) - very artful pathology often masking under other disease. At early stages coxarthrosis appears only aching pain. Quite often sick coxarthrosis assiduously treats knees, a back pain or platypodia, accordingly, the diagnosis is put already when there is more expressed semiology, for example infringement of mobility of a joint. Coxarthrosis amazes women of able-bodied age (from 25 till 55 years) more often and leads early disability. It is necessary to note, that this disease is successfully enough treated at early stages, including chondroprotectors. The reasons:
Exogenous
•heavy physical work •rise weights •shok loading on a joint at employment by the certain kinds of sports (track and field athletics, art gymnastics, some kinds of aerobics)
Endogenous
•disorder circulations in a joint •some accompanying diseases (an atherosclerosis of vessels, chronic venous insufficiency, superfluous weight of a body and adiposity, arthritises) •disorder metabolism •congenital anomalies of joint
Stages coxarthrosis
The first stage |
The second stage |
The third stage |
Character hurt |
||
The pain in a joint arises after physical activity |
The pain disturbs not only at physical activity, but also in rest |
The pain has constant character, disturbs even at night |
Infringements of mobility of a joint |
||
Lamenesses practically it is not observed, movements are not limited |
After physical activity there is a lameness. Movements are limited, it is heavy to set aside a leg aside, to tighten a leg to a breast, to put on footwear. Reduction of volumes of a sick leg due to an atrophy of muscles is observed |
To go without a cane or crutches it is impossible. Muscles of a shin and a hip it is acute atrophy, the sick leg becomes shorter healthy |
Character of changes on the roentgenogram |
||
Non-uniform narrowing of an articulate crack, osteal growths (osteophitis) in a joint in the form of a small nimbus |
The head of a femur is displaced upwards, cervix of heads thickening and is expanded. Extensive osteophitis. The articulate crack is acute narrowed (in some times in comparison with norm) |
Extensive osteal growths both in cotyle, and on a head of a femur. The articulate crack practically is not visible |
Treatment
NAIA
Ointments with irritating and warming effect
Periarticular injections of corticosteroids (dyprospan, cenalog)
Vasodilating (pentoxyphyllini, xantinola nycotinat)
Miorelaxanting (mydocarm, sirdalud)
Chondroprotectors per os: a preparation “Stopartrosis”, compensating for the deficiency glyucosamini sulfate. Glyucosamini sulfate is natural, plays the important role in development and deduction of an intraarticulate liquid which lack leads to illnesses of joints, plays the important role in biochemical processes in cartilage.
Periarticular injections chondroprotectors: a preparation “Alphutop”, possessing chondroprotection, antiinflammatory, analgesic, regenerative, trophic activity.
Manipulation (is more effective on I and II stages)
Physiotherapy exercises
Extension of a hip joint (an equipment room traction)
A postisometric relaxation (on I and II stages)
Operative treatment - at III stage of disease (implantation of an artificial joint) in case other actions do not give desirable effect
Osteochondropathies
In group osteohondropaty at children and teenagers are incorporated; diseases of bones and the cartilages, described original change apophyses, spongy substance short and epiphyses the long tubular bones, arising on hypovascular (avascular) to basis. However at the profound studying separate diseases of this group significant distinctions in their prevalence, etiology, a pathogenesis and clinical current are revealed.
Depending on localization of pathological process in a bone distinguish 4 subgroups osteochondropathis.
A. Osteohondropaty epiphyses the ends of tubular bones: 1) heads of a femur (Legga-Kalve-Pertes disease); 2) heads II - III metatarsus bones (Kohler's II disease); 3) the sternalis end of clavicule; 4) phalanxes of fingers of hands.
B. Osteohondropaty of short spongy bones: 1) a navicular of foot (Kohler's I disease); 2) semilunaris bones of a brush (Kinbek disease ); 3) bodies vertebra (Kalve disease); 4) sesamoid I metatarsusphalanx joint.
B. Osteohondropaty apophyses: 1) Tuberosity tibia (Osgut-Shlatter disease); 2) calcaneal tuber; 3) apophysaris rings of vertebra (Sheyerman-Mau disease, or youthful kyphosis); 4) pubic bone.
Partial osteohondropaty articulate surfaces (Kenig osteochondritis dissecans ).
At children and teenagers most often meets osteohondropaty vertebralis segments, epiphyses heads of a hip and apophyses of tibia. . Osteohondropaties other bones at children meet much less often.
OSTEOHONDROPATY THE BACKBONE
(Sheyerman-Mau disease, or youthful kyphosis)
Disease among all osteohondropaty meets most often, but at children and teenagers in connection with asymptomatic and painless current comes to light far not always. Among the children's population it makes from 0,42 % up to 37 % of cases [Sheuermann H., 1936:, Rube W., Hemmer W., 1962].
Etiology osteohondropaty a backbone remains till now unsolved. The majority of authors connect development osteohondropaty backbone with aseptic necros of apophyses bodies of vertebra which reason remains not opened.
In development osteohondropaty a backbone distinguish a level, stages and weight. Typical localization of osteohondropaty in a chest department (in 58,6 %) is peculiar to process; less often Sheyerman-Mau disease meets in lumbar-chest (in 18,2 %) and lumbar departments (in 17,8 %), and at 5,4 % of children it happens widespread. In a cervical department disease meets seldom.
In current osteohondropaty distinguish three stages depending on age. However, considering, that cardinal attributes of osteohondropaty appear with approach ossiphication apophyses bodies vertebra and disappear or decrease after them sinostosis with bodies, it is expedient I a stage, initial, to consider as arising in stages of a unripe backbone, II stage blossoming, as shown in the beginning ossiphication apophyses bodies vertebra and intensive growth of a backbone, III stage finishing, as corresponding sinostosis of apophyses bodies vertebra.
Weight osteohondropaty backbone is defined by prevalence, i.e. number amazed vertebralis segments, expressiveness of cardinal attributes (weight of deformation of bodies vertebras, a degree of narrowing of disks, presence of individual and plural forward and back hernias of Shmorly), presence of pains in a backbone and secondary membrane-radicular syndrome and their expressiveness, a degree of restriction of function and decompensate backbone, defined by a deviation of the case aside and back. At children and teenagers it is allocated three degrees of weight osteohondropaty depending on expressiveness specified above attributes.
The clinical picture osteohondropaty a backbone depends on age of the child, a stage and expressiveness of pathological process.
The earliest attribute osteohondropaty is the pathological bearing, and the most typical symptom - kiphozis deformation of a backbone. However it is noted transition of a pathological bearing in kiphose. Moreover, fixed kiphose meets in 51 % of cases of Sheyerman-Mau disease, and heavy kiphose - only in 5,1 %.
Restriction of an inclination of the case forward can early be observed, a deviation of the case back and aside which distinctly come to light in a blossoming stage and in the further do not increase.
In II stage of process there is a final deformation: a backbone - kiphosis at 51 %, scoliosis - at 55,4 % of children. These deformations concern to number not progressing. Heavy forms kiphosis and a scoliosis meet no more than at 5 % of children. At 15 % of children with osteohondropaty a backbone the flat back is formed, and physiological bends of a backbone remain with 33,9 % within the limits of norm.
In II and III stages osteohondropaty a backbone children and teenagers quite often mark feeling of weariness in a back and a pain in a backbone, a pain in the bottom extremities; these symptoms differ weak expressiveness and instability; after night rest of the complaint usually disappear.
In I stages, but more often in II and III, come to light positive symptom of Laseg, - less often Vasserman, capsulate symptoms which are combined with restriction of an inclination of the case forward and, probably, are the reason of such restriction.
Radiological inspection provides authentic diagnostics osteohondropaty (backbone) only in II stage of process.
In I stages osteohondropaty cardinal attributes are absent, but can be available indirect. To them concern: projective narrowing of disks on the roentgenogram; unilateral rotation vertebras in chest and lumbar departments; easy cuneiform deformation vertebras at a level formed pathological kiphosis; flatten of bodies vertebras with their increase dorsoventralis size; narrowing of disks in comparison with above and below located.
OSTEOHONDROPATY HEADS of the FEMUR
(Legga-Kalve-Pertes disease)
Etiology.
The reasons of occurrence aseptic necros of epiphyses heads of a femur at children remain obscure, but infectious, traumatic, hormonal and hereditary theories continue to be discussed, however any has no convincing proofs.
Pathogenesis.
In the beginning of disease in a cavity of a hip joint the superfluous quantity of a yellowish liquid, thickening and edemas sinovial environment that testifies to presence sinovitis is found out. Bacteriological research does not certain its infectious character.
Clinical picture.
Osteohondropaty heads of a femur arises at children in the age of 5-10 years, but chances of disease at earlier and later age. As a rule, one is amazed, more often right, a joint, but thus quite often smaller degree osteohondropaty changes comes to light and in other joint which can be exposed to return development, not passing all stages. Typical bilateral process meets in 7-10 % occasional, but, as a rule, it develops not simultaneously. Boys are ill in 4-5 times more often girls.
The clinic of Pertes disease is described by many authors, but till now late diagnostics meets quite often. A principal cause of late diagnostics of disease is weak expressiveness of symptoms, the long periods of painless current after occurrence and disappearances of the first pains.
The earliest and frequent attributes of Pertes disease are the pain and a lameness. However in the certain percent of cases the pain is absent. Localization be ill changeable: at 65,9 % of patients it arises in the field of a hip joint, at 12,4 % of patients - in a knee joint, at 10,6 % in all bottom extremity. Sometimes children complain of feeling of tightening in the field of the big trochanter where the expressed, dense, limited hypostasis is defined.
The lameness in the beginning of disease can be result of a pain and contracture a joint, and later consequence of decrease in height epiphyses, an easy incomplete dislocation of a hip and weakness gluteal muscles. Most often at Pertes disease restriction of internal rotation of a hip - at 87,7-91,2 % of children, a little bit less often - restriction of external rotation of bending - at 35,9 %, reduction - at 30,9 % is observed. At 55 % of children it is formed flexion and lateral-rotational contracture.
The atrophy of muscles concerns to early and constant symptoms; it more all is appreciable in the field of gluteal muscles and muscles of a hip. In some cases on a background lymphostasis, thickenings of a skin and hypodermic it can be undistinguished. Symptom of Alexandrov, as a rule, happens positive. The expressed vegetovascular frustration which are more appreciable at unilateral process can take place. Pallor and a cold snap of foot, decrease in temperature of an extremity concern to them on 0,5-2°С, smaller expressiveness of capillary pulse in the field of fingers of foot, a wrinkled skin of a sole (a skin of the laundress), retardation biological and hydrophyl assays, asymmetry of reaction perspiration on the Minor, infringements of a circulation in all extremity in comparison with healthy, revealed at radioisotope research.
The acute beginning of Pertes disease meets in 0,4-6 % of cases, rise of temperature and inflammatory shift in blood. However and at children with usual current the temperature, increase ROE up to 23-34 mm/ю, leukocytes up to 109/л, lymphocytes up to 45-54 % is quite often observed subfibrial.
Radiological attributes. In current osteohondropaty heads of a femur at children distinguish five consistently developing stages, the are peculiar to each of which pathomorphological and radiological features. I, initial, the stage is characterized necros spongy bone epiphyses and an osteal brain, II stage - by impression crisis, III stage - a fragmentation epiphyses, IV stage - a reparation, V a stage - final restoration of a bone. The greatest difficulties in radiological diagnostics test at initial (I) stages of disease. Therefore for diagnostics of the given stage distinguish three groups of attributes: changes in soft parts (a capsule and muscles), projective changes in pelvic bones and a hip joint, direct attributes of disease.
Treatment.
Complex conservative treatment of Pertes disease provides first of all full unloading of an extremity, improvement and restoration of a circulation in the field of a hip joint and in the amazed extremity, stimulation of processes resorption necrosis an osteal tissue and processes of a new growth following it, preservation of function of a joint, maintenance of a physiological tone of muscles of an extremity and the general muscle tone. Full unloading of an extremity should be appointed immediately as soon as it is diagnosed. Unloading of an extremity warns the further decrease in height epiphyses which subsequent restoration occurs only within the limits of initial height. During treatment by any means it is impossible to increase height flatten epiphyses. With the purpose of unloading use extension by a cuff for an ankle joint, usually hardly fixed on a hip and a shin. At an atrophy of muscles and the widespread vegetovascular infringements in all extremity (first of all the expressed developments of stagnation in a venous channel) it is necessary to consider such kinds of extension irrational and even harmful. Wide application has found plaster кроватка and the deaf plaster bandage, treatment in which 3-4 month alternate everyone to functional regenerative treatment or a skeletal traction, having studied results of treatment of Pertes disease all existing methods, have found, that the best has appeared a method of fixing femurs with internal rotation and the moderate assignment. At this method the head of a femur is aligned in an articulate hollow, and the fixed assignment femurs reduces pressure upon the amazed head; at this method mobility in coxofemoralis and ankle joints also is kept. The general gymnastics for the top and bottom extremities (excepting the amazed extremity), muscles of a back and an abdominal wall start to spend with I stages and continue constantly. At this time the child active reductions gluteal and the four-chapter muscles on the sick party force to make, active movements in an ankle joint. In III stage to children allow to sit down, it spend easy passive movements in coxofemoralis and knee joints. From IV stage connect active exercises for the amazed hip joint. The specified orthopedic mode should be kept up to a stage of restoration of a head of a femur. With restoration of structure of a head and cervix, a peculiar mature bone, in a prone position use an emphasis on spring adaptations (walking laying), rotation on a stationary bicycle, an easy support on an extremity during walking па crutches. Full loading on an extremity resolve only after on two last roentgenograms made with an interval in 2-3 month after specified above preparatory treatment, the structure of a head and cervix remains to a femur constant. Loading by an extremity without crutches in the first year after the termination of treatment increase gradually, completely excepting jumps, transitions to greater distances, rise of weight, knee-bend. At this time it is rational to use walks bicycle, navigation. In the further it is necessary for persons who have transferred Pertes disease to avoid excessive loadings on a joint, regularly to spend morning gymnastics, mainly laying, completely excepting exercises of knee-bend; for them stay on the sea in summertime and navigation in pool - in winter is useful. These measures are necessary for the prevention of development early deforming arthrosis in a hip joint. Massage of the amazed extremity spend in all stages of disease with breaks on 3-4 week; it is directed first of all on elimination of developments of stagnation in lymphatic and venous systems of an extremity and improvement of an active circulation. Medicamental means in complex treatment of Pertes disease take the important place, providing first of all normalization of a circulation in the amazed extremity, stimulation of processes resorption and neogeneses. Considering prevalence of spastic type of a circulation, as vasodilators use nicotinic and Acidum ascorbinicum, no-spa, nikospan, , etc. the Greatest vasodilating effect at children it is received from nicotinic and Acidum ascorbinicum that is confirmed by a capillaroscopy. Therefore with II up to V stages it is necessary to apply the specified means, alternating them and doing breaks for 1-1,5 months During all period of treatment to children give complexes of vitamins. L.A.Smirnova (1976) with the purpose of stimulation of a bone formation applied repeated rates of an injection of vitamin В12 which, being a neurogenic stimulator, promotes normalization and vegetovascular functions; apply paraffin, ozokerite (t 35-38°С), mud applications, hot baths. However at venous stagnation that is characteristic for I stages, these means only increase developments of stagnation that is confirmed by data of a capillaroscopy. The specified thermal procedures are the most rational for appointing in a stage of a fragmentation, a reparation and final restoration. In a stage impression crisis, especially in a stage of a fragmentation, it is rational to use an aloe, electrophoresis with the preparations containing iodine that accelerates resorption necros bones, and in stages of restoration - an electrophoresis with chloride of calcium and the preparations containing phosphorus. The electrophoresis with CaI accelerates restoration of an osteal tissue, and the ultrasound activates resorption necrosis osteal tissue. All the specified medical means at children with Pertes disease apply on a background general treatments (Polyvitaminum, cod-liver oil, glyconat calcium, apilak, feed rich with fibers and vitamins). Results of conservative treatment. The general duration of conservative treatment, but to data of various authors, oscillation from 2-3 till 4-6 years.
OSTEOHONDROPATY THE TIBIAL TUBEROSITAS
(Osgut-Shlatter disease)
Disease is described for the first time in 1903 Meets quite often, amazes mainly boys in the age of 13-15 years, the strong constitution, going in for sports. Among all Osteohondropaty Osgut-Shlatter disease meets from two parties (on both legs) is more often. At microscopic research of pathological formations infringements in processes of ossification are found out. At of some teenagers of change in tibial tuberositas are combined with changes in a backbone, characteristic for osteohondropaty. These clinical supervision only confirm disontogenetic nature of these two processes. Disease arises without the visible reasons or, more often, after a trauma and the raised physical activity.
Clinical picture. Above tuberositas tibial bone there is a swelling, puffiness, a thickening and bulge a cartilage, morbidity palpation, and also at a support on a knee joint, during the moment of bending and carrying out of an extremity in anterior. In an estimation of radiological attributes of Osgut-Shlatter disease it is necessary to consider the big number of variants normal ossiphication apophyses tibial bone, its different character on the right and at the left. Therefore diagnostics base on data of clinic (a pain, a swelling) and discrepancy between significant ehvagination cartilage tuberositas and its smaller size on the roentgenogram. Process proceeds favorably and comes to an end with restoration of structure apophyses; function of a knee joint thus does not suffer. Disease should be differentiated with inphrapatellaris bursitis, osteomyelitis, a cartilaginous tumour. Treatment. Provide first of all exception of overloads; physiotherapeutic procedures are shown. Some authors resort to surgical treatment which at children it is necessary to consider inadmissible in connection with danger of damage and early synostosis apophyses region of growth therefore can develop recurvation in knee joint.
OSTEOHONDROPATY the NAVICULAR of FOOT
(Kohler I disease)
Disease for the first time is described A. Kohler in 1908 Illness meets seldom and mainly at children in the age of 8-12 years. Quite often process develops па both stops. Microscopic it is proved aseptic necros to spongy navicular and safety of a cover cartilage. Disease begins with a pain on a back surface of foot, a lameness. At a level of a navicular there is a swelling without attributes of an inflammation. Night pains are possible. Children go with a support on external edge of foot. Illness proceeds from 8-12 month till 1-2 years. The X-ray pattern in an initial stage is characterized by a bony rarefication, then reduction of a kernel of ossification of a navicular with its subsequent condensation and flattening, its fragmentation is sometimes traced. Process goes slowly and comes to an end with incomplete restoration of structure and the form of a bone. Treatment consists in unloading in plaster; apply physiotherapeutic treatment, and then an insole with an instep support.
OSTEOHONDROPATY OF THE II-III METATARSUS HEADS
(Kohler II disease)
Disease is described And. Кohler in 1920 also it is named by its name. At children meets rather seldom, mainly at persons of a female. In a basis lays aseptic necros epiphysis heads II, less often III, metatarsus and it is the extremely rare - both bones. A clinical picture. Disease arises in the age of 10 20 years. Illness begins gradually with pains at basis II-of III finger of the foot, amplifying at walking and at пальпации heads of these bones. On rear of foot the basis of a finger has a hypostasis without attributes of an inflammation. Patients go with a support on a heel, unloading a forward department of foot. The specified symptoms are kept long enough time, then gradually abate. In the late period of a pain can renew in connection with development deforming arthrosis. Roentgenology condensation and decrease in height of a head II or III metatarsus is more often comes to light; then the head gets spotty figure, the articulate crack extends. In a final stage of full restoration of structure and the form of a head usually it is not observed. Treatment. Orthopedic insole with the calculation of the longitudinal and cross-section arches that provides unloading a forward department of foot. At unsuccessfulness of conservative treatment of A.Radulesku (1967) has offered a resection of the changed head with acryl prosthesis, however at children and teenagers such operation is counter-indicative.
OSTEOHONDROPATY SEMILUNARIS BONES OF THE BRUSH
(Kinbek disease)
Disease is described Kinbek in 1925 and named by its name. At children and teenagers meets seldom, arises mainly at persons of a male in the age of 17-50 years, more often without any visible reasons. In its basis lays subchondral necrosis semilunaris bones. Clinically Kinbek disease is shown by local pains and a swelling in the field of semilunaris bones. At back bending the brush compressed in a fist, pains amplify. On the roentgenogram are defined all over again turbidity of osteal structure, sequestrum similary condensed shadows, decrease in height semilunaris bones. Treatment. Conservative: fixing plaster splint, physiotherapeutic procedures. The forecast favorable at duly diagnostics and long treatment.
TESTS
1. Principal cause of joint infections in all age groups is –
a) Pseudomonas
b) Staphylococcus aureus
c) Klebsiella
d) Streptococcus
e) E. coli
f) Proteus
g) Clostridia
2. E. coli and group B streptococci are involved more common in joint infections
a) in all age groups
b) in the elderly
c) in neonates
d) in the adult
3. Clinical features of joint infections are –
a) The affected joint is swollen
b) The affected joint is tender
c) There is an increasing pain and stiffness in an affected joint
d) The patient is febrile
e) Often the patient will lie motionless
f) All variants are true
4. Erythema may be present in patients with joint infections –
a) always
b) if there is an associated bursitis
c) if there is a spreading cellulitis
d) never
5. What of investigations is ideal for defining joint effusions?
a) Plain X-ray
b) Ultrasonography
c) Isotope scans
d) CT or MRI
6. Which of the following is correct regarding joint infections?
a) The affected joint is exquisitely painful to move
b) Ultrasound-guided puncture allows to aspirate fluid collections and to aid early diagnosis
c) Early aspiration of the affected joint provides temporary symptomatic relief
d) After aspiration, the affected joint should be splinted
e) Purulent inflammation requires operative method of treatment
f) All variants are true
7. Following is true about osteoarthritis –
a) This is most common form of arthritis
b) Three-quarters of the population will have some radiographic evidence of osteoarthritis by retirement age
c) The extent of disease is highly variable
d) Osteoarthritis is more common in women around the time of the menopause
e) All variants are true
8. Typical radiographic appearances of osteoarthritis are –
a) juxta-articular sclerosis
b) marginal osteophytes
c) joint space narrowing
d) All
9. Legg-Calve-Perthes disease is –
a) a benign condition of the navicular. Radiographs show a flattened and sclerotic navicular.
b) a benign condition of the lunate. The lunate flattens and fragments, disturbing the proximal row of the carpus.
c) a poorly understood condition of the hip in which the capital epiphysis undergoes a variable degree of infarction that leads to a cycle of collapse, fragmentation and deformity followed by healing
d) a benign condition. This can occur in athletic children, who may suffer acute or chronic avulsion injures, sometimes pulling off a piece of bone at the tendon insertion or origin. The tibial tubercle is prominent and tender.
10. Kohler’s disease is –
a) a benign condition of the navicular. Radiographs show a flattened and sclerotic navicular.
b) a benign condition of the lunate. The lunate flattens and fragments, disturbing the proximal row of the carpus.
c) a poorly understood condition of the hip in which the capital epiphysis undergoes a variable degree of infarction that leads to a cycle of collapse, fragmentation and deformity followed by healing
d) a benign condition. This can occur in athletic children, who may suffer acute or chronic avulsion injures, sometimes pulling off a piece of bone at the tendon insertion or origin. The tibial tubercle is prominent and tender.
11. Kienböck’s disease is –
a) a benign condition of the navicular. Radiographs show a flattened and sclerotic navicular.
b) a benign condition of the lunate. The lunate flattens and fragments, disturbing the proximal row of the carpus.
c) a poorly understood condition of the hip in which the capital epiphysis undergoes a variable degree of infarction that leads to a cycle of collapse, fragmentation and deformity followed by healing
d) a benign condition. This can occur in athletic children, who may suffer acute or chronic avulsion injures, sometimes pulling off a piece of bone at the tendon insertion or origin. The tibial tubercle is prominent and tender.
12. Osgood-Schlatter disease is –
a) a benign condition of the navicular. Radiographs show a flattened and sclerotic navicular.
b) a benign condition of the lunate. The lunate flattens and fragments, disturbing the proximal row of the carpus.
c) a poorly understood condition of the hip in which the capital epiphysis undergoes a variable degree of infarction that leads to a cycle of collapse, fragmentation and deformity followed by healing
d) a benign condition. This can occur in athletic children, who may suffer acute or chronic avulsion injures, sometimes pulling off a piece of bone at the tendon insertion or origin. The tibial tubercle is prominent and tender.
13. Following investigation must be performed to prove osteochondritis –
a) Radiographs
b) Ultrasound
c) Blood tests
d) History taking
c) All
Answers
B
C
F
B, C
B
F
E
D
C
A
B
D
A, D
МЕТОДИЧЕСКОЕ ОБЕСПЕЧЕНИЕ КОНТРОЛЯ ЗНАНИЙ СТУДЕНТОВ
(тестовые задания)
Тестовые задания для входного контроля
(лечебный факультет)
ВАРИАНТ 1.
1. В поджелудочной железе вырабатывается гормон:
1) адреналин
2) тироксин
3) инсулин
4) альдостерон
5) вазопрессин
2. Гипогликемическая кома - это:
1) состояние, возникающее после введения больших доз инсулина вследствие интенсивного перехода глюкозы внутрь нервных клеток, что приводит к нарушению деятельности ЦНС;
2) состояние, возникающее после введения больших доз инсулина вследствие угнетения механизмов переноса глюкозы через мембраны нервных клеток, что приводит к нарушению деятельности ЦНС;
3) состояние, возникающее после введения больших доз инсулина вследствие угнетения перехода глюкозы внутрь мышечных клеток, что в свою очередь вызывает недостаточное поступление глюкозы в клетки ЦНС и нарушение деятельности ЦНС;
4) состояние, возникающее после введения больших доз инсулина вследствие интенсивного перехода глюкозы внутрь мышечных клеток, что в свою очередь вызывает недостаточное поступление глюкозы в клетки ЦНС.
3. Противовоспалительным действием обладают гормоны:
1) адреналин
2) глюкагон
3) минералкортикоиды
4) глюкокортикоиды
4. Соматостатин - это:
1) соматотропный гормон
2) вещество, стимулирующее выделение гормона роста
3) вещество, тормозящее выделение гормона роста
4) гормон гипофиза
5. Форменные элементы, выступающие как звено иммунной системы организма:
эритроциты
нейтрофилы
эозинофилы
базофилы
лимфоциты
6. Световая микроскопия включает в себя следующие разновидности:
1) фазово-контрастную
2) электронную
3) темнопольную
4) в затемненном поле
5) иммерсионную
7. К грамотрицательным бактериям относятся:
1) сальмонеллы
2) клостридии
3) стафилококки
4) эшерихии
5) легионеллы
6) псевдомонады
8. Споры бацилл погибают при:
автоклавировании
пастеризации
тиндализации
длительном высушивании
действии дезинфектантов
9. Дезинфицирующие вещества:
уничтожают патогенные микробы
уничтожают споровые формы микробов
применяются для обеззараживания помещений, предметов обихода
токсичны для тканей организма
действуют в определенной концентрации
10. Паром под давлением в автоклаве стерилизуют:
сывороточные среды
перевязочный и шовный материал
медицинские инструменты
питательные среды с кровью
основные питательные среды
11. Текущим паром в автоклаве стерилизуют:
перевязочный материал
раствор глюкозы для парэнтерального введения
питательные среды с углеводами
шприцы
медицинские халаты, белье
12. Сухим жаром в печи Пастера стерилизуют:
перевязочный материал
лабораторную стеклянную посуду
шприцы
питательные среды
хирургический металлический инструментарий
13. Показателями фекального загрязнения объектов внешней среды являются:
кишечные палочки
энтерококки
гемолитические стрептококки
стафилококки
молочнокислые бактерии
14. К методам "холодной" стерилизации относятся: стерилизация
текучим паром
УФ-облучением
при помощи бактериальных фильтров
паром под давлением
15. Для проведения бактериологического метода диагностики используют:
лабораторных животных
питательные среды
куриные эмбрионы
культуры клеток
электронный микроскоп
16. Мишенями для антибиотиков в бактериальной клетке являются:
клеточная стенка
нуклеоид
цитоплазматическая мембрана
споры
рибосомы
17. Какие методы применяют для определения чувствительности микроорганизмов к антибиотикам?
метод диффузии в агар (метод дисков)
метод двойной диффузии в геле по Оухтерлони
метод серийных разведений
метод радиальной иммунодиффузии в геле по Манчини
метод иммунофлюоресценции
18. Источники получения антибиотиков:
вирусы
актиномицеты
плесневые грибы
растения
синтез
19. Положительная реакция Видаля может быть у:
больного брюшным тифом на первой неделе болезни
больного брюшным тифом на 2 неделе болезни
привитого брюшнотифозной вакциной
больного сыпным тифом
реконвалесцента
20. Какие анатомические структуры соответствуют глубокому паховому кольцу на задней поверхности передней брюшной стенки?
1) медиальная паховая связка
2) надпузырная ямка
3) латеральная паховая ямка
4) сосудистая лакуна
21. К каким костям прикрепляется мышца - поверхностный сгибатель пальцев?
1) проксимальная фаланга 2-5 пальцев
2) дистальная фаланга 2-5 пальцев
3) средняя фаланга 2-5 пальцев
4) 2-5 пястные кости
22. Какие мышцы лежат в третьем слое на передней поверхности предплечья?
1) глубокий сгибатель пальцев
2) локтевой сгибатель пальцев
3) длинный сгибатель большого пальца кисти
4) лучевой сгибатель запястья
23. Какие мышцы лежат во втором слое на предплечье?
1) локтевой сгибатель запястья
2) лучевой сгибатель запястья
3) поверхностный сгибатель пальцев
4) длинный сгибатель большого пальца кисти
24. К каким костям прикрепляется короткий разгибатель большого пальца кисти?
1) 1-я пястная кость
2) основание проксимальной фаланги большого пальца
3) дистальная фаланга большого пальца
4) головка проксимальной фаланги большого пальца
25. Укажите части желудка.
1) тело
2) кардиальная часть
3) дно
4) привратниковая часть
26. Укажите оболочки желудка.
1) подсерозная основа
2) мышечная оболочка
3) подслизистая основа
4) слизистая оболочка
27. Какие крупные складки находятся в области малой кривизны желудка?
1) косые складки
2) поперечные складки
3) продольные складки
4) кольцевидные складки
28. Какие складки находятся в области дна и тела желудка?
1) поперечные складки
2) кольцевидные складки
3) косые складки
4) продольные складки
29. Где располагается кольцевидная складка в желудке?
1) место перехода пищевода в желудок
2) дно желудка
3) тело желудка
4) место перехода желудка в двенадцатиперстную кишку
30. Укажите сосуд, от которого отходит желчнопузырная артерия.
1) желудочно-дуоденальная артерия
2) общая печеночная артерия
3) левая ветвь собственной печеночной артерии
4) правая ветвь собственной печеночной артерии
31. Укажите ветви нижней брыжеечной артерии.
1) средняя ободочная артерия
2) левая ободочная артерия
3) правая ободочная артерия
4) верхняя прямокишечная артерия
32. Укажите кровеносный сосуд, от которого отходят яичковые артерии.
1) внутренняя подвздошная артерия
2) внутренняя половая артерия
3) брюшная аорта
4) общая подвздошная артерия
33. Укажите источник происхождения прямокишечных артерий.
1) брюшная часть аорты
2) общая подвздошная артерия
3) внутренняя подвздошная артерия
4) нижняя брыжеечная артерия
34. Укажите сосуд, в который впадает латеральная подкожная вена руки.
1) подключичная вена
2) плечевая вена
3) подмышечная вена
4) плечеголовная вена
35. Укажите сосуд, в который впадает медиальная подкожная вена руки.
1) плечевая вена
2) подмышечная вена
3) подключичная вена
4) наружная яремная вена
36. Какое контрастное вещество используют для исследования органов желудочно-кишечного тракта:
Майодил
Сульфат бария
Билитраст
37. Какие контрастные вещества применяют для исследования желчного пузыря:
Майодил
Верографин
Эндоцистобил
38. При каких заболеваниях появляются чаши Клойбера:
при кишечной непроходимости
при дивертикулах полых органов
при перфорации стенки полого органа
39. При каких заболеваниях выявляется симптом «дефект наполнения»:
при объемных образованиях желудочно-кишечного тракта
при деструкциях в костной ткани
при эмболии сосудов
40. При каких заболеваниях выявляется симптом «ниши»:
при язве желудка
при дивертикулах желудка
при эрозиях пищевода
41. Чем отличается поздняя первичная хирургическая обработка от вторичной хирургической обработки?
техникой операции
сроками операции
наличием воспаления в ране
отсутствием первичной хирургической обработки
применением антибиотиков
42. Какой шов можно наложить на рану на восьмой день после первичной хирургической обработки?
1) первичный
2) провизорный
3) первично-отсроченный
4) ранний вторичный
5) поздний вторичный
43. Когда нельзя производить первичную хирургическую обработку раны?
1) при кровотечении
2) при шоке
3) в первые часы после ранения
4) при ее загрязнении
5) при СПИДе
44. Какие максимально допустимые сроки первичной хирургической обработки от момента ранения?
1) до 12 ч
2) до 24 ч
3) до 48 ч
4) до появления признаков развития инфекции
5) до 8 дней после ранения
45. Верно ли, что по характеру повреждения различают раны колотые, резаные, укушенные, рваные, ушибленные, отравленные, скальпированные, огнестрельные, размозженные?
1) да
2) нет
46. Мероприятия, провоцирующие развитие пневмоний в послеоперационном периоде:
1) ранняя активизация больного
2) массивная инфузионно-трансфузионная терапия
3) адекватное обезболивание
4) лечебная гимнастика
5) массаж грудной клетки
47. Что из перечисленного неэффективно в лечении и профилактике пролежней:
1) больных кладут на водяные и воздушные матрацы
2) адекватная иммобилизация
3) рано активизируют больных
4) протирают спиртом заднюю поверхность туловища
5) подкладывают круги и кольца
48. Плановые операции проводятся при:
1) распадающейся злокачественной опухоли
2) абсцедирующем фурункуле
3) варикозное расширение вен
4) циркулярном ожоге предплечья III б степени
5) открытом переломе голени
49. Риск оперативных вмешательств резко возрастает при:
1) глубоком кариесе зубов
2) мерцательной аритмии
3) варикозной болезни вен нижних конечностей I-II ст
4) хроническом тонзиллите
5) перенесенной ранее ортопедической операции на нижней конечности
50. В раннем послеоперационном назначают:
1) строгий постельный режим
2) горизонтальное положение в кровати
3) положение по Фовлеру
4) ходьбу по палате
51. Какая из операций всегда считается экстренной?
1) резекция желудка
2) вскрытие абсцесса
3) пневмонэктомия
4) наложение вторичных швов
5) аппендэктомия
52. Жировая эмболия может быть осложнением:
1) перелома костей
2) ранения вен
3) переливания крови
4) внутривенных вливаний
5) полостных операций
53. Какие повреждения следует считать прямыми:
1) перелом позвоночника при падении на седалищные бугры
2) разрыв Аххилова сухожилия при резком сгибании стопы
3) перелом лучевой кости при падении на кисть
4) перелом шейки бедра при ротации бедра
5) перелом бедра при падении тяжести на бедро
54. Какую шину надо применить при переломе бедра для транспортной иммобилизации:
1) шину Дитерихса
2) шину Кузьминского
4) шину Крамера
5) шину Белера
6) шину Цито
55. К тромбофлебиту вен предрасполагают
1) варикозная болезнь вен
2) прием контрацептивов
3) наличие гнойных процессов в области вены
4) продолжительные и частые венепункции
5) все вышеперечисленное
56. Для утверждения диагноза рак достаточным будет
1) визуализация опухоли при эндоскопии
2) гистологическое исследование
3) пальпация опухоли
4) рентгенологическое исследование
57. Накостный остеосинтез подразумевает
1) открытую репозицию перелома и фиксацию спицами
2) открытую репозицию перелома и фиксацию болтом-стяжкой
3) открытую репозицию перелома и фиксацию пластиной
4) фиксацию отломков пластиной
5) ПХО раны, удаление отломков, проведение спиц и фиксация перелома пластиной
58. Больной был сбит легковым автомобилем на скорости 60 км/ч. Доставлен в стационар бригадой скорой медицинской помощи в бессознательном состоянии, при осмотре отмечаются: ликворея из левого уха, симптом «галифе», укорочение правого бедра, гематома, деформация, патологическая подвижность в верхней трети правого бедра, также имеются доскообразный живот, крепитация в проекции 7,8,9,10 ребер слева. Проанализируйте ситуацию и ответьте, какая патология имеется у больного:
1) перелом основания черепа
2) перелом правого бедра
3) тяжелая сочетанная травма
4) перелом ребер слева
59. Больной 20 дней назад получил открытый перелом бедра. Произведено ПХО раны, наложен аппарат Илизарова. Получал антибиотики, местно - перевязки. Рана зажила. Последние 2 дня появились боли в бедре, краснота, отек, лихорадка. С чем связано изменения в клинике
1. с тромбофлебитом
2. оставлением в ране инородного тела
3. рассасыванием параоссальной гематомы
4. с посттравматическим остеомиелитом
60. Для диагностики рака прямой кишки в первую очередь необходимо произвести
1) пальцевое исследование прямой кишки и ректороманоскопию
2) анализ кала на скрытую кровь
3) лапароскопию
4) ультразвуковое исследование органов малого таза
61. После инфузионной терапии у больной возникли лихорадка, отек правой верхней, конечности, гиперемия по внутренней поверхности плеча, лимфангит в аксиллярной ямке справа. Что это:
1) острый миозит
2) рожистое воспаление
3) флегмона
4) острый тромбофлебит
5) вывих в локтевом суставе
62. Длительно существующий параректальный свищ приводит к
1) стулобоязни
2) кровотечению при дефекации
3) малигнизации
4) выделением слизи при дефекации
63. Острый тромбофлебит после инфузионной терапии может явиться следствием:
1) введения большого количества физиологического раствора
2) введения антибиотиков внутривенно
3) использования иглы вместо внутривенного катетера
4) длительного стояния внутривенного катетера
64. Радикальным методом лечения острого гнойного подкожного парапроктита является:
1) систематические пункции абсцесса с промыванием антибиотиками
2) вскрытие и дренирование полости абсцесса
3) вскрытие гнойной полости с иссечением крипты в зоне воспаления анальной железы и гнойного хода
4) общая антибиотикотерапия
65. Для диагностики источника внутрибрюшного кровотечения наиболее информативным методом исследования является:
1) фиброгастроскопия
2) термография
3) пневмоперитонеография
4) лапароскопия
5) ультразвуковое исследование органов брюшной полости
66. В лечении гнойного плеврита главное значение имеет:
1) антибиотикотерапия
2) межреберный блокады, антибиотикотерапия
3) адекватное дренирование плевральной полости
4) постуральный дренаж
5) дренирование плевральной полости, антибиотикотерапия
67. Костный панариций – это:
1) изолированное воспаление фаланги пальца
2) остеомиелит фаланги пальца
3) воспаление всех тканей пальца
4) киста в диафизе фаланги
68. Переливание первых 200 мл крови оказывает:
1) выраженный дезинтоксикационный эффект
2) гемостатическое действие
3) восполняет ОЦК
4) питательное действие
5) устраняет анемию
69. Острая анемия является показанием к:
1) наложению жгута
2) переливанию эритромассы
3) ультразвуковому исследованию
4) терапии антикоагулянтами
5) назначению витамина К
70. Наиболее частым осложнением рака левой половины ободочной кишки является:
1) воспаление толстой кишки
2) выпадение прямой кишки
3) кишечная непроходимость
4) перфорация опухоли
5) профузное кишечное кровотечение
71. У больного на фоне длительно существующей язвы желудка появились симптомы интоксикации, анемия, снизилась масса тела. Что можно заподозрить?
1) выраженный гастрит
2) стеноз выходного отдела желудка
3) малигнизацию язвы
4) кровотечение из язвы
72. Операцией восстановления проходимости ЖКТ при запущенном стенозе выходного отдела желудка за счет роста опухоли является
1) резекция желудка с анастозом
2) резекция желудка с анастозом и наложением гастростомы
3) гастростомия
4) наложение обходного анастомоза между тонкой кишкой и желудком
73. Какой метод контроля за стерилизацией белья в автоклаве (из приведенных) является наиболее надежным?
1) плавление серы
2) плавление антипирина
3) плавление пирамидона
4) плавление резорцина
5) метод Микулича
74. Резиновые перчатки нельзя стерилизовать в:
1) сулеме
2) хлорамине
3) автоклаве
4) сухожаровом шкафу
75. Что ошибочно отнесено к средствам химической антисептики?
1) перекись водорода
2) марганцовокислый калий
3) этиловый спирт
4) диоксидин
5) нашатырный спирт
76. Какие из перечисленных веществ не применяются для обработки рук хирурга?
1) первомур
2) новосепт
3) церигель
4) этиловый спирт
5) хлорамин
77. Основной симптом столбняка это:
1) затруднение при открывании рта
2) тяжесть в мышцах затылка
3) эйфория
4) плохой сон
5) судороги
78. Выберете неправильный ответ. Для рака лёгкого не является характерным:
1) надсадный кашель
2) повышение температуры тела
3) затемнение в лёгком при рентгеноскопии
4) изменение эпителия бронха, обнаруженное бронхоскопически
5) отсутствие опухолевых клеток в изменённой ткани
79. Гидраденит? Это воспаление:
1) сальных желёз
2) потовых желёз
3) волосяного мешочка
4) лимфатического сосуда
5) лимфоузла
80. Назовите место обычной локализации гидраденита?
1) подмышечная впадина
2) подчелюстная область
3) шея
4) спина
5) лицо
81. Какую пробу не проводят с кровью донора пред каждым переливанием крови?
1) групповая совместимость
2) индивидуальная совместимость
3) биологическая проба
4) определение резус-совместимости
5) определение резус-фактора
82. Свободная кожная пластика при глубоких ожогах возможна:
1) уже в период ожогового шока
2) после выполнения ожогового дефекта грануляциями
3) сразу после химического некроза струпа
4) как правило, через 1-2 недели после травмы
5) не ранее 4-5 недель с момента ожога
83. Кровопотеря лёгкой степени - это потеря:
1) до 50 мл крови
2) до 100мл крови
3) до 500 мл крови
4) до 750 мл крови
5) до 1000 мл крови
84. Кровопотеря тяжелой степени - это потеря:
1) до 500 мл крови
2) до 750 мл крови
3) до 1000 мл крови
4) свыше 1500 мл крови
85. При каком виде кровотечения существует реальная опасность воздушной эмболии:
1) повреждении артерии бедра
2) повреждении лучевой артерии
3) капиллярное кровотечение
4) повреждение вен голени
5) повреждение вен шеи
86. При каком кровотечении наблюдается пенистая кровь?
1) носовое
2) пищеводное
3) лёгочное
4) кишечное
87. В какие сроки производят плановые вмешательства:
1) первые сутки после госпитализации
2) сразу же после установления диагноза
3) первые часы после госпитализации
4) после тщательного обследования пациента и тщательной предоперационной подготовки
5) сроки определяются самим пациентом
88. Чем срочные вмешательства отличаются от экстренных:
1) есть возможность выполнить клиническое обследование, минимальную подготовку и ряд клинических тестов
2) при срочном вмешательстве диагноз заболевания четко установлен
3) экстренные вмешательства преследуют только цель спасти жизнь пациента
4) при срочных вмешательствах никогда не проводят гемотрансфузии
5) срочные вмешательства позволяют выполнить радикальные операции
89. Выберете путь, который никогда не используется для гемотрансфузии:
1) подкожный
2) внутривенный,
3) внутрикостный
4) внутриартериальный
90. Проникающей резаной раной живота называется рана с повреждением:
1) кожи
2) мышц
3) париетальной брюшины
4) висцеральной брюшины
5) внутренних органов
91. Решающим в дифференциальной диагностике острого аппендицита с нарушенной внематочной беременностью является:
1) симптом Кохера - Волковича
2) симптом Промптова
3) головокружение и обмороки
4) симптом Бартомье - Михельсона
5) пункция заднего свода влагалища
92. Наиболее опасным осложнением тромбоза глубоких вен является:
1) трофическая язва голени
2) эмболия легочной артерии
3) тромбофлебит поверхностных вен
4) облитерация глубоких вен
5) слоновость
93. К интраоперационным методам исследования внепеченочных желчных путей относятся все, кроме:
1) пальпации холедоха
2) холедохоскопии
3) интраоперационной холангиографии
4) зондирования холедоха
5) внутривенной холангиографии
94. При подозрении на перфоративную язву желудка первым исследованием должна быть:
1) рентгеноскопия желудка с бариевой взвесью
2) обзорная рентгенография брюшной полости
3) экстренная эзофагогастродуоденоскопия
4) ангиография (селективная чревной артерии)
5) лапароскопия
95. Наиболее информативным методом исследования при остром панкреатите является:
1) диагностический пневмоперитонеум
2) обзорная рентгеноскопия брюшной полости
3) лапароскопия
4) гастродуоденоскопия
5) определение амилазы крови и мочи, УЗИ
96. Наиболее частым осложнением струмэктомии является:
1) повреждение возвратного нерва
2) рецидив тиреотоксикоза
3) тетания
4) гипотиреоз
5) прогрессирующий экзофтальм
97. Метастаз Крукенберга локализуется:
1) в прямокишечно-пузырной складке
2) в пупке
3) в яичниках
4) между ножками кивательной мышцы
5) в печени
98. Невозможность определения пульсации брюшного отдела аорты в эпигастральной области при остром панкреатите носит название симптома:
1) Мейо - Робсона
2) Мондора
3) Кера
4) Кулена
5) Воскресенского
99. При оценке проходимости глубоких вен используется функциональная проба:
1) Тальмана
2) Шейниса
3) Гаккенбруха
4) Дельбе - Пертеса
5) Броди - Троянова - Тренделенбурга
100. Характерным рентгенологическим признаком центрального рака легкого, отличающего его от периферического рака, является:
1) наличие округлой тени в легком
2) наличие "дорожки" к корню легкого
3) ателектаз
4) высокое стояние диафрагмы
5) смещение средостения
Вариант 2.
Функция лимфоцитов заключается в:
фагоцитозе и обеспечении репаративной стадии воспалительного процесса
бактерицидном действии
участии в поддержании рН крови
распознавании антигенов и выработке иммуноглобулинов (антител)
Где синтезируется протромбин:
в селезенке
в почках
в красном костном мозге
в печени
в гипоталамусе
Вторая группа крови характеризуется наличием:
1) агглютиногенов АВ
2) агглютининов альфа и бета
3) агглютиногена А, агглютинина бета
4) агглютиногена В и агглютинина альфа
5) агглютинина А, агглютиногена альфа
Третья группа крови характеризуется наличием:
агглютиногенов АВ
агглютининов альфа и бета
агглютиногена А, агглютинина бета
агглютиногена В и агглютинина альфа
агглютинина А, агглютиногена альфа
Отметьте основное положение современных правил переливания крови:
человек, имеющий 1 группу крови - это универсальный донор
человек, имеющий 4 группу крови - это универсальный реципиент
3) при переливании крови донор и реципиент должны иметь одинаковую группу крови
4) 2 группу крови можно переливать реципиентам с 1, 2, 4 группами крови
5) 3 группу крови можно переливать реципиентам с 1, 3, 4 группами крови
Назовите возбудителей пищевых токсикоинфекций
1) Escherichia coli
2) Staphylococcus epidermidis
3) Salmonella enterica (S.enteritidis)
4) Clostridium botulinum
5) Neisseria meningitidis
6) Proteus vulgaris
7. Лабораторная диагностика пищевых интоксикаций включает:
1) микроскопию пищевых продуктов
2) микроскопию фекалий больного
3) заражение экстрактом из пищевых продуктов лабораторного животного
4) заражение материалом от больного лабораторного животного
5) исследование сыворотки больного на выявление токсина
6) аллергическую пробу
Значение кишечной палочки для макроорганизма?
1) принимает участие в синтезе витаминов группы B
2) является антагонистом патогенной и гнилостной микрофлоры
3) участвует в обмене жиров
4) участвует в минеральном обмене
5) вызывает колиэнтериты
6) вызывает брюшной тиф
7) вызывает дизентериеподобные заболевания
Назовите возбудителей холеры у человека:
1) Cholerae classica (asiaticae)
2) V.cholerae eltor
3) V.parahaemolyticus.
4) V.cholerae o139 (Bengal)
5) V.Metschnikovi
Эндотоксин играет основную роль в патогенезе инфекции, вызываемой:
1) Vibrio cholerae
2) Staphylococcus aureus
3) Salmonella typhi
4) Corynebacterium diphtheriae
5) Clostridium perfringens
В состав биотерапевтических препаратов, применяемых для коррекции микрофлоры кишечника, входят:
1) лактобактерии
2) бифидобактерии
3) стафилококки
4) сальмонеллы
5) эшерихии
Назовите факторы передачи возбудителей газовой гангрены.
1) молочные продукты
2) насекомые
3) почва
4) мясные продукты
5) пыль
6) грызуны
Назовите возбудителей газовой гангрены.
1) Clostridium tetani
2) Clostridium botulinum
3) Bacteroides sp.
4 Clostridium perfringens
5) Clostridium novyi
6) Clostridium septicum
7) Clostridium sordelli
8) Clostridium histolyticum
Чем проводить специфическое лечение газовой гангрены?
1) антибиотики
2) сульфаниламиды
3) физиологический раствор
4) глюкоза
5) антитоксическая поливалентная противогангренозная 6.сыворотка
7) антитоксическая моновалентная противогангренозная сыворотка
8) кровозаменители
Какие токсины играют роль в патогенезе столбняка?
1) эритрогенный токсин
2) тетанолизин
3) энтеротоксин
4) тетаноспазмин
5) летальный токсин
6) эндотоксин
7) экзотоксин
Какие препараты применяют для специфического лечения столбняка?
1) антибиотики
2) столбнячный анатоксин
3) противостолбнячная антитоксическая сыворотка
4) антимикробная сыворотка
5) столбнячный иммуноглобулин
6) АКДС
7) сульфаниламиды
Профилактика газовой гангрены включает:
1) первичную хирургическую обработку раны
2) введение столбнячного анатоксина
3) оксигенацию раны
4) введение поливалентной антитоксической противогангренозной сыворотки
5) введение анатоксинов возбудителей газовой гангрены
6) антибиотикотерапию
7) введение моновалентной антитоксической противогангренозной сыворотки
Какие части имеются у диафрагмы.
1) поясничная
2) грудинная
3) позвоночная
4) реберная
Укажите структуры, участвующие в образовании паховой связки?
1) апоневроз внутренней косой мышцы живота
2) фасция поперечной мышцы живота
3) апоневроз поперечной мышцы живота
4) апоневроз наружной косой мышцы живота
20. Где берет начало внутренняя косая мышца живота?
1) подвздошный гребень
2) лобковая кость
3) паховая связка
4) пояснично-грудная фасция
Укажите верхнюю границу живота.
1) мечевидный отросток
2) Х грудной позвонок
3) реберная дуга
4) XII грудной позвонок
22. Какие функции выполняет диафрагма?
1) дыхательная мышца
2) мышца брюшного пресса
3) сгибание позвоночника
4) разгибание позвоночника
Какие мышцы покрывает внутрибрюшная фасция?
1) диафрагма
2) поясничная мышца
3) подвздошная мышца
4) прямая мышца живота
Укажите анатомические структуры, участвующие в образовании задней стенки влагалища прямой мышцы живота?
1) паховая связка
2) апоневроз внутренней косой и поперечной мышц живота
3) апоневроз наружной косой мышцы живота
4) поперечная фасция
25. Какие анатомические образования участвуют в формировании передней стенки влагалища прямой мышцы живота ниже пупка?
1) поперечная фасция
2) апоневроз поперечной мышцы живота
3) апоневроз наружной косой мышцы живота
4) апоневроз внутренней косой мышцы живота
26. Укажите структуры, участвующие в образовании стенок пахового канала.
1) внутренняя косая мышца живота
2) прямая мышца живота
3) поперечная фасция
4) паховая связка
27. Укажите мышцы возвышения большого пальца кисти.
1) мышца, противопоставляющая большой палец кисти
2) короткий сгибатель большого пальца кисти
3) первая тыльная межкостная мышца
4) мышца, приводящая большой палец кисти
28. Укажите мышцы возвышения мизинца.
1) длинная ладонная мышца
2) короткая ладонная мышца
3) мышца, отводящая мизинец
4) мышца, противопоставляющая мизинец
29. Какие функции выполняют червеообразные мышцы?
1) разгибают проксимальные фаланги
2) сгибают проксимальные фаланги
3) разгибают средние фаланги
4) сгибают средние фаланги
30. Какие мышцы относятся к внутренней группе мышц таза?
1) внутренняя запирательная мышца
2) грушевидная мышца
3) малая поясничная мышца
4) подвздошно-поясничная мышца
31. Укажите мышцы передней группы бедра:
1) четырехглавая мышца
2) гребенчатая мышца
3) портняжная мышца
4) напрягатель широкой фасции
32. Укажите мышцы задней группы бедра:
1) большая ягодичная мышца
2) двуглавая мышца бедра
3) полусухожильная мышца
4) тонкая мышца
33. Укажите мышцы, образующие глубокий слой задней группы мышц голени.
1) подколенная мышца
2) длинный сгибатель пальцев
3) подошвенная мышца
4) задняя большеберцовая мышца
34. Назовите мышцы медиальной группы на подошве.
1) короткий сгибатель большого пальца
2) мышца, приводящая большой палец стопы
3) подошвенная мышца
4) задняя большеберцовая мышца
35. Укажите мышцы, относящиеся к средней группе мышц подошвы стопы.
1) червеобразные мышцы
2) подошвенные межкостные мышцы
3) короткий сгибатель пальцев
4) тыльные межкостные мышцы
36. Укажите мышцы тыла стопы.
1) короткий разгибатель пальцев
2) тыльные межкостные мышцы
3) мышца, отводящая большой палец
4) короткий разгибатель большого пальца
37. Симптом «дефекта наполнения» в желудке характерен для:
язвы желудка
дивертикула
опухоли желудка
Для острой кишечной непроходимости характерно:
1) нарушение смещаемости кишечника
чаши Клойбера
наличие свободного газа в брюшной полости
Для перфорации стенки полого органа брюшной полости характерно:
нарушение смещаемости органа
чаши Клойбера
наличие свободного газа в брюшной полости
Какие контрастные вещества используют для фистулографии:
иодалид
иодолипол
урографин
Какие контрастные вещества применяют для исследования сосудов:
иодолипол
сернокислый барий
омнипак
Механизмом действия протеолитических ферментов при гнойных процессах является все, кроме:
1) лизис некротизированных тканей
2) повышение свертываемости крови
3) фибринолиз
4) потенцирование действия антибиотиков
5) противоотечное действие
43. Дайте наиболее полный правильный ответ кровотечение - это излияние крови:
1) во внешнюю среду;
2) в полости организма;
3) в ткани организма;
4) в ткани, полости организма или во внешнюю среду;
5) во внешнюю среду и полости организма
44. Истинная аневризма - это:
1) патологическое выпячивание стенки сердца или сосуда
2) разрыв сосудистой стенки с образованием гематомы
3) расслоение стенки артерии
4) расположение артерии внутри гематомы
5) расширение вены
Временный гемостаз осуществляется:
1) лигированием сосуда в ране
2) наложением сосудистого шва
3) протезированием сосуда
4) давящей повязкой, жгутом, пальцевым прижатием
5) диатермокоагуляцией
46. Какие кровотечения различают по анатомической классификации?
1) первичные, вторичные
2) скрытые внутренние, скрытые наружные
3) артериальные, венозные, капиллярные, паренхиматозные
4) ранние, поздние
5) наружные, внутренние
47. Что такое гематома?
1) скопление крови, ограниченное тканями
2) кровоизлияние в паренхиматозные органы
3) скопление крови в полости сустава
4) пропитывание кровью мягких тканей
5) скопление крови в плевральной или брюшной полости
Сосудистый шов в целях гемостаза накладывается при повреждении:
1) капилляров
2) артериол
3) венул
4) любых сосудов
5) магистральных сосудов
Укажите метод окончательного гемостаза при ранении аорты:
1) перевязка сосуда в ране
2) сосудистый шов
3) наложение кровоостанавливающего зажима
4) тампонада раны
5) перевязка на протяжении
Укажите метод окончательного гемостаза при ранении нижней полой вены:
1) перевязка сосуда в ране
2) сосудистый шов
3) наложение кровоостанавливающего зажима
4) тампонада раны
5) перевязка сосуда на протяжении
Укажите метод окончательного гемостаза при ранении тыльной артерии стопы:
1) перевязка сосуда в ране
2) сосудистый шов
3) наложение кровоостанавливающего зажима
4) тампонада раны
5) шунтирование сосуда
Укажите метод окончательного гемостаза при глубоком разрыве селезенки, гемоперитонеуме:
1) ушивание разрыва
2) перевязка селезеночной артерии
3) спленэктомия
4) обшивание кровоточащих сосудов
5) пломбирование дефекта селезенки
Укажите метод окончательного гемостаза при ранении общей сонной артерии:
1) наложение кровоостанавливающего зажима
2) сосудистый шов
3) перевязка на протяжении
4) тампонада раны
5) закручивание сосуда
Укажите правило, которое должен соблюдать бинтующий:
1) находиться позади больного, чтобы не дышать ему в лицо
2) смотреть на лицо больного и бинтовать
3) смотреть только на бинтуемую часть тела
4) следить за действиями помощника и бинтовать
5) смотреть на лицо больного и бинтуемую часть тела
Перевязочный материал должен удовлетворять всем требованиям, кроме:
1) гигроскопичности
2) эластичности
3) возможности стерилизации без потери качества герметичности
4) раздражающего действия на ткани
5) капиллярности
Следует ли сбривать волосы с волосистых участков тела перед наложением липкопластырной повязки?
1) да
2) нет
Пращевидная повязка не применяется для удержания перевязочного материала в области:
1) носа
2) затылка
3) подбородка
4) ушной раковины
С помощью какой повязки можно удержать перевязочный материал в области промежности?
1) пращевидной
2) сходящейся черепашьей
3) расходящейся черепашьей
4) Т-образной
5) колосовидной
Для поддержания мошонки после операции на ней применяется повязка:
1) пращевидная
2) сходящаяся черепашья
3) расходящаяся черепашья
4) колосовидная
5) суспензорий
На конусообразные участки тела(предплечье, голень) накладывается повязка:
1) черепашья сходящаяся
2) черепашья расходящаяся
3) крестообразная
4) спиральная с перегибом бинта
5) возвращающаяся
Какие виды анестезии относятся к проводниковым?
1) по Лукашевичу-Оберсту
2) паравертебральная
3) перидуральная
4) спинномозговая
5) межреберная
Выберите правильную комбинацию ответов
1. 1,2,3,4,5 2. 2,3,5 3. 1,2,4 4. 1,2,5 5. 1,2,3,5
При проведении паравертебральной блокады происходит блокада
1) передних корешков
2) задних корешков
3) спинномозгового нерва
Местная анестезия является методом выбора при:
1) полостных операциях
2) вскрытиях гнойников различных локализаций
3) операциях на щитовидной железе
4) пункциях плевральной полости
Какая среда является лучшей для переливания больному с острой кровопотерей:
1) эритроцитарная масса
2) цельная кровь
3) плазма
4) сыворотка крови
5) полиглюкин
В каких элементах крови содержится резус-фактор:
1) плазма
2) сыворотка
3) лейкоциты
4) тромбоциты
5) эритроциты
Для снятия присохшей к ране повязки применяют:
1) эфир
2) водорода пероксид
3) спирт
4) скипидар
5) клеол
В какой концентрации используют поваренную соль в качестве гипертонического раствора при лечении гнойных ран?
1) 0,1%
2) 1%
3) 2%
4) 10%
5) 20%
Паллиативные операции служат для:
1) излечения больного с помощью хирургического вмешательства
2) облегчить страдания больного
3) избежать многомоментных операций
4) выявить основную патологию оперативным путем
5) предупредить повреждение магистральных сосудов
По срочности различают операции:
1) экстренные, срочные, радикальные, плановые
2) экстренные, срочные, симультанные, учебные
3) экстренные, срочные, плановые
4) экстренные, срочные, несрочные, плановые
5) экстренные, срочные, учебные, плановые
Какая рана заживает быстрее других?
1) с грануляциями красными крупнозернистыми
2) с грануляциями мелкозернистыми малиновыми
3) с грануляциями бледно-розовыми
4) с избыточными грануляциями
5) с грануляциями серого цвета
Какой из перечисленных симптомов не является обязательным для раны?
1) боль
2) нарушение чувствительности тканей
3) кровотечение
4) зияние
5) нарушение целостности покрова тела
Грязные операции - это:
позиция костных отломков
2) остеосинтез при переломах бедра
3) наложение аппарата Иллизарова
4) вскрытие абсцесса
5) кожная пластика
Жизненные показания к операции:
1) язвенная болезнь желудка
2) ущемленная грыжа
3) трофические язвы голени
4) аутодермопластика
5) хронический остеомиелит
Радикальные операции - это:
1) гастростомия
2) аппендэктомия
3) репозиция перелома
4) лапароскопия
5) холецистостомия
К клиническим методам исследования не относят:
1) осмотр
2) пальпация
3) ангиография
4) перкуссия
5) аускультация
К диагностическим операциям относят:
1) холецистэктомию
2) резекцию желудка
3) биопсию печени
4) пиелостомию
К специальным методам обследования не относят:
1) функциональные
2) иммунологические
3) определение объема движений в суставах
4) гистологические
5) цитологические
Закрытым методом не проводятся следующие операции:
1) эндоваскулярное расширение сосудов
2) дилатация кардии
3) металлоостеосинтез
4) вправление костных отломков
5) эндоскопическое удаление полипа желудка
Предоперационный эпикриз служит для:
1) обоснования показаний и составления плана операции
2) выбора инструментов для вмешательства
3) обоснования диагноза
4) выбора объема и метода операции
5) выбора метода обезболивания
Для борьбы с болью после операции в первые сутки применяют:
1) эпидуральную анестезию
2) наркотические анальгетики
3) среднефизиологическое положение кровати
4) активное ведение послеоперационного периода
5) лечебный наркоз
Оперативный доступ должен отвечать одному главному условию:
1) быть наименее травматичен
2) учитывать косметические последствия операции
3) обеспечивать широкое обнажение патологического очага
4) производиться в проекции болевых точек
5) выбираться с учетом желания больного
Больному показано срочное оперативное вмешательство. Какие мероприятия в предоперационном периоде являются излишними:
1) общеклиническое обследование
2) коррекция водно-солевого обмена
3) нормализация уровня глюкозы крови
4) ЭКГ
5) коррекция уровня холестерина крови
В свежей ране имеется отграниченный участок некроза края кожи. Что необходимо сделать?
1) иссечь омертвевший участок кожи
2) наложить повязку с протеолитическими ферментами
3) наложить повязку с мазью Вишневского
4) наложить повязку с гипертоническим раствором
5) наложить повязку с метилурацилом
При раке тела желудка радикальной операцией считается:
1) дистальная субтотальная резекция
2) проксимальная субтотальная резекция
3) гастрэктомия
4) резекция 2/3 желудка
5) гастроэнтеростомия
85. Оставление тампонов в брюшной полости после аппендэктомии показано при:
1) неостановленном капиллярном кровотечении
2) гангренозно-перфоративном аппендиците
3) местном перитоните
4) разлитом перитоните
5) всех этих состояниях
86. Радикальным при варикозной болезни будет вмешательство:
1) устраняющее сброс из глубоких вен в поверхностные
2) обеспечивающее удаление несостоятельных поверхностных вен
3) корригирующее несостоятельные клапаны глубоких вен
4) решающее все эти задачи
5) позволяющее решить задачи 1 и 2
87. При раке главного бронха показана:
1) пульмонэктомия
2) лобэктомия
3) сегментэктомия
4) лучевая терапия без операции
5) все неверно
88. При лечении аппендикулярного инфильтрата не применяют:
1) физиотерапевтического лечения
2) антибиотиков
3) стационарного лечения
4) наркотических средств
5) диеты
89. При нежизнеспособной петле тонкой кишки производится:
1) резекция приводящей петли, отступя 20 см от некроза
2) резекция кишки в пределах видимой границы некроза
3) наложение обходного анастомоза
4) выведение кишки
5) резекция отводящей петли, отступя 15-20 см от некроза
90. Прямую паховую грыжу характеризует слабость стенки:
1) задней
2) верхней
3) передней
4) нижней
5) всех стенок
91. При гангрене, поражающей одну из долей легкого, рекомендуется:
1) ежедневная санация бронхиального дерева через бронхоскоп
2) введение антибиотиков в легочную артерию
3) лобэктомия
4) интенсивная терапия с эндобронхиальным введением антибиотиков
5) комплексная терапия, включающая все названные выше консервативные методы лечения
92. Толстокишечная обтурационная непроходимость чаще всего вызывается:
1) инородными телами
2) желчными камнями
3) злокачественными опухолями
4) спайками брюшной полости
5) гельминтами
93. Нерадикальной операцией, выполняемой при раке кардиального отдела желудка, с целью обеспечения питания больного является:
1) гастростомия
2) пилоропластика
3) гастроэнтероанастомоз
4) дистальная резекция желудка
5) гастродуоденоанастомоз
94. Артерио-венозный свищ образуется чаще всего в результате:
1) ранения
2) инфекции
3) новообразования
4) все верно
5) все неверно
95. Основным методом лечения кардиоспазма является:
1) кардиопластика по Геллеру
2) фундопликация по Ниссену
3) кардиодилатация
4) различные способы экстрамукозной пластики
5) бужирование
96. Характер оперативного вмешательства при прободной язве желудка определяет:
1) возраст больного
2) локализация перфоративного отверстия
3) степень выраженности перитонита
4) срок с момента перфорации
5) все перечисленное
97. Для острой высокой кишечной непроходимости не характерно:
1) быстрое снижение ОЦК
2) неукротимая рвота
3) вздутие живота в первые часы заболевания
4) быстрое обезвоживание
5) схваткообразные боли
98. Невправляемость грыжи является следствием:
1) спаек между вышедшими в грыжевой мешок органами и стенкой мешка
2) спаек между вышедшими в грыжевой мешок петлями кишечника
3) рубцового процесса между грыжевым мешком и окружающими его тканями
4) несоответствия вышедших в грыжевой мешок органов размеру грыжевых ворот
5) всего перечисленного
99. Для полной эмболии бедренной артерии не характерно:
1) пульсации под пупартовой связкой
2) отсутствие пульсации бедренной артерии в гунтеровом канале
3) отсутствие пульсации подколенной артерии
4) усиление пульсации (по сравнению с другой конечностью) бедренной
артерии тотчас под пупартовой связкой
5) бледность конечности
100. Укажите оптимальный объем операции при кровотечении из вен пищевода на фоне внутрипеченочной формы портальной гипертензии:
1) прошивание вен пищевода.
2) портокавальный анастомоз.
3) спленэктомия.
4) склерозирование вен пищевода.
Вариант 3.
1. Брадикардия - это:
1) увеличение частоты сердечных сокращений свыше 60 в мин.
2) изменение ритма сердечных сокращений
3) аритмия, вызванная возникновением экстрасистол
4) уменьшение частоты сердечных сокращений меньше 60 в мин
5) остановка сердца
Пневмоторакс - это:
1) остановка дыхания
2) одышка
3) попадание воздуха в легкие
4) попадание воздуха в плевральную полость
5) попадание воздуха в альвеолы
Концентрация HCl и рH желудочного сока в норме равны:
1) 0,1%, 0,1 - 0,5
2) 0,5%, 1,5 - 1,8
3) 1,5%, 2,5 - 3,0
4) 0,2%, 0,2 - 0,6
5) 3%, 1,1 - 3,4
В состав желудочного сока входит фермент:
1) тироксин
2) хемотрипсин
3) пепсин
4) энтераза
5) инсулин
Во вторую фазу желудочной секреции отделение желудочного сока стимулирует гормон:
1) пепсин
2) трипсин
3) тиротропин
4) гастрин
5) панкреозимин
Ботулизмом можно заразиться, употребляя пищевые продукты:
1) молочные
2) мясные консервы
3) консервированные грибы
4) свежие, но не мытые овощи и фрукты
5) колбаса
6) хлебные изделия
7) рыбные консервы
Микробиологическая диагностика ботулизма это:
1) бактериоскопическое исследование пищевых продуктов
2) посев продуктов с целью выделения клостридий
3) определение в крови больного токсина биологическим методом
4) постановка аллергической пробы
5) определение в сыворотке больного токсина в РНГА
6) иммунофлюоресцентное исследование
Возбудителем сибирской язвы является:
1) Bacillus anthracis
2) Brusella abortus
3) Brucella suis
4) Francisella tularensis
5) Brucella melitensis
6) Bacillus cereus
7) Yersinia pestis
Какие лица могут быть отнесены к группе риска по инфекции ВИЧ?
1) больные гeмофилией
2) гомосексуалисты
3) гетеросексуалы
4) бисексуалы
5) работники пищевых предприятий, обслуживающие больных СПИДом
6) врачи (хирурги, акушер-гинекологи), осуществляющие лечение больных СПИДом
7) больные венерическими заболеваниями
Какие серологические реакции применяются для диагностики СПИДа?
1) РСК
2) иммуноферментный анализ (ИФА)
3) реакция преципитации
4) реакция торможения гемагглютинации
5) иммуноблотинг (western blott)
6) реакция нейтрализации
7) реакция непрямой гемагглютинации
Каковы пути передачи вируса бешенства?
1) воздушно-капельный
2) водный
3) трансмиссивный
4) алиментарный
5) контактный (ослюнение)
6) воздушно-пылевой
7) при укусе животного
Назовите препараты, применяемые для профилактики и этиотропного лечения гриппа:
1) ацикловир
2) живая вакцина
3) антибиотики
4) ремантадин
5) интерферон
6) убитая вакцина
7) специфический гамма-глобулин
Укажите источники и пути передачи дифтерии для человека:
1) домашние животные
2) человек-носитель нетоксигенных штаммов возбудителя
3) больные дифтерией люди
4) воздушно-капельный путь
5) алиментарный путь
6) контактно-бытовой путь
7) носители токсигенных штаммов возбудителя
Нарушение нормальной микрофлоры кишечника приводит к:
острому пищевому отравлению
дисбактериозу
кандидомикозу
дизентерии
авитаминозу
Какие препараты используются для активной иммунизации?
1) менингококковая вакцина
2) АКДС
3) противодифтерийная сыворотка
4) интерферон
5) иммуноглобулин человека нормальный
Механизмы специфического иммунитета - это:
1) иммуноглобулины
2) Т-киллеры
3) опсонины
4) бета-лизины
5) естественные киллеры
Антитела – это:
1) альбумины
2) гаммаглобулины
3) бета-глобулины
4) фибриноген
5) трансферраны
Структурные и функциональные особенности иммуноглобулинов класса IgG:
1) мономер
2) пентамер
3) константа седиментации 19s
4) образуются при первичном ответе
5) разрушаются под действием меркамина и цистеина
6) проходят через плаценту
Структурные и функциональные особенности иммуноглобулинов класса IgM:
1) пентамер
2) мономер
3) образуются при первичном иммунном ответе
4) константа седиментации 7s
5) проходят через плаценту
6) разрушаются под действием меркамина и цистеина
Живыми вакцинами являются:
1) БЦЖ
2) лактобактерин
3) полиомиелитная пероральная вакцина
4) коревая вакцина
5) вакцина гепатита А "ГЕП-А-ИНВАК"
6) вакцина гепатита В рекомбинантная
Укажите место расположения мышечной лакуны.
1) большое седалищное отверстие
2) малое седалищное отверстие
3) позади паховой связки
4) медиальнее подвздошно-гребенчатой дуги
Укажите анатомические структуры проходящие через мышечную лакуну.
1) грушевидная мышца
2) подвздошно-поясничная мышца
3) гребенчатая мышца
4) бедренный нерв
Укажите структуры, образующие стенки бедренного канала.
1) паховая связка
2) поперечная фасция
3) бедренная вена
4) глубокая пластинка широкой фасции
Укажите образования, ограничивающие поверхностное кольцо бедренного канала.
1) семенной канатик
2) подвздошно-гребенчатая дуга
3) паховая связка
4) серповидный край решетчатой фасции
Укажите части пищевода.
1) головная часть
2) шейная часть
3) грудная часть
4) брюшная часть
Что прилежит к пищеводу спереди?
1) аорта
2) трахея
3) перикард
4) тимус
Какие структуры участвуют в образовании поверхностного кольца пахового канала?
1) паховая связка
2) загнутая связка
3) гребенчатая связка
4) межножковые волокна
Укажите анатомические сужения пищевода.
1) диафрагмальное
2) желудочное
3) аортальное
4) глоточное
Какие связки берут начало от большой кривизны желудка?
1) желудочно-диафрагмальная
2) печеночно-желудочная
3) желудочно-ободочная
4) желудочно-селезеночная
Какие слои имеет мышечная оболочка желудка?
1) наружный круговой слой
2) внутренние косые волокна
3) средний круговой слой
4) наружный продольный слой
Какие анатомические образования находятся в месте перехода желудка в двенадцатиперстную кишку?
1) заслонка привратника
2) угловая вырезка
3) сфинктер привратника
4) сфинктер стенки желудка
Укажите основные формы желудка.
1) форма крючка
2) форма рога
3) форма веретена
4) форма чулка
Какие отделы выделяют у тонкой кишки?
1) подвздошная кишка
2) тощая кишка
3) слепая кишка
4) двенадцатиперстная кишка
Назовите части двенадцатиперстной кишки.
1) восходящая часть
2) горизонтальная часть
3) нисходящая часть
4) верхняя часть
В какой части двенадцатиперстной кишки располагается большой сосочек?
1) верхняя часть
2) горизонтальная часть
3) нисходящая часть
4) восходящая часть
Какие протоки открываются на большом сосочке двенадцатиперстной кишки?
1) проток поджелудочной железы
2) добавочный проток поджелудочной железы
3) общий желчный проток
4) общий печеночный проток
Какая часть двенадцатиперстной кишки располагается интраперитонеально?
1) нисходящая часть
2) ампула (луковица) двенадцатиперстной кишки
3) восходящая часть
4) горизонтальная часть
Какие части выделяют в прямой кишке?
1) надампулярный отдел
2) ампула
3) перешеек
4) анальный отдел
Назовите части желчного пузыря.
1) основание
2) дно
3) тело
4) шейка
Какие протоки образуют общий печеночный проток?
1) пузырный проток
2) правый печеночный проток
3) левый печеночный проток
4) общий желчный проток
Какие части выделяют у поджелудочной железы?
1) хвост
2) крючковидный отросток
3) головку
4) тело
С какими органами соприкасается головка поджелудочной железы?
1) поперечная ободочная кишка
2) желудок
3) правая почка
4) двенадцатиперстная кишка
Какое положение занимает поджелудочная железа по отношению к брюшине?
1) интраперитонеальное положение
2) мезоперитонеальное положение
3) экстраперитонеальное положение
4) интраперитонеальное положение, при наличии брыжейки
Для изучения тонкой кишки методом динамического наблюдения за продвижением бария из желудка до слепой кишки требуется:
30-45 мин
1,5-2,5 часа
3-5 часов
Двенадцатиперстная кишка имеет форму:
удлиненной трубки
подковы
крючка
При ахалазии пищевода наблюдается:
1) ограниченное увеличение тени пищевода
2) общее равномерное увеличение тени пищевода
3) частичное равномерное увеличение тени
Супрастенотическое расширение развивается при:
1) раке пищевода
дивертикуле пищевода
доброкачественной опухоли пищевода
Симптом «ниши» характерен для:
1) опухоли желудка
язвы желудка
3) полипа желудка
В каком случае накладывается первично-отсроченный шов на рану?
1) если у больного шок
2) в случае массивной кровопотери
3) при возможности развития инфекции в ране
4) в случае невозможности стянуть края раны при ПХО
5) при ранении нерва
В какой ране более вероятно развитие инфекции?
1) резаной
2) укушенной
3) колотой
4) рубленной
5) размозженной
С какой целью применяются протеолитические ферменты при лечении ран?
1) расплавить некротизированные ткани
2) усилить действие антибиотиков
3) уменьшить воспаления
4) усилить рост грануляций
5) ускорить эпителизацию
Противопоказанием к гемотрансфузии являются
1) тяжелая операция
2) хирургическая инфекция
3) шок
4) тяжелое нарушение функции печени
5) снижение АД
Какова техника наложения позднего вторичного шва?
1) игла с ниткой проводится через грануляции
2) игла с ниткой проводится под грануляции
3) иссекаются дно и края раны на всю глубину до здоровых тканей
4) сшиваются кожные края
5) освежеваются грануляции и мобилизуются кожные края раны
В какие сроки накладывается поздний вторичный шов?
1) до 3-4 дней
2) от 3-4 до 7-8 дня
3) от 8-9 до 15-16 дня
4) от 15-16 дня и позже
5) сразу после хирургической обработки
Необходимое условие обуславливающее первичное заживление раны?
1) плотное соприкосновение краев раны
2) наличие в ране кровяных сгустков
3) наличие в ране инородного тела
4) наличие в ране дренажа
5) наличие в ране инфекции 105 на грамм ткани
За счет чего происходит сближение краев раны в естественных условиях?
1) размножение клеток
2) активного роста сосудов
3) нарастания эпителия отторжения мертвых тканей
4) процесса стягивания фиброзной ткани в раневом канале
5) отторжение мертвых тканей
Какое из перечисленных заболеваний чаще всего осложняется гнойной инфекцией?
1) злокачественная опухоль
2) пороки сердца
3) сахарный диабет
4) хроническая почечная недостаточность
5) закрытая травма головного мозга
Какова глубина разреза при вскрытии гнойника пространства Пирогова-Парона?
1) по подкожной клетчатки
2) до поверхностной фасции предплечья
3) до глубокого сгибателя пальцев
4) до поверхностного сгибателя пальцев
5) до квадратного пронатора
Среди осложнений подкожного панариция 5 пальца кисти не встречаются:
1) сухожильный панариций
2) костный панариций
3) суставной панариций
4) бурсит локтевого сустава
5) флегмона предплечья
Парапроктит - это воспаление:
1) геморроидальный узлов
2) заднепроходного сфинктера
3) слизистой прямой кишки
4) околопрямокишечной клетчатки
5) подкожной клетчатки ягодичной области
Верно ли, что по глубине локализации различают парапроктит подкожный, подслизистый, седалищный, тазово-прямокишеный:
1) да
2) нет
Проба на индивидуальную совместимость крови проводится между
1) плазмой реципиента и кровью донора
2) плазмой донора и кровью реципиента
3) форменными элементами крови реципиента и кровью донора
4) форменными элементами крови донора и кровью реципиента
5) цельной кровью донора и цельной кровью реципиента
Всякому отморожению сопутствует:
1) общее переохлаждение
2) развитие инфекции вдп
3) нарушения со стороны цнс
4) гипопротеинемия
5) анемия
Что первично при отморожениях:
1) нарушение перфузии тканей
2) первичный некроз тканей
3) гипоксемия
4) нарушение мышечного тонуса
При каком заболевании может развиться холодный абсцесс:
1) остеомиелите
2) пандактилите
3) туберкулёзном спондилите
4) фурункулёзе
5) антиномикозе
Симптом флуктуации не определяется при:
1) подкожной гематоме
2) абсцессе
3) флегмоне
4) гемотораксе
5) гнойном бурсите
Основным отличием эризипелоида от панариция является
1) отсутствие гипертермии
2) наличие гиперемии кожи и отека пальца
3) отсутствие локальной болезненности
4) выраженный зуд в области припухлости
5) правильно 3 и 4
6) правильно 1 и 2
При рецидивирующей роже нижних конечностей наиболее частое осложнение
1) остеомиелит
2) тромбофлебит
3) периостит
4) лимфостаз
5) сепсис
Выберете неправильный ответ в перечислении форм панарициев:
1) кожный
2) подкожный
3) сухожильный
4) костный
5) ладонный
Что такое паронихия?
1) воспаление всех тканей пальца
2) воспаление околоногтевого валика
3) воспаление околоногтевого ложа
4) воспаление межфалангового сустава
5) воспаление сухожильного влагалища пальца
Больной с подкожным панарицием 2 пальца кисти провел бессонную ночь из-за мучительных болей. Ваша тактика при лечении такого больного?
1) спиртовые ванночки и компрессы
2) повязки с мазями
3) кварцевое облучение и УВЧ
4) антибиотикотерапия
5) разрез, дренирование, иммобилизация
Пандактилит - это гнойное воспаление:
1) ногтя
2) подкожной клетчатки
3) околоногтевого валика
4) сухожильного влагалища пальца
5) всех тканей пальца
Какай разрез выполняется при вскрытии ретромаммарного гнойника?
1) радиарный в верхней половине железы
2) циркуляция около соска
3) радиарный в нижней половине железы
4) полуовальный над верхним краем железы
5) полуовальный по переходной складке железы
Буллёзная форма рожи характеризуется наличием:
1) абсцессов
2) пустул
3) пузырей
4) язв
5) участков некроза в коже
При исследовании крови у больного рожистым воспалением отмечается:
1) лейкоцитоз с нейтрофилёзом
2) лимфоцитоз
3) эозинофилия
4) тромбоцитопения
5) гиперглобулинемия
Вовлечение в процесс подкожной клетчатки при рожистом воспалении ведёт к развитию:
1) некроза
2) флегмоны подкожной клетчатки
3) сепсиса
4) карбункула
5) абсцесса
Возникновению рожистого воспаления способствует:
1) травмы, охлаждение
2) гидраденит
3) лимфаденит
4) опухоли кожу
5) аллергия
Из общих методов лечения при рожистом воспалении наиболее эффективно применение:
1) сульфаниламидных препаратов
2) аспирина
3) физиотерапевтических процедур
4) антибиотиков и сульфаниламидных препаратов
5) рентгенотерапии
При роже противопоказаны:
1) антибиотики
2) сульфаниламидные препараты
3) УФ-облучение
4) рентгенотерапия
5) влажные повязки и ванны
Возбудителем эризипелоида является:
1) стафилококк
2) стрептококк
3) палочка свиной краснухи
4) протей
По течению различают следующие формы эризипелоида:
1) острую, подострую и хроническую
2) острую, хроническую и рецидивирующую
3) флегмонозную, эритематозную
4) эритематозную, буллёзную, флегмонозную
5) острую, рецидивирующую, септическую
Основным симптомом перитонита является:
1) рвота
2) боль в животе
3) кровавый стул
4) задержка стула и газов
5) напряжение мышц передней брюшной стенки
Патологический процесс при эризипелоиде локализуется на:
1) пальцах кисти
2) предплечье
3) пальцах стопы
4) лице
5) голени
Одним из важных компонентов лечения сепсиса является:
1) массаж
2) антибиотикотерапия
3) лечебная физкультура
4) физиотерапевтические процедуры
5) витаминотерапия
К осложнениям сепсиса не относятся:
1) пневмонию
2) пролежни
3) тромбоэмболию
4) кахексию
5) геморрагии
Что является наиболее важным в лечении сепсиса?
1) строгий постельный режим
2) тщательный сбор анамнеза
3) лечение сопутствующего заболевания
4) ликвидация первичного очага
5) выявление наследственного фактора
Дозы крови, переливаемой с гемостатической целью:
1) 100 мл
2) 200 мл
3) 500 мл
4) 1000 мл
5) ни одна из указанных доз
Противопоказания к переливанию крови:
1) тяжелые операции
2) хирургическая инфекция
3) шок
4) тяжелые нарушения функции печени
5) снижение артериального давления
Характер оперативного вмешательства при прободной язве желудка определяет:
1) возраст больного
2) локализация перфоративного отверстия
3) степень выраженности перитонита
4) срок с момента перфорации
5) все перечисленное
Для острой высокой кишечной непроходимости не характерно:
1) быстрое снижение ОЦК
2) неукротимая рвота
3) вздутие живота в первые часы заболевания
4) быстрое обезвоживание
5) схваткообразные боли
Для флеботромбоза подвздошно-бедренного сегмента не характерно:
1) гиперемия кожи бедра в области прохождения вен
2) отек стопы и голени
3) распирающие боли в бедре
4) увеличение объема бедра и голени
5) цианотичность кожи бедра
При развитии пиопневмоторакса при абсцессе легкого в первую очередь показано:
1) эндобронхиальное введение протеолитических ферментов
2) дренирование плевральной полости
3) антибиотики
4) рентгенотерапия
5) введение цитостатиков
Наиболее информативным методом диагностики кисты поджелудочной железы является:
1) ЭРХПГ
2) исследование пассажа бария по кишечнику
3) биохимическое исследование
4) УЗИ
5) ничто из названного
Наиболее частой причиной острого артериального тромбоза является:
1) облитерирующий тромбангит
2) облитерирующий атеросклероз
3) пункция и катетеризация артерий
4) экстравазальная компрессия артерий
5) полицитемия
Укажите оптимальный объем операции при кровотечении из вен пищевода на фоне внутрипеченочной формы портальной гипертензии:
1) прошивание вен пищевода
2) портокавальный анастомоз
3) спленэктомия
4) склерозирование вен пищевода
Рак Панкоста - это:
1) центральный рак средней доли
2) периферический рак нижней доли
3) центральный рак верхней доли
4) периферический рак верхушки легкого
5) полостная форма периферического рака легкого
При абсцессе Дугласова пространства показано:
1) пункция через брюшную стенку
2) лечебные клизмы
3) вскрытие через брюшную стенку
4) пункция, вскрытие и дренирование через прямую кишку
5) консервативное лечение
Наиболее частым осложнением язвы передней стенки 12-перстной кишки является:
1) перфорация
2) кровотечение
3) пенетрация в головку поджелудочной железы
4) малигнизация
5) все неверно
99. В лечении разлитого перитонита аппендикулярного происхождения основное значение имеет:
1) устранение источника перитонита
2) антибактериальная терапия
3) коррекция водно-электролитных нарушений
4) санация брюшной полости
5) все перечисленное верно
Не характерным для синдрома Педжета - Шреттера является:
1) цианоз лица и шеи
2) распирающие боли в руке
3) цианоз кожи руки, усиление венозного рисунка
4) отек руки
5) все перечисленные признаки характерны
Вариант 4.
Превращение пепсиногена в пепсин активируют:
1) гастрин
2)энтерокиназа
3) HCl
Гастрин образуется в одном из отделов желудка:
1) фундальном
2) кардиальном
3) пилорическом
В активном состоянии вырабатываются ферменты поджелудочной железы:
1) трипсиноген, химотрипсиноген
2) прокарбоксиполипептидазы
3) амилаза, липаза, нуклеазы
При закупорке выводных желчных протоков нарушается всасывание веществ:
1) моносахаридов
2) высших жирных кислот
3) аминокислот
4) алкоголя
5) витамина С
Секретин стимулирует выделение поджелудочного сока, в котором преобладают:
1) ферменты
2) слизь
3) бикарбонаты
Диурез - это:
1) объем вторичной мочи, образующейся в единицу времени
2) объем первичной мочи, образующейся в единицу времени
3) объем первичной мочи, реабсорбирующейся в единицу времени
4) объем мочи, поступающей в единицу времени в собирательные трубки
К неспецифическим гуморальным факторам защиты относятся:
1) агглютинины
2) комплемент
3) пропердиновая система
4) бета-лизины
5) бактериолизины
Основные функции фагоцитов:
1) защитная (уничтожение микробов)
2) участие в иммунном ответе (презентация антигена)
3) секреторная (лизосомальные ферменты, интерферон)
4) продукция антител
5) продукция интерлейкина-2
К факторам естественной резистентности относятся:
1) специфические антитела
2) интерферон
3) нормальные (естественные) киллеры
4) фагоцитоз
5) комплемент
Вакцины - это препараты, содержащие:
1) живых вирулентных возбудителей
2) убитых микробов
3) микробные токсины
4) живых возбудителей со сниженными вирулентными свойствами
5) бактериальные протективные антигены
Какие микроорганизмы вызывают синегнойную инфекцию?
1) P.mallei
2) P.aeruginosa
3) P.vulgaris
4) P.stuartii
5) P.haemolytica
6) P.putida
Какой материал нужно взять у пациента для выявления стафилококкового носительства?
1) кровь
2) раневое отделяемое
3) фекалии
4) слюна
5) мокрота
6) слизь из носа
7) слизь из зева
Реакция Вассермана и реакция микропреципитации положительны чаще всего у больных сифилисом в следующие периоды болезни:
1) инкубационном
2) твердого шанкра
3) генерализации
4) гуммозном
5) нейросифилиса
Где открывается добавочный проток поджелудочной железы?
1) большой сосочек двенадцатиперстной кишки
2) малый сосочек двенадцатиперстной кишки
3) печеночно-поджелудочная ампула
4) продольная складка двенадцатиперстной кишки
Укажите связки печени.
1) серповидная связка
2) круглая связка
3) венечная связка
4) левая треугольная связка
Какие органы (из перечисленных) занимают экстраперитонеальное положение?
1) желудок
2) поджелудочная железа
3) печень
4) надпочечник
Укажите непарные висцеральные ветви брюшной части аорты.
1) чревный ствол
2) верхняя прямокишечная артерия
3) нижняя брыжеечная артерия
4) средняя ободочная артерия
Укажите ветви чревного ствола.
1) левая желудочная артерия
2) правая желудочная артерия
3) верхняя брыжеечная артерия
4) селезеночная артерия
Укажите артерии желудка, отходящие от селезеночной артерии.
1) правая желудочная артерия
2) левая желудочно-сальниковая артерия
3) правая желудочно-сальниковая артерия
4) короткие желудочные артерии
Укажите ветви общей печеночной артерии.
1) правая желудочно-сальниковая артерия
2) левая желудочно-сальниковая артерия
3) желудочно-дуоденальная артерия
4) левая желудочная артерия
Укажите, на уровне какого позвонка берет начало нижняя полая вена.
1) третий поясничный позвонок
2) первый крестцовый позвонок
3) четвертый-пятый поясничные позвонки
4) крестцово-подвздошный сустав
Укажите анатомические образования, которые располагаются позади нижней полой вены.
1) головка поджелудочной железы
2) симпатический ствол
3) двенадцатиперстная кишка
4) правая почечная артерия
Укажите вены, впадающие в нижнюю полую вену.
1) поясничная вена
2) нижняя брыжеечная вена
3) почечная вена
4) селезеночная вена
Укажите вены, относящиеся к висцеральным притокам нижней полой вены.
1) надпочечниковые вены
2) нижние диафрагмальные вены
3) яичковая (яичниковая) вена
4) почечные вены
Укажите органы, от которых венозная кровь оттекает в воротную вену.
1) диафрагма
2) печень
3) кишечник
4) почки
Укажите глубокие вены нижней конечности.
1) бедренная вена
2) большая подкожная вена
3) подколенная вена
4) передние большеберцовые вены
Укажите вену, в которую впадает малая подкожная вена.
1) большая подкожная вена
2) бедренная вена
3) задняя большеберцовая вена
4) подколенная вена
Укажите место впадения лимфатических протоков в кровеносное русло.
1) плечеголовная вена
2) венозный угол
3) наружная яремная вена
4) внутренняя яремная вена
Укажите, какие анатомические образования включает лимфатическая система.
1) лимфоидные фолликулы
2) лимфатические капилляры
3) лимфатические сосуды
4) лимфатические стволы и сосуды
Укажите место впадения лимфатических протоков в кровеносное русло.
1) плечеголовная вена
2) венозный угол
3) наружная яремная вена
4) внутренняя яремная вена
Укажите органы, к которым подходят вегетативные волокна от блуждающего нерва.
1) матка
2) тонкая кишка
3) мочевой пузырь
4) желудок
Какие нервы принимают участие в иннервации желудка?
1) симпатические
2) парасимпатические
3) поясничные спинномозговые нервы
4) крестцовые нервы
От каких нервных структур иннервируется желудок.
1) блуждающий нерв
2) большой чревный нерв
3) диафрагмальный нерв
4) узлы чревного сплетения
При пневмотораксе прозрачность легочного поля на стороне поражения:
понижена
повышена
не изменена
Легочный рисунок при пневмотораксе на стороне поражения:
избыточный
обедненный
отсутствует
Легочный рисунок образован:
бронхиальными ветвями
лимфатическими сосудами
кровеносными сосудами
При дренированном абсцессе определяется тень:
однородная интенсивная
кольцевидная
неоднородная, просветление с горизонтальным уровнем жидкости
Для периферического рака легкого характерно:
затемнение с ровными контурами
затемнение с неровными контурами
затемнение с нечеткими контурами
Альбуминозный остеомиелит L.Ollier (Оллье) обычно локализуется
1) в дистальных отделах бедра
2) в дистальных отделах большеберцовой кости
3) в проксимальных отделах плеча
Склерозирующий остеомиелит C.Garre (Гарре) начинается обычно:
1) остро
2) подостро
Консервативное лечение при хроническом остеомиелите обычно:
1) может иметь самостоятельное значение
2) осуществляется в комплексе с оперативным
3) не имеет существенного значения
Целью операции секвестрэктомии является:
1. ликвидация костной полости
2. иссечение свища
3. устранение основного источника гнойно-воспалительного процесса
Заполнение остаточной костной полости по M.Schede (1886) производится:
1) близлежащей мышцей
2) кровяным сгустком
3) полимерами
4) костными фрагментами
Местные симптомы хронического гематогенного остеомиелита:
1) бледность кожных покровов,
2) нарушение периферической иннервации
3) отсутствие пульса на артериях
4) отслойка эпидермиса,
5) наличие свищей с гнойно-геморрагическим отделяемым
Общие симптомы хронического гематогенного остеомиелита:
1) слезотечение
2) судороги
3) затруднение глотания пищи
5) повышение температуры тела
Основа в лечении хронического гематогенного остеомиелита:
1) введение антибиотиков
2) общеукрепляющее лечение
3) введение склерозирующих растворов
4) рентгенотерапия
5) оперативное лечение
К первично хроническому остеомиелиту (атипичные формы) относятся:
1) остеомиелит Оллье
2) остеомиелит Гарре
3) поднадкостничный абсцесс
4) правильно 1 и 2
5) правильно 3 и 6
6) антибиотический остеомиелит
Хронический остеомиелит характеризуется следующими основными признаками:
1) рецидивирующее течение
2) наличие секвестра (или остеомиелитической полости)
3) интоксикацией
4) гнойным свищом
5) всем перечисленным
Радикальными операциями в плановом порядке при хроническом остеомиелите являются:
1) секвестрэктомия
2) секвестрнекрнекрэктомия
3) резекция кости в пределах здоровых тканей
Для газовой гангрены характерно все, кроме:
1) воспалительная реакция, отёк, интоксикация
2) отсутствие воспалительной реакции, отёк, некроз
3) сухой струп в области раны
4) зияющая рана с гнилостным экссудатом
5) лейкоцитоз, бактериемия
Для экстренной профилактики столбняка применяют:
1) введение противостолбнячного анатоксина
2) введение антибиотиков
3) баротерапию
4) активно-пассивную профилактику - введение противостолбнячного анатоксина и введение противостолбнячной сыворотки
5) введение противостолбнячной сыворотки
Выберете неправильный ответ в перечислении доброкачественных опухолей:
1) липома
2) фиброма
3) лейомиома
4) меланома
5) лимфангиома
Ранними симптомами столбняка являются:
1) быстро прогрессирующий отёк
2) сардоническая улыбка, опистотонус
3) брадикардия, понижение температуры тела, сухость кожных покровов
4) подёргивание мышц в области раны, гипертермия
5) потеря сознания, паралич
Явным признаком столбняка является:
1) бред
2) декомпенсация сердечно-сосудистой системы
3) анемия
4) сардоническая улыбка
5) циклически повторяющиеся приступы лихорадки
Профилактика столбняка не проводится при:
1) ожогах и отморожениях 2-3 степенях
2) открытом переломе, разрыве мышц и сухожилий
3) парапроктите
4) криминальном аборте
5) ножевом ранении
Основной симптом столбняка это:
1) затруднение при открывании рта
2) тяжесть в мышцах затылка
3) эйфория
4) плохой сон
5) судороги
Выберете неправильный ответ в перечислении признаков рака желудка:
1) отсутствие аппетита
2) тошнота
3) рвота
4) дефект слизистой желудка
5) боли в эпигастрии спастического характера
Выберете неправильный ответ в приведенном перечне признаков рака лёгкого.
1) надсадный кашель
2) повышение температуры тела
3) затемнение в лёгком при рентгеноскопии
4) изменение эпителия бронха, обнаруженное бронхоскопически
5) отсутствие опухолевых клеток в изменённой ткани
Гидраденит - это воспаление:
1) сальных желёз
2) потовых желёз
3) волосяного мешочка
4) лимфатического сосуда
5) лимфоузла
Назовите место обычной локализации гидраденита?
1) подмышечная впадина
2) подчелюстная область
3) шея
4) спина
5) лицо
Какую пробу не проводят с кровью донора пред каждым переливанием крови?
1) групповая совместитмость
2) индивидуальная совместимость
3) биологическая проба
4) определение резус-совместимости
5) определение резус-фактора
Свободная кожная пластика при глубоких ожогах возможна:
1) уже в период ожогового шока
2) после выполнения ожогового дефекта грануляциями
3) сразу после химического некроза струпа
4) как правило, через 1-2 недели после травмы
5) не ранее 4-5 недель с момента ожога
Сколько раз обрабатывается операционное поле раствором антисептика
1) 1
2) 2
3) 4
4) 3
Парами формалина следует стерилизовать?
1) режущие инструменты
2) резиновые перчатки
3) инструменты с оптическими системами
4) марлевые салфетки
5) шприцы
Минимальная температура, вызывающая гибель спороносных бактерий?
1) 60о
2) 80о
3) 100о
4) 120о
5) 140о
Гипертонический раствор хлорида натрия применяют при:
1) первичной хирургической обработке раны
2) наложение согревающего компресса
3) стерилизация режущих инструментов
4) лечение гнойных ран
5) лечение рожистого воспаления
Обработка рук хирурга раствором первомура длится
1) 1 мин
2) 2 мин
3) 3 мин
4) 5 мин
5) 10 мин
Под стерилизацией понимают:
1) уничтожение патогенных микроорганизмов
2) частичное уничтожение патогенных микроорганизмов
3) уничтожение отдельных видов микроорганизмов
4) уничтожение микроорганизмов всех видов находящихся на всех стадиях развития
Что из перечисленного не относится к профилактике воздушной инфекции?
1) УФ-стерилизация воздуха
2) обработка операционного поля
3) проветривание
4) уборка операционного зала
5) ношение маски
Где категорически (по соображениям асептики) нельзя стоять и даже проходить в операционном зале во время операции?
1) за спиной хирурга на расстоянии 1 м
2) между анестезиологом и капельницей
3) между столиком операционной сестры и большим инструментальным столом
4) головным концом операционного стола и входной дверью
5) между наркозным аппаратом и капельницей
Что из перечисленного не относится к средствам холодовой стерилизации:
1) ультрафиолетовые лучи
2) ионизирующее облучение
3) ультразвуковые волны
4) пары формалина
5) автоклавирование
Для оценки качества предстерилизационной очистки инструментов на предмет наличия крови используют следующие пробы:
1) амидопириновая
2) фенолфталеиновая
3) азопирамовая
4) бензидиновая
К химическим антисептикам не относятся следующие вещества:
1) риванол
2) перекись водорода
3) сульфат бария
4) формальдегид
5) йодонат
Слайдж-синдром - это:
1) миграция лейкоцитов и эритроцитов за пределы сосудистой стенки
2) пристеночное расположение лейкоцитов
3) сгруппирование эритроцитов в виде монетных столбиков
4) макрогематурия
5) микрогематурия
Кровопотеря лёгкой степени - это потеря:
1) до 50 мл. крови
2) до 100мл крови
3) до 500 мл крови
4) до 750 мл крови
5) до 1000 мл крови
Кровопотеря тяжелой степени - это потеря:
1) до 500 мл крови
2) до 750 мл крови
3) до 1000 мл крови
4) свыше 1500 мл крови
При каком виде кровотечения существует реальная опасность воздушной эмболии:
1) повреждении артерии бедра
2) повреждении лучевой артерии
3) капиллярное кровотечение
4) повреждение вен голени
5) повреждение вен шеи
При каком кровотечении наблюдается пенистая кровь?
1) носовое
2) пищеводное
3) лёгочное
4) кишечное
В какие сроки производят плановые вмешательства:
1) первые сутки после госпитализации
2) сразу же после установления диагноза
3) первые часы после госпитализации
4) после тщательного обследования пациента и тщательной предоперационной подготовки
5) сроки определяются самим пациентом
Чем срочные вмешательства отличаются от экстренных:
1) есть возможность выполнить клиническое обследование, минимальную подготовку и ряд клинических тестов
2) при срочном вмешательстве диагноз заболевания четко установлен
3) экстренные вмешательства преследуют только цель спасти жизнь пациента
4) при срочных вмешательствах никогда не проводят гемотрансфузии
5) срочные вмешательства позволяют выполнить радикальные операции
Выберете путь, который никогда не используется для гемотрансфузии:
1) подкожный
2) внутривенный,
3) внутрикостный
4) внутриартериальный
Проникающей резаной раной живота называется рана с повреждением:
1) кожи
2) мышц
3) париетальной брюшины
4) висцеральной брюшины
5) внутренних органов
Ценкеровский дивертикул пищевода локализуется:
1) в области бифуркации трахеи
2) над диафрагмой
3) в верхней трети пищевода
4) в глоточно-пищеводном переходе
5) над кардией
Наиболее характерными для острого панкреатита являются боли:
1) ноющие
2) опоясывающие
3) схваткообразные
4) кинжальные
5) тупые
Основным симптомом перитонита является:
1) рвота
2) боль в животе
3) кровавый стул
4) задержка стула и газов
5) напряжение мышц передней брюшной стенки
Основным признаком скользящей грыжи брюшной стенки является:
1) легкая вправляемость
2) врожденная природа
3) одной из стенок грыжевого мешка является орган брюшной полости, частично покрытый брюшиной
4) проникновение между мышцами и апоневрозом
5) все перечисленное верно
Синдром Лериша - это:
1) брахиоцефальный неспецифический артериит
2) атеросклеротическая хроническая окклюзия бифуркации брюшной аорты
3) капилляропатия дистальных отделов конечности
4) мигрирующий тромбангиит
5) окклюзия нижней полой вены
В лечении разлитого перитонита аппендикулярного происхождения основное значение имеет:
1) устранение источника перитонита
2) антибактериальная терапия
3) коррекция водно-электролитных нарушений
4) санация брюшной полости
5) все перечисленное верно
Для флеботромбоза подвздошно-бедренного сегмента не характерны:
1) гиперемия кожи бедра в области прохождения вен
2) отек стопы и голени
3) распирающие боли в бедре
4) увеличение объема бедра и голени
5) цианотичность кожи бедра
Зоб у лиц одной биогеохимической области определяется как:
1) эпидемический
2) спорадический
3) острый струмит
4) эндемический
5) массовый тиреотоксикоз
Рихтеровским называется ущемление:
1) пристеночное
2) сигмовидной кишки в скользящей грыже
3) желудка в диафрагмальной грыже
4) дивертикула Меккеля
5) червеобразного отростка
Наиболее информативным методом диагностики кисты поджелудочной железы является:
1) ЭРПХГ
2) исследование пассажа бария по кишечнику
3) биохимическое исследование
4) УЗИ
5) ничто из названного
При рецидиве язвенного гастродуоденального кровотечения показана:
1) экстренное хирургическое вмешательство
2) срочное хирургическое вмешательство
3) эндоваскулярная селективная гемостатическая терапия
4) повторная эндоскопическая гемостатическая терапия
5) интенсивная консервативная гемостатическая терапия
Укажите наиболее часто встречающуюся причину синдрома портальной гипертензии:
1) синдром Бадда-Киари.
2) болезнь Киари.
3) цирроз печени с внутрипеченочным блоком кровотока.
4) триада Сента.
5) подпеченочный блок кровотока.
Какой из методов бужирования пищевода является наиболее безопасным?
1) ортоградное бужирование вслепую;
2) бужирование под контролем эзофагоскопа;
3) ретроградное бужирование за нитку;
4) ортоградное бужирование по струне полыми рентгеноконтрастными бужами;
5) ортоградное бужирование по нитке-направителю
В лечении разлитого перитонита аппендикулярного происхождения основное значение имеет:
1) устранение источника перитонита
2) антибактериальная терапия
3) коррекция водно-электролитных нарушений
4) санация брюшной полости
5) все перечисленное верно
Заражение свиной рожей происходит:
1) гематогенным путём
2) при переливании крови
3) при инъекциях
4) воздушно-капельным путём
5) контактным путём
Больному с гангренозным холециститом показано:
1) консервативное лечение
2) отсроченная операция
3) принятие решения зависит от возраста больного
4) операция при отсутствии эффекта от консервативной терапии
5) экстренная операция
К интраоперационным методам исследования внепеченочных желчных путей относится все, кроме:
1) пальпации холедоха
2) холедохоскопии
3) интраоперационной холангиографии
4) зондирования холедоха
5) внутривенной холангиографии
К осложнениям варикозной болезни относят:
1) пигментацию кожи
2) индурацию подкожной клетчатки
3) трофические язвы
4) тромбофлебит
5) все перечисленное
О Т В Е Т Ы
На тестовый контроль исходного уровня знаний
1 Вариант
№ вопроса |
Ответ |
|
№ вопроса |
Ответ |
1 |
3 |
|
51 |
2 |
2 |
4 |
|
52 |
1 |
3 |
4 |
|
53 |
5 |
4 |
3 |
|
54 |
1 |
5 |
5 |
|
55 |
5 |
6 |
1,3,4,5 |
|
56 |
2 |
7 |
1,4,5,6 |
|
57 |
3 |
8 |
1 |
|
58 |
3 |
9 |
1,3,4,5 |
|
59 |
4 |
10 |
2,3,5 |
|
60 |
1 |
11 |
2,3 |
|
61 |
4 |
12 |
2,3,5 |
|
62 |
3 |
13 |
1,2 |
|
63 |
4 |
14 |
2,3 |
|
64 |
3 |
15 |
2 |
|
65 |
4 |
16 |
1,2,3,5 |
|
66 |
5 |
17 |
1,3 |
|
67 |
2 |
18 |
2,3,4,5 |
|
68 |
2 |
19 |
2,3,5 |
|
69 |
2 |
20 |
3 |
|
70 |
3 |
21 |
3 |
|
71 |
3 |
22 |
1,3 |
|
72 |
4 |
23 |
3 |
|
73 |
1 |
24 |
2 |
|
74 |
4 |
25 |
1,2,3,4 |
|
75 |
5 |
26 |
1,2,3,4 |
|
76 |
5 |
27 |
3 |
|
77 |
5 |
28 |
1,3,4 |
|
78 |
5 |
29 |
4 |
|
79 |
2 |
30 |
4 |
|
80 |
1 |
31 |
2,4 |
|
81 |
5 |
32 |
3 |
|
82 |
2 |
33 |
3,4 |
|
83 |
5 |
34 |
3 |
|
84 |
4 |
35 |
1 |
|
85 |
5 |
36 |
2 |
|
86 |
3 |
37 |
2 |
|
87 |
4 |
38 |
1 |
|
88 |
1 |
39 |
1 |
|
89 |
1 |
40 |
1 |
|
90 |
3 |
41 |
2 |
|
91 |
5 |
42 |
4 |
|
92 |
2 |
43 |
2 |
|
93 |
5 |
44 |
2 |
|
94 |
2 |
45 |
1 |
|
95 |
3 |
46 |
2 |
|
96 |
4 |
47 |
2 |
|
97 |
3 |
48 |
3 |
|
98 |
5 |
49 |
2 |
|
99 |
4 |
50 |
3 |
|
100 |
3 |
О Т В Е Т Ы
На тестовый контроль исходного уровня знаний
2 Вариант
№ вопроса |
Ответ |
|
№ вопроса |
Ответ |
1 |
4 |
|
51 |
1 |
2 |
4 |
|
52 |
3 |
3 |
3 |
|
53 |
2 |
4 |
4 |
|
54 |
5 |
5 |
3 |
|
55 |
4 |
6 |
1,3,6 |
|
56 |
1 |
7 |
3,4,5 |
|
57 |
4 |
8 |
1,2,5,7 |
|
58 |
4 |
9 |
1,2,4 |
|
59 |
5 |
10 |
3 |
|
60 |
4 |
11 |
1,2,5 |
|
61 |
4 |
12 |
3,5 |
|
62 |
3 |
13 |
4,5,6,7,8 |
|
63 |
2 |
14 |
5,6 |
|
64 |
1 |
15 |
2,4,7 |
|
65 |
5 |
16 |
3,5 |
|
66 |
2 |
17 |
1,3,4,5,6 |
|
67 |
4 |
18 |
1,2,4 |
|
68 |
2 |
19 |
4 |
|
69 |
3 |
20 |
1,3,4 |
|
70 |
1 |
21 |
1,3,4 |
|
71 |
2 |
22 |
1,2 |
|
72 |
4 |
23 |
1,2,3,4 |
|
73 |
2 |
24 |
2,4 |
|
74 |
2 |
25 |
2,3,4 |
|
75 |
3 |
26 |
1,3,4 |
|
76 |
3 |
27 |
1,2,4 |
|
77 |
3 |
28 |
2,3,4 |
|
78 |
3 |
29 |
2,3 |
|
79 |
1 |
30 |
1,2,3,4 |
|
80 |
2 |
31 |
1,3 |
|
81 |
3 |
32 |
2,3 |
|
82 |
5 |
33 |
1,2,4 |
|
83 |
1 |
34 |
1,2 |
|
84 |
3 |
35 |
1,2,3,4 |
|
85 |
1 |
36 |
1,4 |
|
86 |
4 |
37 |
3 |
|
87 |
1 |
38 |
2 |
|
88 |
4 |
39 |
3 |
|
89 |
1 |
40 |
3 |
|
90 |
1 |
41 |
3 |
|
91 |
3 |
42 |
2 |
|
92 |
3 |
43 |
4 |
|
93 |
1 |
44 |
1 |
|
94 |
1 |
45 |
4 |
|
95 |
3 |
46 |
3 |
|
96 |
5 |
47 |
1 |
|
97 |
3 |
48 |
5 |
|
98 |
1 |
49 |
2 |
|
99 |
1 |
50 |
2 |
|
100 |
1 |
О Т В Е Т Ы
На тестовый контроль исходного уровня знаний
3 Вариант
№ вопроса |
Ответ |
|
№ вопроса |
Ответ |
1 |
4 |
|
51 |
1 |
2 |
4 |
|
52 |
4 |
3 |
2 |
|
53 |
5 |
4 |
3 |
|
54 |
4 |
5 |
4 |
|
55 |
1 |
6 |
2,3,5,7 |
|
56 |
4 |
7 |
2,3,5 |
|
57 |
3 |
8 |
1 |
|
58 |
5 |
9 |
1,2,4,6,7 |
|
59 |
4 |
10 |
2,5 |
|
60 |
4 |
11 |
5,7 |
|
61 |
1 |
12 |
2,4,5,6,7 |
|
62 |
1 |
13 |
3,4,5,6,7 |
|
63 |
1 |
14 |
2,3,5 |
|
64 |
1 |
15 |
1,2 |
|
65 |
3 |
16 |
1,2 |
|
66 |
4 |
17 |
2 |
|
67 |
5 |
18 |
1,6 |
|
68 |
4 |
19 |
1,3,6 |
|
69 |
5 |
20 |
1,3,4,6 |
|
70 |
2 |
21 |
3 |
|
71 |
5 |
22 |
2,4 |
|
72 |
5 |
23 |
1,3,4 |
|
73 |
5 |
24 |
4 |
|
74 |
3 |
25 |
2,3,4 |
|
75 |
1 |
26 |
2,3 |
|
76 |
2 |
27 |
1,2,4 |
|
77 |
1 |
28 |
1,3,4 |
|
78 |
4 |
29 |
1,3,4 |
|
79 |
5 |
30 |
2,3,4 |
|
80 |
3 |
31 |
1,3 |
|
81 |
2 |
32 |
1,2,4 |
|
82 |
5 |
33 |
1,2,4 |
|
83 |
1 |
34 |
1,2,3,4 |
|
84 |
2 |
35 |
3 |
|
85 |
2 |
36 |
1,3 |
|
86 |
4 |
37 |
2 |
|
87 |
2 |
38 |
1,2,4 |
|
88 |
4 |
39 |
2,3,4 |
|
89 |
5 |
40 |
2,3 |
|
90 |
3 |
41 |
1,2,3,4 |
|
91 |
1 |
42 |
3,4 |
|
92 |
2 |
43 |
3 |
|
93 |
4 |
44 |
2 |
|
94 |
2 |
45 |
2 |
|
95 |
1 |
46 |
2 |
|
96 |
4 |
47 |
1 |
|
97 |
4 |
48 |
2 |
|
98 |
1 |
49 |
3 |
|
99 |
5 |
50 |
2 |
|
100 |
1 |
О Т В Е Т Ы
На тестовый контроль исходного уровня знаний
4 Вариант
№ вопроса |
Ответ |
|
№ вопроса |
Ответ |
1 |
3 |
|
51 |
4 |
2 |
3 |
|
52 |
4 |
3 |
3 |
|
53 |
4 |
4 |
2 |
|
54 |
4 |
5 |
3 |
|
55 |
3 |
6 |
1 |
|
56 |
5 |
7 |
2,3,4 |
|
57 |
5 |
8 |
1,2,3 |
|
58 |
5 |
9 |
2,3,4,5 |
|
59 |
2 |
10 |
2,4,5 |
|
60 |
1 |
11 |
2 |
|
61 |
5 |
12 |
6,7 |
|
62 |
2 |
13 |
2,3 |
|
63 |
3 |
14 |
2 |
|
64 |
3 |
15 |
1,2,3,4 |
|
65 |
4 |
16 |
2,4 |
|
66 |
4 |
17 |
1,3 |
|
67 |
1 |
18 |
1,4 |
|
68 |
4 |
19 |
2,4 |
|
69 |
2 |
20 |
3 |
|
70 |
3 |
21 |
3 |
|
71 |
5 |
22 |
2,4 |
|
72 |
4 |
23 |
1,3 |
|
73 |
3 |
24 |
1,3 |
|
74 |
3 |
25 |
3 |
|
75 |
5 |
26 |
1,3,4 |
|
76 |
4 |
27 |
4 |
|
77 |
5 |
28 |
2,4 |
|
78 |
3 |
29 |
2,3,4 |
|
79 |
4 |
30 |
2,4 |
|
80 |
1 |
31 |
2,4 |
|
81 |
1 |
32 |
1,2 |
|
82 |
3 |
33 |
1,2,4 |
|
83 |
4 |
34 |
2 |
|
84 |
2 |
35 |
3 |
|
85 |
5 |
36 |
1 |
|
86 |
3 |
37 |
3 |
|
87 |
2 |
38 |
1 |
|
88 |
5 |
39 |
1 |
|
89 |
5 |
40 |
2 |
|
90 |
4 |
41 |
2 |
|
91 |
1 |
42 |
3 |
|
92 |
4 |
43 |
2 |
|
93 |
1 |
44 |
5 |
|
94 |
3 |
45 |
5 |
|
95 |
4 |
46 |
5 |
|
96 |
5 |
47 |
4 |
|
97 |
5 |
48 |
5 |
|
98 |
5 |
49 |
3 |
|
99 |
5 |
50 |
3 |
|
100 |
5 |
Тестовые задания для входного контроля (факультет иностранных студентов)
1. Appendicular artery is a branch of : a) ilieocolic artery
b) Right colic artery
c) Middle colic artery
d) Posterior cecal artery
2. Primary closure of incised wounds must be done within ...........
a) 2hrs
b) 4hrs
c) 6hrs
d) 12hrs
e) 16hrs
3. Which is not true of carbuncle -
a) Infective gangrene of subcutaneous tissue
b) Caused by staphylococcus
c) Diabetics are more prone
d) Caused by streptococcus
e) Pencillin and excision of necrotic tissue treatment of choice
4. Sardonic grin is associated with
a) Rabies
b) Tetanus
c) Bell's palsy
d) Hemiplegia
5. Erysipelas is caused by -
a) Staph aureus
b) Staph albus
c) Strep pyogenes
d) Hemophilus
6. Most common infection of the hand is -
a) Acute paronychia
b) Felcon
c) Web space infection
d) Palmar abscess
7. Commonest cause of nosocomial infection -
a) Pseudomonas
b) Staphylococci
c) Klebsiella
d) Enterobacteriaceae
8. Premalignant conditions of the skin include -
a) Bowen disease
b) Pagel's disease of nipple
c) Leukoplakia
d) Solar keratosis
e) All of the above
9. Prognosis of malignant melanoma depends on -
a) Grade of tumor
b) Spread of tumor
c) Depth of invasion
d) Metastasis
10. Pus in burns form in –
a) 2-3 Days
b) 3-5 days
c) 2-3 weeks
d) 4
11. Maximum tourniquet time for the upper limb is -
a) 1/2 hour
b) 1 hr
c) 1-1/2 hrs.
d) 2 hrs
e) 2-1/2 hrs
12. Commonest cause of abdominal aortic aneurysm -
a) Atherosclerosis
b) Marfan's syndrome
c) Thrombosis
d) Endocarditis
13. The sequence of symptoms in pulmonary embolism is-
a) Fever, pain, dyspnoea
b) Fever, dyspnoea
c) Dyspnoea, pain, haemoptysis
d) Dyspnoea, cough, purulent sputum
14. White leg is due to –
a) Femoral vein thrombosis and lymphatic obstruction
b) Deep femoral vein thrombosis
c) Lymphatic obstruction only
d) None of the above
15. The following is the commonest site for venous ulcer -
a) Instep of foot
b) Lower 1/3 leg and ankle
c) Lower 2/3 of leg
d) middle 1/3 of leg
16. Investigation of choice for diagnosis of deep vein thrombosis –
a) Venogram
b) Doppler
c) Isotope scan
d) Homans sign
17. Brodie -Trendlenburg test demonstrates-
a) Mid - thigh perforation
b) Deep vein thrombosis
c) Sapheno-femoral incompetence
d) Calf perforators
18. Best treatment of tension pneumothorax is -
a) Immediate letting out of air
b) Wait and watch
c) Rib resection
d) Underwater drainage
19. Most common type of diaphragmatic hernia -
a) Bochdalek's hernia
b) Morgagnl's hernia
c) Hernia throught the dome
d) Hiatus hernia
20. Normal amount of pleural fluid is approximately - a) 5ml
b) 15 ml
c)50ml
d) 100 ml
21. The commonest cause of hematemesis and malena a) Oesophageal varies
b) Chronic peptic ulcer
c) Acute peptic ulcer
d) Carcinoma of stomach
22. Uncommon cause of upper GI bleed –
a) Varices
b) Erosive gastritis
c) Peptic ulcer
d) Carcinoma stomach
23. Commonest site of peptic ulcer perforation -
a) Anterior aspect of the first part of duodenum
b) Posterior aspect of the 1st part of duodenum
c) Greater cuvature of the stomach
d) Lesser curvature of the stomach
24. Gastrin levels are raised in –
a) Zolinger Ellison syndrome
Сarcinoma stomach
Gastric ulcer
All
25. Anemia is greater in which of the following gastric resection-
a) BillRoth II
b) BillRoth I
c) Both of the above are equal
d) Neither of the above
26. Prensentmg symptom of carcinoma stomach is -
a) Bleeding
b) Obstruction
c) Perforation
d) Weight loss
27. Investigation of choice in peptic ulcer perforation is
a) USG
b) X-Ray abdomen
c) Paracentasis
d) CTscan
28. What complication commonly occurs in anterior duodenal ulcer –
a) Bleeding
b) Penetration
c) Perforation
d) Stricture formation
29. Normal portal venous pressure is -
a) 5-8 mm Hg
b) 6-12 mm Hg
c) 12-15 mm Hg
d) 45 mm Hg
30. Most common cause of surgical wound infection is -
a) Staph. aureus
b) Streptococcus
c) Pseudomonas
d) Anaerobes
31. Common bile duct stones will manifest all except -
a) Distended gall bladder
b) Jaundice
c) Itching
d) Clay coloured stools
32. Gold standard investigation for stone in bile-duct is
a) USG
b) ERCP
c) Cholangiography
d) CT scan
e) MRI
33. Most common cause of acute pancreatitis is
a) Biliary tract diseases
b) Alcoholism
c) Post traumatic
d) Idiopathic
34. Best investigation for air in peritoneal cavity is -
a) USG
b) Laparotomy
c) Laparoscopy
d) X-ray abdomen-erect view
e) CT scan
35. The commonest organism seen in peritonitis is -
a) Escherichia coli
b) Clostridium welchii
c) Staphylococci
d) Klebsiella
36. Best investigation for carcinoma colon -
a) Barium enema
b) Colonic biopsy
c) Clinical examination
d) Colonoscopy
37. Best investigation of acute mechanical intestinal obstruction is -
a) X-Ray abdomen
b) Barium enema
c) Proctosigmoidoscopy
d) Flatus tube
38. The first to appear in a cause of acute intestinal obstruction is –
a) Constipation
b) Colicky pain
c) Vomiting
d) Distension
39. Paralytic ileus is caused by -
a) Peritonitis
b) Hyperkalemia
c) Acute intestinal obstruction
d) Head injury
40. Primary feature of small intestinal obstruction -
a) Fever
b) High peristalsis with colic
c) Abdominal distension
d) Empty rectum
41. Earliest symptoms in acute appendicitis is -
a) Pain
b) Fever
c) Vomiting
d) Rise of pulse rate
42. Acute appendicitis is best diagnosed by -
a) History
b) Physical examination
c) X-ray abdomen
d) Ba meal
43. Meckel's diverticulum is -
a) Ductus venosus
b) Vitello intestinal duct
c) Left umbilical vein
d) Obliterated umbilical artery
44. Commonest type of hernia is -
a) Femoral
b) Inguinal
c) Ventral
d) Epigastric
e) Hiatus
45. Commonest type of hernia in a female is -
a) Femoral
b) Inguinal
c) Ventral
d) Hiatus
46. The superficial inguinal ring is a defect in-
a) Transversalis fascia
b) Internal oblique
c) External oblique
d) External oblique aponeurosis
47. Treatment of strangulated hernia is -
a) Observation
b) Immediate surgery
c) Manual reduction
d) Analgesics
48. Which is the 1st sign of strangulation of inguinal hernia-
a) Tense
b) Tender
c) Irreducible
d) Redness
49. What is oliguria -
a) Excretion of less than 300ml in 24 hrs
b) Excretion of less man 500ml in 24 hrs
c) Excretion of less than 300 ml. in 12 hrs
d) Excretion of less than 100 ml. in 24 hrs
50. The best site for intramuscular injection is -
a) Deltoid
b) Anterolateral part of thigh
c) Upper outer segment of buttocks
d) Upper inner segment of buttocks
№ вопроса |
Ответ |
1 |
A |
2 |
C |
3 |
D |
4 |
B |
5 |
C |
6 |
A |
7 |
D |
8 |
E |
9 |
A |
10 |
A |
11 |
C |
12 |
A |
13 |
C |
14 |
B |
15 |
B |
16 |
B |
17 |
C |
18 |
A |
19 |
D |
20 |
B |
21 |
B |
22 |
D |
23 |
A |
24 |
A |
25 |
A |
№ вопроса |
Ответ |
26 |
D |
27 |
B |
28 |
C |
29 |
B |
30 |
A |
31 |
A |
32 |
B |
33 |
A |
34 |
D |
35 |
A |
36 |
B |
37 |
A |
38 |
B |
39 |
A |
40 |
B |
41 |
A |
42 |
B |
43 |
B |
44 |
B |
45 |
B |
46 |
D |
47 |
B |
48 |
A |
49 |
A |
50 |
C |
Программированный контроль к зачетному занятию по циклу
“Абдоминальная хирургия”
В приемное отделение с улицы доставлен тяжелый больной. Хирург заподозрил перфорацию полого органа. Какой симптом не может свидетельствовать за данный диагноз: а. резкие внезапные боли в животе; б. вздутие живота; в. "доскообразный" живот; г. исчезновение печеночной тупости; д. пневмоперитонеум.
1.а. 2. б. 3. в. 4. г. 5. д.
При обследовании больного с острым панкреатитом выявлена болезненность в левом реберно-позвоночном углу. Как называется данный симптом: а. Хвостека; б. Мэрфи; в. Мейо-Робсона; г. Керте; д. Воскресенского.
1.а. 2. б. 3. в. 4. г. 5. д.
Хирург при обследовании больной заподозрил перитонит. Какой из нижеизложенных симптомов является признаком перитонита: а. рвота; б. боли в животе; в. кровавый стул; г. задержка стула и газов; д. напряжение мышц передней брюшной стенки.
1.a. 2. б. 3. в. 4. г. 5. д.
Шоковый индекс Алльговера - это: а. отношение пульса к систолическому артериальному давлению; б. отношение пульса к диастолическому артериальному давлению; в. отношение систолического артериального давления к центральному венозному давлению; г. отношение систолического артериального давления к пульсу.
1.а. 2. б. 3. в. 4. г.
У больного, обратившегося к хирургу и перенесшего аппендэктомию, через 1,5 месяца после операции появились тошнота, вздутие живота, 3-х кратная рвота, схваткообразные боли в животе. Для какого осложнения характерны указанные симптомы: а. ранняя спаечная кишечная непроходимость; б. поздняя спаечная кишечная непроходимость; в. эвентрация; г. пневмония; д. перфорация полого органа брюшной полости.
1.a. 2. б. 3. в. 4. г. 5. д.
У 19-летнего мужчины при статической нагрузке вышла и перестала вправляться ранее существовавшая у него левосторонняя паховая грыжа. Больной неоднократно пытался самостоятельно вправить грыжу, но неудачно, поэтому обратился за помощью к хирургу. Что следует делать в таком случае: а. применить груз и тепло на область грыжи; б. попытаться вновь вправить грыжу через 1 час; в. ввести спазмолитики; г. назначить строгий постельный режим; д. выполнить обзорный снимок брюшной полости; е. выполнить экстренную операцию.
1.а. 2. б. 3. в. 4. г. 5. д. 6. е.
По данным обследования больной с болями в животе выявлены незначительное вздутие живота, тошнота, периодическая рвота, гиперемия лица и положительный симптом Керте, лейкоцитоз 10,4 х109/л. Какое заболевания может быть у больной: а. язвенная болезнь желудка; б. острый холецистит; в. острый панкреатит; г. острая кишечная непроходимость; д. острый гастрит.
1.а. 2. б. 3. в. 4. г. 5. д.
Больная 19 лет обратилась с жалобами на тупые боли в эпигастральной области, тошноту, слабость, повышение температуры тела до 37,6°С. Больна 2 часа. При обследовании выявлено: пульс – 76 уд./мин, АД - 120/70 мм рт. ст., язык влажный, живот мягкий во всех отделах, симптомов раздражения брюшины нет. Лейкоциты крови – 12,0 х 109/л. Какое заболевание может так начинаться: а. острый аднексит; б. заворот тонкой кишки; в. острый аппендицит; г. парапроктит; д. почечная колика; е. острая пневмония.
1.а. 2. б. 3. в. 4. г. 5. д. 6. е.
Врачу следует помнить, что наиболее вероятным осложнением язв передней стенки 12-перстной кишки является: а. малигнизация; б. перфорация; в. кровотечение; г. дуоденостаз; д. пенетрация в головку поджелудочной железы.
1.а. 2. б. 3. в. 4. г. 5. д.
Врачу следует помнить, что наиболее вероятным осложнением язв задней стенки 12‑перстной кишки является: а. перфорация; б. малигнизация; в. дуоденостаз; г. кровотечение; д. все верно.
1.а. 2. б. 3. в. 4. г. 5. д.
Молодой мужчина поступает в приемное отделение с жалобами на сильнейшие боли в животе. Страдает язвенной болезнью несколько лет. АД - 90/60 мм рт. ст., пульс - 100 уд. в 1 мин, анурия. Пальпаторно передняя брюшная стенка резко напряжена. Диагноз, скорее всего будет, поставлен на основании следующего: а. подсчета лейкоцитов в периферической крови; б. обзорной рентгенографии брюшной полости в положении стоя; в. уровня СОЭ; г. контрастной рентгенографии желудка; д. контрастного рентгенологического исследования толстой кишки.
1.а. 2. б. 3. в. 4. г. 5. д.
Симптом Куленкампфа определяется: а. при желудочно-кишечном кровотечении; б. при прободной язве желудка и 12-перстной кишки; в. при остром панкреатите; г. при ущемленной паховой грыже; д. при закрытой травме органов грудной клетки.
1.а. 2. б. 3. в. 4. г. 5. д.
Симптом Курвуазье является патогномоничным: а. для рака головки поджелудочной железы; б. для вирусного гепатита; в. для желчнокаменной болезни; г. для цирроза печени; д. для травмы селезенки; е. для острого панкреатита; ж. для язвенной болезни; з. ни для одного из указанных заболеваний.
1.а. 2. б. 3. в. 4. г. 5. д. 6. е. 7. ж. 8. з.
При какой патологии может не определяться печеночная тупость? Выберете правильный ответ: а. перитонит; б. разрыв селезенки; в. мезентериальный тромбоз; г. желудочно-кишечное кровотечение; д. перфорация язвы желудка и 12-перстной кишки.
1.а. 2. б. 3. в. 4. г. 5. д.
У больного после приема алкоголя появилась многократная рвота, последняя с примесью алой крови. Ваш предположительный диагноз: а. кровотечение из варикозно-расширенных вен пищевода; б. синдром Маллори – Вейсса; в. острый панкреатит; г. язвенная болезнь желудка; д. болезнь Крона.
1.а. 2. б. 3. в. 4. г. 5. д.
Симптом Кохера встречается: а. при остром панкреатите; б. при остром холецистите; в. при кишечной непроходимости; г. при остром аппендиците; д. при остром аднексите.
1.а. 2. б. 3. в. 4. г. 5. д.
При каком заболевании встречается симптом Мейо-Робсона? Выберете правильный ответ: а. острый холецистит; б. перфорация язвы 12-перстпой кишки; в. острый аппендицит; г. острый панкреатит; д. кишечная непроходимость.
1.а. 2. б. 3. в. 4. г. 5. д.
У больной с ожирением IV степени внезапно появились тянущие боли внизу живота справа, с иррадиацией в правое бедро, тошнота, однократная рвота, пальпируется опухолевидное образование ниже паховой складки. О каком заболевании идет речь? Выберете правильный ответ: а. почечная колика справа; б. острый аппендицит; в. киста круглой связки матки; г. ущемленная бедренная грыжа; д. паховый лимфаденит.
1.а. 2. б. 3. в. 4. г. 5. д.
Больной 28 лет жалуется на боли в правой подвздошной области, которые начались 12 часов тому назад в эпигастрии и в последующем сместились в правую подвздошную и мезогастральную область. Общее состояние больного удовлетворительное. Температура тела - 37,7°С, пульс 96 уд. в минуту, ритмичный, удовлетворительных свойств. Язык влажный, обложен по краям. Живот мягкий. Небольшая болезненность в правой подвздошной области, симптом Щеткина-Блюмберга сомнительный. Болезненность в области треугольника Пти, здесь же - определяется ригидность мышц. Симптомы Пастернацкого, Образцова. (псоас-симптом) - положительные. Анализ крови: лейкоциты - 11,8х109/л, палочкоядерный сдвиг - 9%. Анализ мочи: удельный вес - 1016, свежие эритроциты - 3-4 в поле зрения. Выберите наиболее вероятный диагноз: а. острый аппендицит с ретроцекальным расположением червеобразного отростка; б. правосторонняя почечная колика; в. острый гастродуоденит; г. правосторонний пиелонефрит; д. опухоль правой половины ободочной кишки.
1.а. 2. б. 3. в. 4. г. 5. д.
При оценке данных обзорной рентгенографии брюшной полости хирург выявил чаши Клойбера. Они не являются характерными для: а. обтурационной кишечной непроходимости; б. странгуляционной кишечной непроходимости; в. гастрита; г. спастической кишечной непроходимости; д. паралитической кишечной непроходимости.
1.а. 2. б. 3. в. 4. г. 5. д.
При аускультации живота больной с абдоминальными болями хирург выявил звонкую усиленную перистальтику. Этот симптом характерен для ранней стадии следующего заболевания: а. желудочно-кишечного кровотечения; б. перфоративной язвы желудка; в. мезентериального тромбоза; г. механической кишечной непроходимости; д. гангренозного аппендицита.
1.а. 2. б. 3. в. 4. г. 5. д.
Врач должен знать, что синдром Маллори-Вейсса - это: а. птоз, миоз и энофтальм; б. разрыв слизистой линейной формы в кардиальном отделе желудка; в. надпеченочный блок оттока крови из печени; г. диссеминированное внутрисосудистое свертывание крови; д. гастрогенная тетания; е. форма механической желтухи.
1.а. 2. б. 3. в. 4. г. 5. д. 6. е.
Мужчина 55 лет поступает в стационар с жалобами на рвоту пищей в течение недели. Кожные покровы и слизистые сухие. Гематокрит 55%. В анамнезе отмечен постоянный болевой синдром, сменяющийся в последнее время чувством тяжести в эпигастральной области. Ранее не обследовался. При рентгеноскопии желудка выявлен значительно увеличенный желудок. Укажите патологическое состояние, чаще других встречающееся при наличии указанных симптомов: а. артериальная гипертензия; б. электролитные нарушения; в. гектическая лихорадка; г. паренхиматозная желтуха; д. гипергликемия.
1.а. 2. 6. 3. в. 4. г. 5. д.
У больного 59 лет трое суток назад появились боли в эпигастральной области, которые сместились в правую подвздошную область. Больной принимал анальгин и прикладывал к животу грелку, после чего боли в животе стихли. На следующий день боли возобновились, распространились по всему животу, появилась многократная рвота. Состояние больного тяжелое. Пульс 128 уд. в минуту. Язык сухой. Живот болезненный и напряженный во всех отделах. Симптом Щеткина-Блюмберга положительный во всех отделах живота. Лейкоцитоз - 18,6x109/л. О каком заболевании можно думать? Выберете правильный ответ: а. острый перфоративный аппендицит, разлитой перитонит; б. пилефлебит; в. перфоративная язва желудка, разлитой перитонит; г. пищевая токсикоинфекция; д. деструктивный холецистит.
1.а. 2. 6. 3. в. 4. г. 5. д.
Во время операции по поводу калькулезного холецистита при интраоперационной холангиографии выявлено расширение желчевыводящих путей, сброс контраста в 12-перстную кишку замедлен, высказано предположение о наличии конкрементов. Какой метод интраоперационного обследования является наиболее информативным для подтверждения диагноза: а. пальпация желчного протока; б. трансиллюминация; в. зондирование протоков; г. фиброхолангиоскопия; д. ревизия корзинкой Дормиа.
1.а. 2. б. 3. в. 4. г. 5. д.
Больная 60 лет при поступлении предъявляет жалобы на опоясывающие боли в эпигастральной области, многократную рвоту пищей и желчью. При пальпации болезненность в эпигастральной области с напряжением мышц передней брюшной стенки. Тахикардия (104 уд. в минуту). Лейкоциты крови ‑ 10,0х109/л, диастаза мочи - 1024 ед. На рентгенограмме - пневматизация поперечно-ободочной кишки. Ваш диагноз: а. острый панкреатит; б. обострение язвенной болезни; в. острый гастрит; г. острый холецистит; д. острая кишечная непроходимость.
1.а. 2. б. 3. в. 4. г. 5. д.
При неясной клинической картине у больного имеется напряжение и болезненность в правом подреберье и правой подвздошной области. УЗИ органов брюшной полости не оказалось информативным. Ваши действия: а. диагностическая лапаротомия; б. лапароскопия; в. компьютерная томография брюшной полости; г. динамическое наблюдение в течение суток; д. антибиотики и анальгетики, пузырь со льдом на живот.
1а. 2.б. 3. в. 4. г. 5. д.
Определите тактические действия в отношении больного, доставленного в хирургический стационар бригадой “скорой помощи” с диагнозом "острый живот". Выберете правильный ответ: а. срочная лaпаротомия; б. попытка консервативного лечения (внутривенная инфузионная терапия, спазмолитики, антибактериальная терапия, очистительная клизма); в. попытка уточнения диагноза дополнительными методами лабораторного и инструментального обследования; г. уточнение диагноза по результатам динамического наблюдения; д. срочная лапароскопия.
1.а. 2.б. 3.в. 4. г. 5. д.
Как избежать ненужной и очень опасной для больного операции при "ложном остром животе"? Выберете правильный ответ: а. провести диагностическую лапароскопию; б. назначить спазмолитики и обезболивающее средство; в. провести пробное консервативное лечение; г. обеспечить консультации специалистов другого профиля.
1.а. 2.б. 3.в. 4. г.
При проведении дифференциального диагноза у больной 26 лет между острым аппендицитом (тазовое расположение) и прервавшейся внематочной беременностью следует принимать во внимание следующие моменты: а. жалобы и данные анамнеза; б. показатели гемоглобина; в. результаты пункции заднего свода влагалища; г. наличие симптома Куленкампфа; д. результаты влагалищного и ректального исследования. Выберете правильную комбинацию ответов:
1.а, б. 2. а, б, в. 3. а, б, в, г. 4. а, б, в, д. 5. все ответы правильные.
При проведении дифференциального диагноза между острым аппендицитом и прикрытой перфорацией язвы 12-перстной кишки необходимо применить следующие методы обследования: а. гастродуоденоскопия; б. обзорная рентгеноскопия брюшной полости; в. УЗИ брюшной полости; г. лапароскопия; д. ирригоскопия. Выберете правильную комбинацию ответов:
1.а, б, в. 2. б, в, д. 3. а, б, г. 4. б, д. 5. все ответы правильные.
У больного пять дней назад появились боли в эпигастральной области, которые затем сместились в правую подвздошную область. Больной принимал тетрациклин и анальгин, обратился к врачу на пятый день заболевания в связи с сохранением болей. Состояние больного удовлетворительное. Температура 37,4°С, пульс 88 уд./мин. В правой подвздошной области пальпируется образование размерами 12x8 см плотноэластической консистенции, неподвижное, с четкими границами, умеренно болезненное. Симптом Щеткина-Блюмберга отрицательный. Лейкоциты крови 11,0х109/л. О каком заболевании можно думать: а. опухоль слепой кишки; б. терминальный илеит; в. аппендикулярный инфильтрат; г. перфоративная язва желудка или 12-перстной кишки; д. ущемленная правосторонняя паховая грыжа.
1.а. 2. б. 3. в. 4. г. 5. д.
У больной 40 лет с клиникой разлитого перитонита при лапароскопии обнаружен геморрагический выпот в количестве 1 л, кровоизлияния в области брыжейки поперечно-ободочной кишки и гепатодуоденальной связки, гиперемия брюшины; желчный пузырь – без признаков воспаления. Диастаза содержимого брюшной полости – 512 ед. Ваш диагноз: а. закрытая травма живота; б. внематочная беременность; в. геморрагический панкреонекроз; г. разрыв кисты яичника; д. разрыв селезенки.
1.а. 2.б. 3. в. 4. г. 5. д.
Дивертикул Меккеля локализуется на: а. тощей кишке; б. подвздошной кишке; в. восходящем отделе ободочной кишки; г. слепой кишке; д. сигмовидной кишке.
1.а. 2.б. 3.в. 4. г. 5. д.
При необходимости дифференциального диагноза у больной между почечной коликой и острым аппендицитом хирург поликлиники должен выполнить следующее: а. экскреторную урографию; б. анализ мочи общий и по Нечипоренко; в. хромоцистоскопию ; г. отправить в хирургический стационар; д. ввести спазмолитики.
1.а. 2. б. 3. в. 4. г. 5. д.
Лечение распространенного перитонита предусматривает: а. устранение источника перитонита; б. санацию и дренирование брюшной полости; в. коррекцию водно-электролитных нарушений; г. комбинированную антибактериальную терапию; д. дезинтоксикационную терапию. Выберете правильную комбинацию ответов:
1.а, в. 2. в, г, д. 3. в, г. 4. а, б, в, г. 5. верно все.
Противопоказаниями к экстренной операции по поводу разлитого перитонита являются: а. свежий инфаркт миокарда; б. тяжелый травматический шок при сочетанной травме; в. крайне тяжелое состояние больного; г. послеоперационный перитонит; д. нет противопоказаний. Выберете правильную комбинацию ответов:
1.а, б, в. 2. в, г. 3. б, в. 4. а, в. 5. д.
Самой частой причиной перитонита является: а. острый аппендицит; б. прободная язва; в. острый холецистит; г. странгуляция тонкой кишки; д. острый панкреатит.
1.а. 2.б. 3.в. 4. г. 5. д.
Для перитонита не характерно: а. напряжение мышц брюшной стенки; б. симптом Курвуазье; в. учащение пульса; г. задержка отхождения газов; д. рвота.
1.а. 2.б. 3.в. 4. г. 5. д.
Для перитонита не характерно: а. тахикардия; б. сухой язык; в. напряжение мышц передней брюшной стенки; г. отсутствие перистальтики кишечника; д. диарея.
1.а. 2.б. 3.в. 4. г. 5. д.
Укажите место, где определяют "френикус-симптом": а. между ножками musculus sternocleidomastoideus; б. в углу, образованном ключицей и наружным краем musculus sternocleidomastoideus; в. в области яремной вырезки грудины; г. на 3 см выше середины ключицы; д. на середине заднего края musculus sternocleidomastoideus.
1.а. 2. б. 3. в. 4. г. 5. д.
Больная 24 лет жалуется на тошноту и однократную рвоту, боли в области пупка длительностью около 5 часов. В течение последнего получаса боли переместились в правую подвздошную область, температура тела - 37,6°С. Какой диагноз наиболее вероятен у больной: а. острый панкреатит; б. острый правосторонний аднексит; в. острый аппендицит; г. перфорация язвы желудка или 12-перстной кишки; д. нарушенная внематочная беременность.
1.а. 2. б. 3. в. 4. г. 5. д.
Нормальные показатели билирубина крови: а. 0,10-0,68 мкмоль/л; б. 8,55-20,52 мкмоль/л; в. 2,50-8,33 мкмоль/л; г. 3,64-6,76 мкмоль/л; д. 7,62-12,88 мкмоль/л.
1.а. 2.б. 3.в. 4. г. 5. д.
Внутривенная холецистография информативна при: а. наличии пальпируемого желчного пузыря; б. желтухе; в. желчном перитоните; г. стихшем приступе острого холецистита; д. холангите.
1.а. 2.б. 3.в. 4. г. 5. д.
При остром и хроническом холецистите противопоказано применение: а. промедола; б. морфина гидрохлорида; в. но-шпы; г. атропина сульфата; д. спазмалгона, баралгина и спазгана.
1.а. 2.б. 3.в. 4. г. 5. д.
Ширина холедоха в норме равна: а. до 0,5 см; б. 0,6-1,0 см; в. 1,1-1,5 см; г. 1,6-2,0 см; д. свыше 2,0 см.
1.а. 2.б. 3.в. 4. г. 5. д.
Желчно-каменная болезнь может вызвать все, кроме: а. пузырно-дуоденального свища; б. механической желтухи; в. острого холецистита; г. внутрибрюшного кровотечения; д. холангита.
1.а. 2.б. 3.в. 4. г. 5. д.
Какая операция является операцией выбора при остром холецистите: а. холецистостомия; б. холецистэктомия; в. холецистолитотомия; г. холецистэктомия с холедоходуоденоанастомозом.
1.а. 2.б. 3.в. 4. г.
Для уточнения характера возникновения желтухи и ее причины не используется: а. компьютерная томография; б. внутривенная холецистохолангиография; в. чрескожная чреспеченочная холангиография; г. ЭРХПГ; д. УЗИ
1.а. 2.б. 3.в. 4. г. 5. д.
Поперечная болевая резистентность передней брюшной стенки в проекции поджелудочной железы при остром панкреатите носит название симптома: а. Мейо – Робсона; б. Керте; в. Грея – Турнера; г. Мондора; д. Воскресенского.
1.а. 2.б. 3.в. 4. г. 5. д.
При остром панкреатите в первые сутки назначается: а. стол 15; б. стол 5; в. стол 9; г. стол 10; д. голод.
1.а. 2.б. 3.в. 4. г. 5. д.
Больной 58 лет поступил с жалобами на боли в эпигастральной области, похудание на 10 кг, отвращение к жирным продуктам, плохой аппетит, метеоризм, поносы, повышение температуры тела (37,3°С). Болен около года. При осмотре: желтушность кожных покровов, при пальпации живота определяется увеличенный, безболезненный желчный пузырь. Ваш предположительный диагноз: а. стенозирующая пилородуоденальная язва; б. острый холецистит; в. рак поджелудочной железы; г. цирроз печени; д. желчно-каменная болезнь.
1.а. 2. б. 3. в. 4. г. 5. д.
Больной, перенесший 1 год назад панкреонекроз, обратился к хирургу, который заподозрил кисту поджелудочной железы. Какой метод дополнительного исследования наиболее информативен при данной патологии: а. УЗИ брюшной полости; б. рентгенография желудка и 12-перстной кишки; в. исследование амилазы крови и мочи; г. фиброэзофагогастродуоденоскопия; д. ЭРХПГ.
1.а. 2. б. 3. в. 4. г. 5. д.
Укажите основные принципы консервативной терапии острой кишечной непроходимости: а. промывание желудка; б. сифонная клизма; в. спазмолитическая терапия; г. коррекция водно-электролитных нарушений; д. экстракорпоральная детоксикация; е. паранефральная блокада. Выберете правильную комбинацию ответов:
1.а, в, е. 2. а, в, г, д. 3. а, г, д. 4. б, в, г, д, е. 5. верно все.
Не нарушается кровообращение в брыжейке кишки при: а. завороте; б. обтурации; в. узлообразовании; г. инвагинации; д. ущемлении.
1.а. 2. б. 3. в. 4. г. 5. д.
Кровянистые выделения из прямой кишки могут быть при кишечной непроходимости: а. паралитической; б. спастической; в. инвагинационной; г. спаечной; д. странгуляционной.
1.а. 2. б. 3. в. 4. г. 5. д.
Консервативное лечение острой кишечной непроходимости применяется только при: а. завороте; б. узлообразовании; в. обтурационной кишечной непроходимости; г. динамической непроходимости; д. обтурации кишки желчным камнем.
1.а. 2. б. 3. в. 4. г. 5. д.
При подозрении на острую кишечную непроходимость в первую очередь производится: а. обзорная рентгенография брюшной полости; б. исследование пассажа бария по кишечнику; в. эзофагогастродуоденоскопия; г. лапароскопия; д. биохимический анализ крови.
1.а. 2. б. 3. в. 4. г. 5. д.
Кал в виде малинового желе характерен для:
а. желудочного кровотечения; б. инвагинации; в. спастического колита; г. дивертикулита; д. свинцового отравления.
1.а. 2. б. 3. в. 4. г. 5. д.
Выявление при лапароскопии бляшек стеатонекроза соответствует: а. панкреонекрозу; б. желчному перитониту; в. гнойному перитониту; г. мезадениту; д. такие изменения не характерны для острой хирургической патологии.
1.а. 2.б. 3.в. 4. г. 5. д.
Укажите хирургическую тактику при ущемленной грыже: а. экстренная операция; б. назначить обезболивающие и спазмолитики; в. сделать теплую ванну и попытаться вправить грыжу; г. динамическое наблюдение.
1.а. 2. б. 3. в. 4. г.
Укажите тактические действия врача в отношении больного с грыжей после ее ущемления и самостоятельного вправления: а. срочная операция; б. динамическое наблюдение в условиях хирургического стационара; в. при желании больного - наблюдение врача в домашних условиях; г. отказ от дальнейшего наблюдения с рекомендацией обращения к хирургу для проведения операции в плановом порядке; д. обзорная рентгенография органов брюшной полости.
1.а. 2. б. 3. в. 4. г. 5. д.
Для чего пожилым больным с грыжами белой линии живота и пупочными грыжами перед операцией обследовать желудок? а. для определения характера органа в грыжевом мешке; б. для выявления размеров грыжевых ворот; в. для диагностики внутрибрюшной гипертензии; г. для исключения опухоли желудка или язвенной болезни; д. для исключения гастростаза.
1. а. 2. б. 3. в. 4. г. 5. д.
У больного 70 лет левосторонняя косая паховая грыжа со склонностью к ущемлению. Имеется аденома предстательной железы с нарушением мочеиспускания. Ваши рекомендации: а. ношение постоянно бандажа; б. экстренная операция при очередном ущемлении; в. оперативное лечение при быстром увеличении размеров грыжи; г. плановая операция, после осмотра уролога и коррекции нарушений мочеиспускания; д. одновременное грыжесечение и удаление аденомы.
1.а. 2. б. 3. в. 4. г. 5. д.
При осмотре больного 67 лет, перенесшего 2 месяца назад инфаркт миокарда, хирург поликлиники обнаружил ущемленную паховую грыжу. Ущемление со слов больного произошло 3 часа назад. Что следует делать: а. ввести спазмолитики и наркотики; б. положить больного в горячую ванну; в. выполнить экстренную операцию; г. наблюдать, холод на живот; д. попытаться вправить грыжу.
1.а. 2. б. 3. в. 4. г. 5. д.
Врач должен знать, что бедренные грыжи чаще встречаются: а. у мужчин; б. у стариков; в. у детей; г. у женщин; д. пол и возраст не имеют значения.
1.а. 2. б. 3. в. 4. г. 5. д.
Основным рентгенологическим признаком перфорации язвы являются: а. пневмоперитонеум; б. горизонатальные уровни жидкости; в. симптом "арок"; г. большое количество жидкости в желудке; д. симптом керкринговых складок.
1.а. 2. б. 3. в. 4. г. 5. д.
К хирургу обратился больной, в течение 23 лет страдающий язвенной болезнью 12-перстной кишки. В последний год отмечает у себя похудание, запоры, отрыжку с тухлым запахом. Около 1 месяца назад появились судороги в верхних конечностях и подергивания мышц лица. Какое осложнение развилось у больного: а. малигнизация язвы; б. гастрогенная тетания; в. кровотечение; г. пенетрация в поджелудочную железу; д. атипичная перфорация.
1.а. 2. б. 3. в. 4. г. 5. д.
Что должен назначить хирург больному с подозрением на перфорацию полого органа брюшной полости: а. фиброэзофагогастродуоденоскопию; б. сонографию; в. лапароцентез; г. контрастную рентгенографию желудка с пассажем взвеси сульфата бария по кишечнику; д. обзорную рентгеноскопию или рентгенографию брюшной полости.
1.а. 2. б. 3. в. 4. г. 5. д.
У больного установлен диагноз перфоративной язвы желудка, но он отказывается от экстренной операции по религиозным соображениям. Что следует делать хирургу: а. наблюдать больного в условиях терапевтического стационара; б. проводить комплексное консервативное лечение в хирургическом стационаре; в. ограничиться назначением массивной антибиотикотерапии; г. назначить строгий постельный режим и обезболивающее лечение на дому.
1.а. 2. б. 3. в. 4. г.
Назовите классические клинические признаки перфоративной гастродуоденальной язвы, которые удается выявить в первые часы от начала заболевания: а. предшествующий прием алкоголя или чрезмерное физическое напряжение; б. резкая, как бы "кинжальная" боль в эпигастрии; в. доскообразное напряжение мышц живота; г. "вагусный" замедленный пульс; д. рвота, не приносящая облегчения. Выберите правильную комбинацию ответов:
1.а, б, в, г. 2. все правильно. 3. а, г, д. 4. б, в, г. 5. б, в, г, д.
Консервативная терапия при прободной язве допустима лишь при: а. отсутствии у больного язвенного анамнеза; б. старческом возрасте больных; в. отсутствии условий для выполнения экстренного оперативного вмешательства; г. крайне высокой степени операционного риска; д. сочетании язвенной болезни желудка и 12-перстной кишки.
1.а. 2. б. 3. в. 4. г. 5. д.
Первый признак гастродуоденального кровотечения при язвенной болезни: а. мелена; б. легкое головокружение; в. стихание болей в животе; г. рвота типа "кофейной гущи"; д. побледнение кожных покровов.
1.а. 2. б. 3. в. 4. г. 5. д.
Самый простой метод определения объема кровопотери: а. учет количества отделяемого по желудочному зондy; б. по "индексу шока" (индексу Алльговера); в. по уровню гематокрита; г. по часовому объему диуреза; д. по уровню центрального венозного давления.
1.а. 2. б. 3. в. 4. г. 5. д.
Определите основные показатели, характеризующие кровотечение тяжелой степени: а. частота пульса больше 120 ударов в минуту; б. систолическое АД ниже 80 мм рт. ст.; в. Нв ниже 80 г/л; г. дефицит ОЦК больше 20%; д. дефицит ГО больше 30%. Выберете правильную комбинацию ответов:
1. а, б, в. 2. б, в, г. 3. все ответы правильные. 4. в, г, д. 5. Все ответы неправильные.
У практически здорового человека, злоупотребляющего алкоголем, после многократной рвоты без примеси крови началось массивное кровотечение из верхних отделов ЖКТ. Указания на язвенную болезнь в анамнезе отсутствуют. Что, скорее всего, послужило причиной кровотечения: а. хиатальная грыжа; б. рак желудка; в. язва двенадцатиперстной кишки; г. синдром Маллори-Вейсса; д. гастрит.
1.а. 2. б. 3. в. 4. г. 5. д.
Срыгивание пенистой кровью ярко-красного цвета, усиливающееся при кашле, характерно для: а. кровоточащей язвы желудка; б. опухоли кардии; в. синдрома Маллори – Вейсса; г. синдрома Рандю – Ослера; д. легочного кровотечения.
1.а. 2. б. 3. в. 4. г. 5. д.
Наиболее точно установить источник гастродуоденального кровотечения позволяет: а. рентгенологическое исследование желудка; б. фиброэзофагогастродуоденоскопия; в. назогастральный зонд; г. лапароскопия; д. повторное определение гемоглобина и гематокрита.
1.а. 2. б. 3. в. 4. г. 5. д.
Вынужденное положение больного с приведенными к животу ногами и доскообразным напряжением мышц живота характерно для: а. геморрагического панкреонекроза; б. заворота кишок; в. прободной язвы; г. почечной колики; д. мезентериального тромбоза.
1.а. 2. б. 3. в. 4. г. 5. д.
При определении группы крови в системе АВО стандартными изогемагглютинирующими сыворотками выявлена положительная реакция агглютинации со стандартными сыворотками 0(1) и А(П) групп и отрицательной с В(Ш). К какой группе принадлежит исследуемая кровь? Выберете правильный ответ: а. 0(I). б. А(II). в. В(III). г. AB(IV). д. заключение сделать нельзя.
1.а. 2. б. 3. в. 4. г. 5. д.
Что следует выполнить в первые сутки после переливания больному крови: а. наблюдение дежурного врача; б. трехкратное измерение температуры тела через 1 час; в. общий анализ мочи больного; г. общий анализ крови больного; д. анализ кала на скрытую кровь. Выберете правильную комбинацию ответов:
1.в, г, д. 2. а, б, в, г. 3. а, в, г, д. 4. а, в, г. 5. верно всё.
Биологическая проба при переливании крови предусматривает кратность и способ введения 10-15 мл крови с последующим пережатием системы: а. однократно; б. двукратно; в. трехкратно; г. четырехкратно; д. струйно. Выберете правильную комбинацию ответов:
1. а, б. 2. в, д. 3. г, д. 4. д. 5. а, в.
Перед переливанием крови необходимо: а. провести пробу на совместимость сыворотки донора и крови реципиента; б. провести пробы на совместимость сыворотки реципиента и крови донора; в. провести трехкратную биологическую пробу; г. определить группу крови реципиента; д. определить группу крови донора. Выберете правильную комбинацию ответов:
1.а, в, г, д. 2. а, в. 3. а, г, д. 4. б, в, г, д. 5. б, г, д, .
Для повреждения (разрыва) селезенки характерно положение больного: а. на левом боку с выпрямленными ногами; б. на спине с поджатыми ногами; в. беспокойное положение, симптом "ваньки-встаньки"; г. попытка занять коленно-локтевое положение; д. положение на животе.
1.а. 2. б. 3. в. 4. г. 5. д.
Больной доставлен с ножевым ранением груди в тяжелом состоянии. беспокоен, цианоз кожных покровов тоны сердца глухие, вены шеи набухшие, пульс - 130 в минуту, АД - 70/50 мм рт. ст. Причиной тяжести состояния является: а. ранение легкого ; б. геморрагический шок; в. ранение диафрагмы; г. кардиогенный шок; д. гемоперикард с тампонадой сердца.
1.а. 2. б. 3. в. 4. г. 5. д.
Пункцию плевральной полости при пневмотораксе необходимо выполнять: а. в 1-м межреберье; б. во 2‑м межреберье; в. в 4-м межреберье; г. в 5-м межреберье; д. в 7-м межреберье.
1.а. 2. б. 3. в. 4. г. 5. д.
Объясните, почему пункцию плевральной полости производят по верхнему краю ребра: а. из-за возможности повреждения межреберного coсудисто-нервного пучка; б. из-за возможности пневмоторакса; в. для предупреждения повреждения межреберных мышц; г. из‑за особенностей строения надкостницы; д. для облегчения анестезии.
1.а. 2. б. 3. в. 4. г. 5. д.
По какому из перечисленных признаков Вы определите, что кровотечение в плевральную полость продолжается: а. бледность кожных покровов; б. низкое артериальное давление; в. кровохаркание; г. притупление перкуторного звука на стороне травмы; д. положительная проба Рувилуа-Грегуара.
1.а. 2. б. 3. в. 4. г. 5. д.
Какая из перечисленных манипуляций при проникающих ранениях брюшной полости должна быть выполнена обязательно: а. первичная хирургическая обработка раны; б. лапароцентез; в. рентгеноскопия брюшной полости; г. диагностическая лапаротомия; д. гастродуоденоскопия.
1.а. 2. б. 3. в. 4. г. 5. д.
О Т В Е Т Ы
№ вопроса |
Ответ |
1 |
2 |
2 |
3 |
3 |
5 |
4 |
1 |
5 |
2 |
6 |
6 |
7 |
3 |
8 |
3 |
9 |
2 |
10 |
4 |
11 |
2 |
12 |
2 |
13 |
1 |
14 |
5 |
15 |
2 |
16 |
4 |
17 |
4 |
18 |
4 |
19 |
1 |
20 |
3 |
21 |
4 |
22 |
2 |
№ вопроса |
Ответ |
23 |
2 |
24 |
1 |
25 |
4 |
26 |
1 |
27 |
2 |
28 |
3 |
29 |
1 |
30 |
5 |
31 |
3 |
32 |
3 |
33 |
3 |
34 |
2 |
35 |
4 |
36 |
5 |
37 |
5 |
38 |
1 |
39 |
2 |
40 |
5 |
41 |
1 |
42 |
3 |
43 |
2 |
44 |
4 |
№ вопроса |
Ответ |
45 |
2 |
46 |
2 |
47 |
4 |
48 |
2 |
49 |
2 |
50 |
2 |
51 |
5 |
52 |
3 |
53 |
1 |
54 |
4 |
55 |
2 |
56 |
3 |
57 |
4 |
58 |
1 |
59 |
2 |
60 |
1 |
61 |
1 |
62 |
2 |
63 |
4 |
64 |
4 |
65 |
3 |
66 |
4 |
67 |
1 |
№ вопроса |
Ответ |
68 |
2 |
69 |
5 |
70 |
2 |
71 |
4 |
72 |
3 |
73 |
3 |
74 |
2 |
75 |
3 |
76 |
4 |
77 |
5 |
78 |
2 |
79 |
3 |
80 |
3 |
81 |
2 |
82 |
2 |
83 |
4 |
84 |
3 |
85 |
5 |
86 |
2 |
87 |
1 |
88 |
5 |
89 |
1 |
Программированный контроль к зачетному занятию по циклу
“Колопроктология”
1. Область, в которой чаще всего образуются анальные трещины (один ответ): 1) ректосигмоидный отдел толстой кишки; 2) область гребешковой (зубчатой, пограничной) линии; 3) среднеампулярный отдел прямой кишки; 4) ишеоректальная область.
2. Острая анальная трещина представляет собой (один ответ): 1) хроническую язву; 2) острую язву; 3) эрозию; 4) травматическое повреждение.
3. Наиболее вероятный путь инфицирования параректальной клетчатки при остром парапроктите (один ответ): 1) лимфогенный; 2) гематогенный; 3) через морганьевы крипты и протоки анальных желез; 4) периневральный.
4. Укажите глубокие формы острого парапроктита: а) подслизистый; б) пельвиоректальный; в) ишеоректальный; г) ретроректальный; д) подкожный. Выберете правильную комбинацию ответов:
1. б, в, г. 2. б, д. 3. б, г. 4. в, г, д. 5. верно все
5. Осложнения эпителиального копчикового хода: а) кровотечение; б) стеноз; в) перфорация; г) нагноение; д) инфицирование; е) пенетрация. Выберете правильную комбинацию ответов:
1. в, г, д. 2. а, б, д. 3. а, г. 4. г, д. 5. а, д, е.
6. Метод лечения неосложненного эпителиального копчикового хода (один ответ): 1) консервативный - мазевые повязки, анальгетики, противовоспалительные препараты; 2) оперативный - иссечение эпителиального копчикового хода; 3) оперативный - рассечение эпителиального копчикового хода.
7. Метод лечения хронической анальной трещины (один ответ): 1) консервативный - ректальные суппозитории, сидячие ванночки с антисептиками, маслянные микроклизмы, блокады дна анальной трещины, репаранты; 2) оперативный - иссечение анальной трещины с восстановлением целостности слизистой; 3) оперативный - ушивание анальной трещины.
8. Метод лечения свищевой формы хронического парапроктита (один ответ): 1) консервативный - ректальные суппозитории, сидячие ванночки с антисептиками, маслянные микроклизмы, новокаиновые блокады, репаранты; 2) оперативный - иссечение параректального свища; 3) оперативный - ушивание наружного свищевого отверстия.
9. Область расположения эпителиального копчикового хода (один ответ): 1) анальный отдел прямой кишки; 2) пельвиоректальное клетчаточное пространство; 3) область межягодичной складки; 4) ишеоректальная область.
10. Хроническая анальная трещина представляет собой (один ответ): 1) хроническую язву; 2) острую язву; 3) эрозию; 4) полип с изъязвлением.
11. Наиболее вероятный путь инфицирования параректальной клетчатки при хроническом рецидивирующем парапроктите (один ответ): 1) лимфогенный; 2) гематогенный; 3) через морганьевы крипты и протоки анальных желез; 4) периневральный.
12. Укажите поверхностные формы острого парапроктита: а) подслизистый; б) пельвиоректальный; в) ишеоректальный; г) ретроректальный; д) подкожный. Выберете правильную комбинацию ответов:
1. а, в, д. 2. б, в, д. 3. а, б, г. 4. в, г, д. 5. верно все
13. Осложнения выпадения слизистой прямой кишки: а) кровотечение; б) некроз слизистой; в) перфорация; г) ущемление стенки кишки; д) воспаление слизистой; е) пенетрация. Выберете правильную комбинацию ответов:
1. в, г, д. 2. а, б, г, д. 3. а, в, г. 4. г, д, е. 5. а , в, д, е.
14. Методы, позволяющие отличить параректальный свищ от эпителиального копчикового хода: а) проба с зондом; б) проба с введением красящего вещества; в) проба с введением рентгеноконтрастного вещества. Выберете правильную комбинацию ответов:
1. а. 2. б. 3. в. 4. а, в. 5. верно все
15. Метод лечения нагноения эпителиального копчикового хода (один ответ): 1) консервативный - мазевые повязки, анальгетики, противовоспалительные препараты; 2) оперативный - вскрытие и дренирование гнойника; 3) оперативный - удаление эпителиального копчикового хода.
16. Метод лечения острой анальной трещины (один ответ): 1) консервативный – ректальные суппозитории, сидячие ванночки с антисептиками, маслянные микроклизмы, блокады дна анальной трещины, репаранты. 2) оперативный – иссечение анальной трещины с восстановлением целостности слизистой; 3) оперативный – ушивание анальной трещины.
17. Метод лечения острого парапроктита в стадии абсцедирования (один ответ): 1) консервативный - ректальные суппозитории, сидячие ванночки с антисептиками, масляные микроклизмы, новокаиновые блокады, репаранты; 2) оперативный - вскрытие и дренирование абсцесса; 3) оперативный - резекция прямой кишки и наложение колостомы.
18. Укажите признаки, характерные для начальной стадии странгуляционной кишечной непроходимости: а) боли постоянного характера; б) схваткообразные боли; в) рвота рефлекторная, не приносящая облегчения; г) рвота фекалоидная, интоксикационная; д) положительны симптомы Валя, Склярова; е) симптомы Валя, Склярова не выявляются; ж) рентгенологически выявляются “арки”; з) рентгенологически выявляются множественные “чаши” Клойбера. Выберете правильную комбинацию ответов:
1. а, г, е, ж. 2. б, в, д, з. 3. а, в, е, з. 4. а, г, д, з. 5. а, в, д, ж.
19. Укажите признаки, характерные для обтурационной кишечной непроходимости: а) боли в животе постоянного характера; б) схваткообразные боли; в) рвота рефлекторная, не приносящая облегчения; г) рвота фекалоидная, интоксикационная на поздних стадиях; д) положительны симптомы Кивуля, Склярова; е) симптомы Валя, Склярова, Кивуля не выявляются; ж) рентгенологически выявляются “арки”; з) рентгенологически выявляются “чаши” Клойбера. Выберете правильную комбинацию ответов:
1. а, г, е, з. 2. б, г, д, з. 3. а, в, е, ж. 4. а, г, д, ж. 5. а, в, д, з.
20. Укажите основные принципы консервативной терапии острой кишечной непроходимости: а) промывание желудка; б) установка назогастрального зонда для декомпресии; в) спазмолитическая терапия; г) коррекция водно-электролитных нарушений; д) паранефральная блокада анестетиком; е) введение антикоагулянтов; ж) клизма (очистительная, сифонная); з) блокада анестетиком параректальной клетчатки. Выберете правильную комбинацию ответов:
1. а, г, е, ж, з. 2. б, г, д, е, з. 3. б, в, г, д, ж. 4. а, г, д, е, ж. 5. а, в, д, е, з.
21. Укажите признаки жизнеспособности кишки: а) розовый цвет; б) наличие перистальтики; в) отсутствие пульсации брыжеечных сосудов; г) наличие пульсации брыжеечных сосудов; д) наложение фибрина на кишке; е) отек тканей брыжейки. Выберете правильную комбинацию ответов:
1. а, д, е. 2. а, б, г. 3. б, в, е. 4. а, в, д. 5. а, в, е.
22. Инвагинация относится к непроходимости (один ответ): 1) спастической; 2) паралитической; 3) обтурационной; 4) странгуляционной; 5) смешанной.
23. Для низкой обтурационной опухолевой толстокишечной непроходимости характерно все, кроме (один ответ): 1) постепенного нарастания симптомов; 2) вздутия живота; 3) появление “чаш” Клойбера; 4) задержка стула; 5) быстрого обезвоживания.
24. При острой обтурационной толстокишечной непроходимости наблюдается все, кроме (один ответ): 1) схваткообразных болей в животе; 2) вздутия живота; 3) постепенного развития перитонита; 4) постоянных болей в животе; 5) задержки стула и газов.
25. Не нарушается кровообращение в брыжейке кишки при: 1) завороте; 2) обтурации; 3) узлообразовании; 4) инвагинации; 5) ущемлении (один ответ).
26. Толстокишечная обтурационная непроходимость чаще всего вызывается (один ответ): 1) инородными телами; 2) желчными камнями; 3) злокачественными опухолями; 4) спайками брюшной полости; 5) гельминтами.
27. При подозрении на острую кишечную непроходимость в первую очередь производится (один ответ): 1) обзорная рентгенография брюшной полости; 2) исследование пассажа бария по кишечнику; 3) эзофагогастродуоденоскопия; 4) лапароскопия; 5) биохимический анализ крови.
28. Основной причиной паралитической кишечной непроходимости является (один ответ): 1) заворот; 2) инвагинация; 3) перитонит; 4) копростаз; 5) травма живота.
29. Реактивная стадия перитонита продолжается (один ответ): 1) 4-6 часов; 2) 24 часа; 3) 48 часов; 4) 72 часа; 5) более 72 часов.
30. Для перитонита не характерно (один ответ): 1) тахикардия; 2) сухой язык; 3) напряжение мышц передней брюшной стенки; 4) отсутствие перистальтики кишечника; 5) диарея.
31. Основным симптомом перитонита является (один ответ): 1) рвота; 2) боли в животе; 3) мелена; 4) задержка стула и газов; 5) напряжение мышц передней брюшной стенки.
32. Консервативное лечение неспецифического язвенного колита включает (один ответ): 1) диету; 2) витаминотерапию; 3) лечение сульфаниламидами; 4) десенсебилизирующую терапию; 5) все перечисленное.
33. Хирургическое лечение при неспецифическом язвенном колите показано при (один ответ): 1) профузном кровотечении; 2) перфорации кишки; 3) токсической дилатации; 4) неэффективности консервативного лечения; 5) всех названных состояниях.
34. Наиболее частой причиной механической тонкокишечной непроходимости являются (один ответ): 1) инородные тела; 2) желчные камни; 3) доброкачественные опухоли; 4) спайки брюшной полости; 5) злокачественные опухоли.
35. Наиболее достоверным методом диагностики полипов ободочной кишки является (один ответ): 1) рентгенологическое исследование с пероральным введением бария; 2) ирригоскопия; 3) колоноскопия; 4) исследование кала на скрытую кровь; 5) ультразвуковое исследование.
36. При раке прямой кишки на 12 см от гребешковой линии без метастазов целесообразна (один ответ): 1) экстирпация прямой кишки по Кеню-Майлсу; 2) операция Гартмана; 3) передняя резекция прямой кишки; 4) брюшно-анальная резекция прямой кишки; 5) наложение сигмостомы; 6) наложение цекостомы.
37. При раке прямой кишки на 4 см от гребешковой линии без метастазов целесообразна (один ответ): 1) экстирпация прямой кишки по Кеню-Майлсу; 2) операция Гартмана; 3) передняя резекция прямой кишки; 4) брюшно-анальная резекция прямой кишки; 5) наложение сигмостомы; 6) наложение цекостомы.
38. При раке прямой кишки на 8 см от гребешковой линии без метастазов целесообразна (один ответ): 1) экстирпация прямой кишки по Кеню-Майлсу; 2) операция Гартмана; 3) передняя резекция прямой кишки; 4) брюшно-анальная резекция прямой кишки; 5) наложение сигмостомы; 6) наложение цекостомы.
39. К облигатным предракам толстой кишки относят (один ответ): 1) одиночный полип толстой кишки; 3) групповые полипы толстой кишки; 3) неспецифический язвенный колит; 4) болезнь Крона; 5) диффузный семейный полипоз толстой кишки.
40. Большую склонность к малигнизации имеют полипы толстой кишки (один ответ): 1) гиперпластические; 2) ворсинчатые; 3) аденоматозные; 4) множественные аденоматозные; 5) индекс малигнизации одинаков во всех случаях.
41. Основной гистологической формой рака толстой кишки является (один ответ): 1) скирр; 2) перстневидноклеточный (слизистый); 3) плоскоклеточный; 4) аденокарцинома; 5) недифференцированный.
42. Токсикоанемическая форма рака толстой кишки характерна для локализации опухоли (один ответ): 1) в правых отделах ободочной кишки; 2) в поперечно-ободочной кишке; 3) в нисходящей ободочной кишке; 4) в сигмовидной кишке; 5) в прямой кишке.
43. К радикальным операциям при раке ободочной кишки относятся: а) правосторонняя гемиколэктомия; б) левосторонняя гемиколэктомия; в) трансверзостомия; г) резекция поперечно-ободочной кишки; д) трансверзосигмостомия; е) сигмостомия; ж) резекция сигмовидной кишки; з) илеотрансверзостомия. Выберете правильную комбинацию ответов:
1. а, г, е, з. 2. а, б, г, ж. 3. а, в, д, ж. 4. а, б, е, з. 5. б, в, д, ж.
44. Геморрой – это заболевание, возникновение которого объясняется (один ответ): 1) варикозным расширение вен прямой кишки; 2) лимфостазом; 3) гиперплазией кавернозных вен прямой кишки; 4) тромбозом геморроидального сплетения.
45. Внутренние геморроидальные узлы расположены (один ответ): 1) ниже гребешковой (пограничной) линии на уровне морганьевых крипт; 2) на уровне гребешковой линии; 3) выше гребешковой линии на уровне морганьевых складок; 4) в подслизистолм слое ампулярного отдела прямой кишки на уровне предстательной железы (у мужчин) и матки (у женщин).
46. Осложнения геморроя: а) кишечная непроходимость; б) тромбоз геморроидальных узлов; в) кровотечение; г) малигнизация; д) воспаление геморроидальных узлов; е) перфорация в просвет кишки; ж) перфорация в брюшную полость. Выберете правильную комбинацию ответов:
1. а, б, ж. 2. а, б, г. 3. а, д, ж. 4. а, б, е. 5. б, в, д.
47. Типичная локализация геморроидальных узлов в анальном канале (один ответ): 1) на 3, 6, 9 часах условного циферблата; 2) на 4, 8, 12 часах условного циферблата; 3) на 2, 5, 9 часах условного циферблата; 4) на 3, 7, 11 часах условного циферблата; 5) на 1, 4, 9 часах условного циферблата.
48. Характер выделяющейся крови при геморрое канале (один ответ): 1) алая кровь, характерная для артериального кровотечения; 2) темная кровь, характерная для венозного кровотечения; 3) смешанная кровь, характерная для капиллярно-паренхиматозного кровотечения.
49. Варианты геморроидэктомии предусматривают: а) оставление внутренних геморроидальных узлов; б) иссечение морганьевых крипт; в) перевязку сосудистых ножек геморроидальных узлов; г) предварительную перевязку протоков анальных желез; д) иссечение всех геморроидальных узлов; е) лигирование нижне-брыжеечной артерии; ж) удаление регионарного лимфоузла. Выберете правильную комбинацию ответов:
а., в. 2. б, г. 3. д, ж. 4. в, д. 5. а , е. 6. г, д.
50. Вторичный геморрой – это (один ответ): 1) геморрой у беременных; 2) геморрой, возникший на фоне привычных запоров; 3) геморрой у лиц, занимающихся тяжелым физическим трудом; 4) геморрой при портальной гипертензии различного происхождения.
О Т В Е Т Ы
№ вопроса |
Ответ |
1 |
2 |
2 |
4 |
3 |
3 |
4 |
3 |
5 |
4 |
6 |
2 |
7 |
2 |
8 |
2 |
9 |
3 |
10 |
1 |
11 |
3 |
12 |
1 |
13 |
2 |
14 |
5 |
15 |
2 |
16 |
1 |
17 |
2 |
18 |
5 |
19 |
2 |
20 |
3 |
21 |
2 |
22 |
5 |
23 |
5 |
24 |
4 |
25 |
2 |
№ вопроса |
Ответ |
26 |
3 |
27 |
1 |
28 |
3 |
29 |
2 |
30 |
5 |
31 |
4 |
32 |
5 |
33 |
5 |
34 |
4 |
35 |
3 |
36 |
3 |
37 |
1 |
38 |
4 |
39 |
5 |
40 |
2 |
41 |
4 |
42 |
1 |
43 |
2 |
44 |
3 |
45 |
3 |
46 |
5 |
47 |
4 |
48 |
1 |
49 |
4 |
50 |
4 |
Программированный контроль к зачетному занятию по циклу
“Хирургическая инфекция”
1. Выберите правильное определение сепсиса. Сепсис - это сочетание: а. периодической или упорной бактериемии с несанированным очагом инфекции; б. упорной бактериемии с синдромом полиорганной дисфункции; в. системного ответа на воспаление с наличием очага инфекции; г. синдрома системной воспалительной реакции с гнойно-резорбтивной лихорадкой; д. периодической или упорной бактериемии, очага инфекции и синдрома полиорганной дисфункции.
а. 2. б. 3. в. 4. г. 5. д.
2. Септический уровень бактериальной контаминации ран составляет (микробных тел на 1 г ткани): а. 105-106 микр/г ткани; б. 106-107 микр/г ткани; в. 107-108 микр/г ткани; г. 108-109 микр/г ткани; д. выше 109 микр/г ткани.
1. а. 2. б. 3. в. 4. г. 5. д.
3. Основные признаки бактериально-токсического шока следующие: а. высокая температура тела; б. брадикардия; в. ознобы; г. падение артериального давления; д. олигурия. Выберете правильную комбинацию ответов:
а, в, г, д. 2. а, б, в, д. 3. б, в, г, д. 4. а, в, г. 5. верно все.
4. С чего следует начинать лечение первичного очага при сепсисе? а. хирургическая обработка раны; б. применение протеолитических ферментов: в. гипербарическая оксигенация; г. тампонирование раны; д. ушивание раны.
1. а. 2. б. 3. в. 4. г. 5. д.
5. Первичная хирургическая обработка огнестрельной раны представляет собой: а) промывание раны антисептиками; б) наложение асептической повязки; в) обкалывание раны антибиотиками; г) оперативное вмешательство с иссечением нежизнеспособных тканей и рассечением раневого канала; д) наложение транспортной шины.
1. а. 2. б. 3. в. 4. г. 5. д.
6. При первичной хирургической обработке огнестрельной раны преследуется основная цель: а) остановить кровотечение; б) произвести остеосинтез в случае огнестрельного перелома конечности; в) предупредить развитие раневой инфекции; г) добиться заживления раны первичным натяжением; д) сшивание сосудов, нервов и сухожилий при их повреждениях.
1. а. 2. б. 3. в. 4. г. 5. д.
7. Вторичное заживление раны наблюдается при заживлении через: а. нагноение; б. струп; в. грануляции; г. все указанное; д. ничего из указанного.
а. 2. б. 3. в. 4. г. 5. д.
8. К амбулаторному хирургу пришел больной с загрязненной укушенной раной правого предплечья. В анамнезе - нападение бездомной собаки. Что из ниже перечисленного не показано данному пациенту: а. первичная хирургическая обработка раны; б. ушивание раны; в. введение антибиотиков; г. профилактика столбняка.
а. 2. б. 3. в. 4. г.
9. Необходимым условием для первичного заживления раны является: а. наличие в ране очагов некроза и гематом; б. соприкосновение краев раны; в. сохранение жизнеспособности краев раны; г. небольшая зона повреждения; д. бактериальная обсемененность тканей раны выше критического уровня. Выберете правильную комбинацию ответов:
1. а, в. 2. б, д. 3. б, в. 4. г, д. 5, верно все.
10. Для местного лечения гнойных ран в фазе воспаления применяются: а. жирорастворимые мази; б. протеолитические ферменты; в. водорастворимые мази; г. промывание антисептиками; д. иммунизация. Выберете правильную комбинацию ответов:
1. а, б. 2. а, б, в. 3. б, в, г. 4. а, д. 5. а, г, д.
11. Какие манипуляции входят в первичную хирургическую обработку раны? а. иссечение краев раны; б. остановка кровотечения; в. удаление из раны инородных тел; г. промывание раны антибиотиками; д. иссечение дна раны; е. иссечение стенок раны. Выберете правильную комбинацию ответов:
а, в, г, д. 2. а, б, в, д, е. 3. б, в, г, д. 4. а, б, г, д. 5. верно все.
12. Различают следующие виды заживления ран: а. путем вторичного рассасывания гематомы; б. путем биологического слипания тканей; в. вторичным натяжением; г. первичным натяжением; д. под повязкой; е. под гипсовой лонгетой; ж. под струпом. Выберете правильную комбинацию ответов:
а, б, д. 2. д, е, ж. 3. в, г, ж. 4. в, г, д. 5. верно все.
13. У больного с анаэробной инфекцией состояние крайне тяжелое, нижняя конечность резко отечна, чувствительность и движения в пальцах стопы отсутствуют, нарастает интоксикация. В каком из перечисленных мероприятий больной нуждается по жизненным показаниям: а. дезинтоксикационная терапия; б. гипербарическая оксигенация; в. лампасные разрезы; г. лампасные разрезы с иссечением мертвых тканей; д. ампутация конечности.
а. 2. б. 3. в. 4. г. 5. д.
14. Малая подкожная (скрытая) вена обычно располагается: а) в подкожной клетчатке на всем протяжении задней поверхности голени; б) в подкожножировой клетчатке в нижней половине голени и между листками глубокой фасции в верхней; в) между листками глубокой фасции на всем протяжении; г) субфасциапьно; д) между листками глубокой фасции в нижней половине и субфасциапьно в верхней.
а. 2. б. 3. в. 4. г. 5. д.
15. Наиболее опасным осложнением тромбоза глубоких вен является: а) трофическая язва голени; б) эмболия легочной артерии; в) тромбофлебит поверхностных вен; г) облитерация глубоких вен; д) слоновость.
а. 2. б. 3. в. 4. г. 5. д.
16. Хирург решил выполнить пробу Пратта с двумя бинтами. Для чего она выполняется: а. для выявления непроходимости глубоких вен нижних конечностей; б. для определения недостаточности артериального кровообращения нижних конечностей; в. для исследования недостаточности перфорантных вен; г. для диагностики окклюзии подколенной артерии.
а. 2.,б. 3. в. 4. г.
17. Компрессионное бинтование нижних конечностей после флебэктомии начинают с: а. верхней трети бедра; б. нижней трети бедра; в. подколенной области; г. стопы.
а. 2. б. 3. в. 4. г.
18. Каким должен быть оптимальный верхний уровень компрессионного бинтования нижних конечностей после флебэктомии: а. средняя треть голени; б. верхняя треть голени; в. нижняя треть бедра; г. верхняя треть бедра.
а. 2. б. 3. в. 4. г. 5. д.
19. В амбулаторном лечении флеботромбоза вен нижних конечностей используют все, кроме: а. возвышенного положения конечности в постели; б. антикоагулянтной терапии; в. дезагрегантов; г. компрессионной тера пии; д. спазмолитиков.
а. 2. б. 3. в. 4. г. 5. д.
20. К симптомам варикозной болезни не относятся: а. отеки дистальных отделов конечностей к вечеру; б. перемежающаяся хромота; в. трофические расстройства кожи; г. судороги по ночам; д. видимое расширение подкожных вен.
1.а. 2. б. 3. в. 4. г. 5. д.
21. При оценке проходимости глубоких вен нижних конечностей можно применить функциональную пробу: а. Гаккенбруха; б. Пратта-2; в. Гоманса; г. Дельбе-Пертеса; д. Шварца.
1. а. 2. б. 3. в. 4. г. 5. д.
22. При отсутствии инструментальных методов исследования хирург для выявления несостоятельности клапанов поверхностных вен может использовать пробу: а. трехжгутовую (Шейниса); б. маршевую (Дельбе-Пертеса); в. Троянова-Тренделенбурга; г. Пратта-2.
а. 2. б. 3. в. 4. г. 5. д.
23. При осмотре в поликлинике хирург выявил у больного ряд симптомов заболевания. Что при этом характерно для острого флеботромбоза: а. резкий отек и гиперемия нижней конечности; б. аритмия; в. отсутствие пульса на артериях стопы; г. перемежающаяся хромота; д. неустойчивый стул.
1. а. 2. б. 3. в. 4. г. 5. д.
24. Что не следует рекомендовать хирургу при остром тромбофлебите поверхностных вен голени: а. постельный режим; б. лекарства противовоспалительного действия; в. местное применение антикоагулянтной мази; г. активную ходьбу; д. возвышенное положение конечности.
1. а. 2. б. 3. в. 4. г. 5. д.
25. Больная 60 лет поступила с жалобами на кровотечение из венозного узла правой голени. Страдает варикозным расширением вен правой нижней конечности в течение 20 лет. Объективно: в нижней трети правой голени на фоне гиперпигментации и индурации кожи имеется трофическая язва, размерами 3x4 см. В зоне язвы имеется венозный узел, из которого поступает кровь. На голени и бедре выраженные варикозные изменения по ходу ствола большой подкожной вены. Для остановки кровотечения из венозного узла следует предпринять: а. прижать бедренную артерию; б. придать конечности возвышенное положение; в. наложить давящую повязку; г. ввести внутривенно дицинон; д. внутривенно перелить стрептокиназу. Выберете правильную комбинацию ответов:
1. а, б, в. 2. б, в, д. 3, а, б, г. 4. б, в, г. 5. все верно.
26. Для варикозной болезни нижних конечностей характерны следующие клинические признаки: а. боли в икроножных мышцах, появляющиеся при ходьбе; б. постоянный отек всей конечности; в. трофические расстройства кожи у медиальной лодыжки; г. отек стопы и тупые боли в ноге, появляющиеся к концу рабочего дня; д. судороги икроножных мышц голени в покое. Выберете правильную комбинацию ответов:
б, в, д. 2. а, б, д. 3. в, г, д. 4. а, в, д. 5. все ответы правильные.
27. Укажите, с какой стороны от бедренной артерии располагается бедренная вена у основания бедренного треугольника: а. медиально; б. латерально; в. сзади; г. спереди; д. перпендикулярно.
1. а. 2. б. 3. в. 4. г. 5. д.
28. В дифференциальном диагнозе между острым венозным и артериальным тромбозом учитывается все, кроме: а. характера отека; б. окраски кожи; в. состояния поверхностных вен; г. пульсации артерий; д. пола больного.
1. а. 2. б. 3. в. 4. г. 5. д.
29. Какое из перечисленных заболеваний может привести к возникновению мезентериального тромбоза? а. мерцательная аритмия; б. варикоз вен нижних конечностей; в. тромбофлебит; г. артрит; д. острый панкреатит.
1. а. 2. б. 3. в. 4. г. 5. д.
30. Хирург осматривает больного с признаками острой артериальной ишемии нижней конечности. Что нельзя отнести к характерным симптомам данной патологии: а. бледность кожи; б. похолодание кожи; в. отсутствие или ослабление пульса ниже уровня окклюзии; г. периодические судороги в голени; д. постоянные боли в конечности.
а. 2. 6. 3. е. 4. г. 5. д.
31. У больной 54 лет, страдающей ревматическим митральным пороком сердца, подозревается эмболия левой подколенной артерии. При исследовании левой нижней конечности можно выявить следующие признаки вышеуказанной локализации эмболической окклюзии: а. отсутствие пульсации бедренной артерии; б. отсутствие пульсации подколенной артерии; в. отсутствие пульсации артерий на стопе; г. усиление пульсации подколенной артерии по сравнению с контрлатеральной; д. ослабление пульсации подколенной артерии. Выберете правильную комбинацию ответов:
б, в. 2. а, д. 3. в, г. 4. а, б, в. 5. все неверно.
32. Наиболее частой причиной эмболии артерий большого круга кровообращения является: а. ишемическая болезнь сердца; б. атеросклероз дуги аорты; в. аневризма аорты; г. артерио-венозные свищи; д. тромбоз вен системы нижней полой вены.
1. а. 2. б. 3. в. 4. г. 5. д.
33. Больной 26 лет последние 5 лет отмечает боли в левой стопе и голени при ходьбе, может пройти без остановки лишь 50‑60 м. Объективно: кожные покровы левой стопы и голени до средней трети бледные, прохладные наощупь; гипостезия на стопе. Пульсация бедренной и подколенной артерии - четкая, на артериях стопы не определяется.Отмечается ослабление пульсации артерий на правой стопе. Для уточнения диагноза и определения тактики лечения в обязательном порядке следует произвести следующие исследования: а. допплерографию сосудов нижних конечностей; б. аортоскопию; в. ультразвуковое ангиосканирование сосудов нижних конечностей; г. радиоизотопную аортографию; д. артериографию нижних конечностей. Выберите правильную комбинацию ответов:
1. а, б, в. 2. б, в, г. 3. б, г, д. 4. а, в, д. 5. а, б, д.
34. Укажите основные клинические симптомы массивной тромбоэмболии лёгочных артерий: а. боли за грудиной; б. коллапс; в. цианоз лица и верхней половины туловища; г. набухание и пульсация ярёмных вен; д. гидроторакс. Выберете правильную комбинацию ответов:
1. а, б, в. 2. а, в, г, 3. а, б, д. 4. все ответы правильные.
35. Для чего используют при операциях на сосудах катетер Фогарти. а. тромбэктомии; б. закрытия баталлова протока; в. длительной внутривенной инфузии лекарственных средств; г. внутривенной урографии; д. пункции подключичной вены.
1. а. 2. б. 3. в. 4. г. 5. д.
36. Объясните, чем опасно острое нарушение кровообращения в чревном стволе: а. острой почечной недостаточностью; б. некрозом органов верхнего этажа брюшной полости; в. острой кишечной непроходимостью; г. острой ишемией органов малого таза; д. острой надпочечниковой недостаточностью.
а. 2. б. 3. в. 4. г. 5. д.
37. Какое положение нужно придать конечности, чтобы определить пульсацию подколенной артерии: а. ногу разогнуть в коленном суставе; б. ногу согнуть в коленном суставе; в. ногу ротировать кнаружи; г. ногу ротировать кнутри; д. ногу поднять под углом 30 .
а. 2. б. 3. в. 4. г. 5. д.
О Т В Е Т Ы
на
Программированный контроль к зачетному занятию по циклу
“Хирургическая инфекция”
№ вопроса |
Ответ |
1 |
3 |
2 |
1 |
3 |
1 |
4 |
1 |
5 |
4 |
6 |
3 |
7 |
3 |
8 |
2 |
9 |
3 |
10 |
3 |
11 |
5 |
12 |
3 |
13 |
5 |
14 |
2 |
15 |
2 |
16 |
3 |
17 |
4 |
18 |
4 |
19 |
5 |
№ вопроса |
Ответ |
20 |
2 |
21 |
4 |
22 |
3 |
23 |
1 |
24 |
4 |
25 |
4 |
26 |
3 |
27 |
1 |
28 |
5 |
29 |
1 |
30 |
4 |
31 |
3 |
32 |
1 |
33 |
4 |
34 |
2 |
35 |
1 |
36 |
2 |
37 |
2 |
Программированный контроль к зачетному занятию по циклу
“Поликлиническая хирургия”
В поликлинику явилась больная с послеродовым правосторонним маститом в стадии серозного воспаления. Какое лечение нельзя назначать хирургу:
массаж груди;
сцеживание молока;
смазывание сосков дезинфицирующими растворами;
возвышенное положение груди;
УФ-терапия.
Где наиболее часто следует искать первичный очаг воспаления при остром гематогенном остеомиелите:
в диафизе кости;
в эпифизе кости;
в метафизе кости;
не имеет значения.
Какие признаки считаются характерными для начального периода острого гематогенного остеомиелита:
лейкоцитоз;
боль в конечности;
нарушение функции конечности;
гипертермия;
анемия.
Эризипелоид от панариция отличается:
отсутствием отека;
отсутствием локальной болезненности и зудом;
лимфангитом;
гиперемией пальца.
Какое типичное осложнение можно наблюдать при фурункуле верхней губы:
тромбоз кавернозного синуса;
тромбоз сонной артерии;
периостит верхней челюсти;
рожистое воспаление лица;
некроз кожи.
При надпоневротической флегмоне ладони отмечается:
сильный отек тыла кисти;
незначительное нарушение общего самочувствия;
флюктуация;
незначительное нарушение функции кисти;
гипертермия.
При постановке диагноза "карбункул" с локализацией на конечности хирург должен:
оперировать больного;
назначить антибиотики;
назначить физиотерапевтическое лечение;
наблюдать в динамике.
Лечение фурункула в начальной (первой) фазе заболевания предусматривает все, кроме:
операции;
физиотерапии;
спиртовых компрессов;
антибиотиков;
методов иммунотерапии.
Воспаление каких сухожильных влагалищ сгибателей пальцев может ;осложниться флегмоной предплечья:
I и V;
I и III;
Ill и IV;
II иIV.
Что нельзя использовать в лечении серозной фазы мастита:
рассечение;
антибиотикотерапию;
физиотерапию;
профилактику лактостаза;
ретромаммарную новокаиновую блокаду с антибиотиками.
Инфильтрат от абсцесса мягких тканей отличается:
болью;
гиперемией;
отсутствием флуктуации;
гипертермией;
лейкоцитозом.
При подапоневротической флегмоне ладони отмечается:
сильный отек тыла кисти;
незначительное нарушение общего самочувствия;
флюктуация;
незначительное нарушение функции кисти;
гипертермия.
Гидраденит чаще всего локализуется в области:
подмышечной впадины;
паховой области;
локтевой ямки;
подколенной области;
не имеет значения.
Возбудителем эризипелоида является:
стафилококк;
стрептококк;
палочка свиной рожи;
клебсиелла;
анаэробы.
Возбудителем фурункула чаще всего является:
стафилококк;
стрептококк;
палочка свиной рожи;
клебсиелла;
анаэробы.
Возбудителем гидраденита чаще всего является:
стафилококк;
стрептококк;
палочка свиной рожи;
клебсиелла;
анаэробы.
Оперативное лечение абсцедирующего фурункула предусматривает:
линейный разрез;
дугообразный разрез;
иссечение гнойника;
крестообразный разрез;
все верно.
Оперативное лечение карбункула предусматривает:
линейный разрез;
дугообразный разрез;
иссечение гнойника;
крестообразный разрез;
все верно.
При вскрытии подкожного панариция используют анестезию по методу:
Оберста-Лукашевича;
Брауна;
инфильтрационную местную анестезию;
блокаду плечевого сплетения;
все верно.
20. К хирургу обратился пациент с жалобами на резкую боль во 2 пальце правой кисти, повышение температуры тела до 37,9°С. При осмотре палец резко увеличен в объеме, неправильной формы, кожа цианотична, движения в суставах пальца отсутствуют. Давность заболевания - 5 суток. Наиболее вероятный диагноз:
костный панариций;
сухожильный панариций,
пандактилит;
подкожный панариций.
К хирургу обратился пациент с жалобами на интенсивные, "сверлящего" характера боли на протяжении дистальной фаланги 3 пальца правой руки, повышение температуры тела до 39°С, головную боль, общее недомогание. При осмотре наблюдается колбообразное утолщение ногтевой фаланги, напряженность мягких тканей пальца с гиперемией кожных покровов. Давление по оси пальца резко болезненно. Давность заболевания - 3 суток. Наиболее вероятный диагноз:
костный панариций;
сухожильный панариций;
пандактилит;
подкожный панариций.
Какой из симптомов флегмоны не характерен при локализации процесса на ладонной поверхности кисти:
боль;
флюктуация;
повышение температуры тела;
локальная отечность;
гиперемия кожи.
К хирургу обратился больной с температурой 38°С, жалобами на озноб, выраженные головные боли. При осмотре в области затылка определяется плотный болезненный синюшно-багровый инфильтрат, на коже имеется несколько свищевых отверстий, через которые выделяется гной. Поставьте диагноз:
абсцесс;
карбункул;
флегмона;
фурункул.
Для рожистого воспаления не характерно:
образование на коже резко ограниченных эритематозных очагов;
образование на коже воспалительных эритематозных очагов с нечеткими границами;
рецидивирующий характер;
лимфангит, лимфаденит.
На прием к хирургу пришел пациент с инфицированной раной правого предплечья, от которой в виде жгута проксимально тянется полоска инфильтрации и гиперемии. Пальпация данной зоны болезненна. О развитии какого осложнения следует думать:
абсцесс;
тендовагинит;
стволовой лимфангит;
миозит.
На прием к хирургу пришла больная с ретромаммарным абсцессом. Каким разрезом следует производить вскрытие абсцесса:
по складке под молочной железой;
радиальными в верхних квадрантах железы;
радиальными разрезами в нижних квадрантах железы;
околососковым.
27. К формам рожистого воспаления относятся: а. эритематозная; б. буллезная; в. катаральная; г. флегмонозная; д. некротическая; е. гангренозная. Выберете правильную комбинацию ответов:
а, б, д, е.
а, б, г, д.
б, в, г, е.
в, г, д, е.
верно все.
28. Опасность перехода гнойного процесса на предплечье возникает при панарициях: а. I пальца; б. II пальца; в. Ill пальца; г. IV пальца; д. V пальца. Выберете правильную комбинацию ответов:
а, в.
б, в, г.
а, д.
б, д.
верно все.
29. Виды панариция: а. кожный; б. гематогенный; в. подкожный; г. сухожильный; д. костный; е. межмышечный; ж. эризепилоид; Выберете правильную комбинацию ответов:
а, в, г, д.
а, б, г, д.
д, е, ж.
б, d, г, ж.
верно все.
Каким микроорганизмом вызывается рожа:
стафилококк;
стрептококк;
синегнойная палочка;
вульгарный протей;
пневмококк.
Какие структурные элементы поражаются при фурункуле? а. волосяной фолликул; б. сальная железа; в. мышцы; г. потовая железа; д. подкожная клетчатка. Выберете правильную комбинацию ответов:
а, б, г.
а, б, д.
а, г, д.
а, в, д.
верно все.
Что надо делать при флегмоне мягких тканей в стадии гнойного расплавления?
холод (гипотермия);
широкий разрез и дренирование;
пункцию с последующим бактериологическим исследованием;
горячий компресс;
новокаиновое обкалывание с антибиотиками
Лечение острого интрамаммарного мастита в стадии инфильтрации предусматривает: а. выполнение операции; б. предупреждение лактостаза; в. подвешивание молочной железы косыночной повязкой; г. антибактериальную терапию; д. выполнение ретромаммарной новокаиновой блокады с антибиотиками и протеолитическими ферментами. Выберете правильную комбинацию ответов:
а.
а, б, в.
в, г, д.
б, в, г, д.
верно все.
Какой разрез будет оптимальным при осуществлении дренирующей операции по поводу острого гнойного интрамаммарного мастита?
параареолярный разрез;
полуовальный разрез;
радиарный разрез;
разрез по нижней переходной складке;
разрез не нужен, можно ограничиться пункцией гнойника.
Клиническую картину гидраденита характеризуют следующие признаки:
а. образование плотного болезненного узла;
б. наличие фолликулярной пустулы;
в. выделение сливкообразного гноя;
г. наличие некротического стержня;
д. возникновение плотного инфильтрата.
Выберете правильную комбинацию ответов:
а, б, д.
б, в, г.
б, в, д.
в, г, д.
а, в, д.
Как подразделяют остеомиелит в зависимости от пути инфицирования?
а. гематогенный;
б. неспецифический;
в. негематогенный: травматический, огнестрельный, контактный;
г. специфический;
д. гематогенный: острый, первичный хронический, вторичный хронический;
е. негематогенный: острый, хронический.
Выберете правильную комбинацию ответов:
б, г.
д, е.
а, в.
в, д.
верно все.
Для хронического гематогенного остеомиелита характерно:
а. поражение кости на значительном протяжении;
б. опухолеподобный инфильтрат мягких тканей;
в. замещение костного мозга соединительной тканью;
г. поражение метаэпифиза и диафиза;
д. постоянно наблюдается атрофия мышц;
е. гнойная интоксикация;
ж. обязательное поражение ближайших суставов.
Выберете правильную комбинацию ответов:
а, д, ж.
б, в.
б, в, г, е.
а, г, е.
а, б, д, ж.
Когда появляются рентгенологические признаки острого гематогенного остеомиелита?
через 3 дня;
через 3 мес.;
через 10-15 дней;
через 20 - 30 дней;
через 30 - 40 дней.
Какие хирургические приемы наиболее целесообразны при лечении больного с острым гематогенным остеомиелитом?
а. только вскрытие флегмоны;
б. вскрытие флегмоны и рассечение надкостницы;
в. трепанация на протяжении пораженной кости;
г. резекция пораженной кости;
д.. декомпрессивное дренирование костного канала.
Выберете правильную комбинацию ответов:
а, в, г.
б, г, д.
б, в, д.
а, в, д.
в, г, д.
Каков наиболее рациональный объем хирургических манипуляций при лечении хронического остеомиелита?
а. иссечение свищей;
б. остеоперфорация;
в. секвестрэктомия;
г. вскрытие флегмоны;
д. пластика костной полости;
е. длительное активное промывное дренирование.
Выберете правильную комбинацию ответов:
б, в, г, д.
а, б, д, е.
а, в, д, е.
в, г, д, е.
а, в, г, е.
Кардинальными симптомами хронического остеомиелита являются:
а. высокая температура;
б. рецидивирующий характер заболевания;
в. пульсирующая боль;
г. наличие секвестральной коробки, секвестра;
д. появление свищей.
Выберете правильную комбинацию ответов:
а, б, в.
б, в, д.
а, в, д.
б, г, д.
верно все.
С чего следует начать лечение острого гнойного артрита в коленном суставе? (один ответ)
наложение мазевой повязки;
физиотерапия;
иммобилизация конечности;
эвакуация гнойного экссудата путем пункции или вскрытия;
резекция пораженного гнойным процессом участка кости.
О Т В Е Т Ы
на
Программированный контроль к зачетному занятию по циклу
“Поликлиническая хирургия”
№ вопроса |
Ответ |
1 |
1 |
2 |
3 |
3 |
1, 2, 3, 4 |
4 |
2 |
5 |
1 |
6 |
2, 4, 5 |
7 |
1 (1, 2, 3) |
8 |
1 |
9 |
1 |
10 |
1 |
11 |
3 |
12 |
1, 5 |
13 |
1(1, 2) |
14 |
3 |
15 |
1 |
16 |
1 |
17 |
1 |
18 |
4 |
19 |
1 |
20 |
3 |
21 |
1 |
№ вопроса |
Ответ |
22 |
2 |
23 |
2 |
24 |
2 |
25 |
3 |
26 |
1 |
27 |
2 |
28 |
3 |
29 |
1 |
30 |
2 |
31 |
2 |
32 |
2 |
33 |
4 |
34 |
3 |
35 |
5 |
36 |
3 (3,4) |
37 |
4 |
38 |
3 |
39 |
3 |
40 |
3 |
41 |
4 |
42 |
4 |
Итоговый тестовый контроль на кафедре госпитальной хирургии Вариант 1
1.Что из указанных средств и методов не следует применять при лечении гнойных ран в фазе гидратации? а) мазевые повязки; б) покой; в) антибиотикотерапию; г) промывание перекисью водорода; д)теплые марганцевые ванны.
2. Для фазы дегидратации в течении раневого процесса характерно: а)отек краев раны; б)гиперемия краев раны; в)дно раны покрыто фибрином; г)появление грануляций; д)лейкоцитарная инфильтрация тканей.
3. Лечение гнойных ран конечностей в фазе дегидратации: что не следует применять из указанного? а) витаминотерапию; б) сближение краев раны; в) повязки с гипертоническими растворами; г) переливание крови; д) повязки с мазью Вишневского.
4. Каковы оптимальные сроки для проведения первичной хирургической обработки раны? а) до 6 час; б) до 8 час; в) до 12 час; г) до 18 час; д) до 24 час.
5. Больному с AB(IV) группой крови по жизненным показаниям необходимо перелить кровь. Определить резус-фактор нет ни времени, ни возможности. Какой группы и "резуса" кровь предпочтительнее при этом перелить больному?
а) AB(IV) резус-положительную; б) AB(IV) резус-отрицательную; в) В(III) резус-положительную; г) А(II) резус-отрицательную; д) О(I) резус-положительную.
6. Какой из ниже перечисленных возбудителей сепсиса наиболее часто дает метастазирование? а) стрептококк; б) стафилококк; в) пневмококк; г) гонококк; д) кишечная палочка.
7. Для острого аппендицита не характерен симптом: а) Ровзинга; б) Воскресенского; в) Мерфи; г) Образцова; д) Бартомье-Михельсона.
8. К перитонеальным симптомам при остром аппендиците относят симптомы: а) Воскресенского (симптом «рубашки»); б) Щеткина-Блюмберга; в) Раздольского; г) все названные симптомы; д) ни один из них.
9. Острый аппендицит следует дифференцировать со всеми перечисленными заболеваниями, кроме: а) гломерулонефрита; б) острого панкреатита; в) острого аднексита; г) острого гастроэнтерита; д) правосторонней почечной коликой.
10. Клинически острый аппендицит может быть принят: а) за сальпингит; б) за острый холецистит; в) за дивертикулит Меккеля; г) за внематочную беременность; д) за любую из этих видов патологии.
11. Первично-гангренозный аппендицит чаще всего встречается: а) у детей; б) у лиц с тяжелой травмой; в) у мужчин; г) у женщин; д) у лиц пожилого и старческого возраста.
12. Противопоказанием к экстренной аппендэктомии является: а) аппендикулярный инфильтрат; б) инфаркт миокарда; в) вторая половина беременности; г) геморрагический диатез; д) разлитой перитонит.
13. Для диагностики острого аппендицита используются методы: а) лапароскопия; б) клинический анализ крови; в) ректальное исследование; г) термография; д) все перечисленное верно.
14. Острый холецистит обычно начинается с: а) повышения температуры; б) появления рвоты; в) болей в правом подреберье; г) расстройства стула; д) тяжести в эпигастральной области.
15. Приступ печеночной (желчной) колики возникает: а) внезапно, остро; б) после продромального периода; в) исподволь, постепенно; г) после длительного голодания; д) после переохлаждения.
16. Нормальные показатели билирубина крови: а) 0,10-0,68 мкмоль/л; б) 8,55-20,52 мкмоль/л; в) 2,50-8,33 мкмоль/л; г) 3,64-6,76 мкмоль/л; д) 7,62-12,88 мкмоль/л.
17. Ширина холедоха в норме равна: а) до 0,5; б) 0,6-1,0 см; в) 1,1-1,5 см; г) 1,6-2,0 см; д) свыше 2,0 см;
18. Больному с гангренозным холециститом показано: а) консервативное лечение; б) отсроченная операция; в) принятие решения зависит от возраста больного; г) операция при отсутствии эффекта от консервативной терапии; д) экстренная операция.
19. Больной желтухой на фоне холедохолитиаза нуждается в: а) экстренной операции; б) консервативном лечении; в) срочной операции после предоперационной подготовки; г) катетеризации чревной артерии; д) плазмаферезе.
20. К осложнениям острого калькулезного холецистита не относят: а) варикозное расширение вен пищевода; б) механическую желтуху; в) холангит; г) подпеченочный абсцесс; д) перитонит.
21. При остром калькулезном холецистите может применяться: а) экстренная операция; б) срочная операция; в) консервативная терапия и в дальнейшем плановая операция; г) только консервативная терапия; д) все перечисленное.
22. Симптом Курвуазье не характерен для: а) острого калькулезного холецистита; б) рака головки поджелудочной железы; в) индуративного панкреатита; г) опухоли большого дуоденального соска; д) опухоли холедоха.
23. Для уточнения характера желтухи и причины ее возникновения не используется: а) компьютерная томография; б) внутривенная холецистохолангиография; в) чрескожная чреспеченочная холангиография; г) эндоскопическая ретроградная панкреатохолангиография; д) УЗИ.
24. Наиболее оптимальный вид лечения холедохолитиаза у больных с постхолецист-эктомическим синдромом: а) эндоскопическая папилло-сфинктеротомия; б) холедохотомия; в) холедоходуоденоанастомоз; г) камнедробление; д) холедохоэнтеростомия.
25. Больной 35 лет, поступил в клинику с диагнозом острый панкреатит. Наиболее информативным тестом является исследование: а) амилазы крови; б) трипсиногена; в) аминотрансферазы; г) альдолазы; д) лактазы.
26. Больной поступил в клинику с подозрением на острый панкреатит. Укажите наиболее информативный метод диагностики заболевания: а) целиакография; б) ультразвуковое исследование; в) лапароцентез; г) термография; д) гастродуоденоскопия.
27. Механизм лечебного действия цитостатиков при остром панкреатите: а) блокада блуждающего нерва; б) уменьшение воспаления в железе; в) уменьшение болей; г) блокада белкового синтеза в железе; д) инактивация панкреатических ферментов.
28. У больного - клиническая картина острого панкреатита, нельзя исключить прободную язву желудка. Выберите достоверный лапароскопический признак деструктивного панкреатита: а) пневматизация кишечника; б) гиперемия брюшины; в) отек большого сальника; г) наличие крови в брюшной полости; д) бляшки стеатонекроза на брюшине.
29. Признаки инкреторной недостаточности поджелудочной железы при хроническом панкреатите: а) желтуха; б) частые потери сознания; в) высокое содержание сахара в крови и моче; г) увеличение печени, пальпируемый желчный пузырь; д) креаторея, стеаторея.
30. Больной в течение 15 лет страдает хроническим панкреатитом. Укажите простейший способ обнаружения кальциноза поджелудочной железы: а) эксплоративная лапаротомия; б) лапароскопия; в) ирригоскопия; г) холангиография; д) обзорная рентгенография брюшной полости.
31. В развитии острого панкреатита главенствующая роль принадлежит: а) микробной флоре; б) плазмоцитарной инфильтрации; в) микро-циркуляторным нарушениям; г) аутоферментной агрессии; д) венозному стазу.
32. Поперечная болевая резистентность передней брюшной стенки в проекции поджелудочной железы при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Керте; в) Грея-Турнера; г) Мондора; д) Воскресенского.
33. Болезненность при пальпации в левом реберно-позвоночном углу характерна для симптома: а) Воскресенского; б) Мейо-Робсона; в) Грюнвальда; г) Мондора; д) Грея-Турнера.
34. Развитие метеоризма у больных острым панкреатитом обусловлено: а) сдавлением 12-перстной кишки отечной головкой поджелудочной железы; б) частой неукротимой рвотой; в) парезом кишечника; г) дефицитом панкреатических гормонов; д) ферментативной недостаточностью поджелудочной железы.
35. Невозможность определения пульсации брюшного отдела аорты в эпигастрии при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Мондора; в) Кера; г) Куллена; д) Воскресенского.
36. К острому панкреатиту относятся все формы, кроме: а) отечного; б) псевдотумороз-ного панкреатита; в) жирового панкреонекроза; г) геморрагического панкреонекроза.
37. Основным в патогенетическом лечении острого панкреатита является: а) подавление секреторной функции поджелудочной железы; б) ликвидация гиповолемии; в) инактивация панкреатических ферментов; г) назогастральная декомпрессия желудочно-кишечного тракта; д) введение цитостатиков.
38. Инвагинация относится к непроходимости: а) спастической; б) паралитической; в) обтурационной; г) странгуляционной; д) смешанной.
39. Выявление геморрагического выпота в брюшной полости и очагов жирового некроза на брюшине позволяет думать: а) о повреждении полого органа; б) о разрыве печени; в) об остром панкреатите; г) о перфоративной язве желудка; д) о мезентериальном тромбозе.
40. Наиболее ранним и постоянным симптомом острой тонкокишечной непроходи-мости является: а) задержка стула и газов; б) усиление перистальтики;в) схваткообразные боли в животе; г) асимметрия живота; д) рвота.
41. При узлообразовании, ущемлении кишки и завороте: а) следует проводить консервативные мероприятия по разрешению непроходимости; б) показана экстренная операция; в) предпочтительна операция в "холодном" периоде; г) необходимо динамическое наблюдение; д) все ответы не верны.
42. При острой кишечной непроходимости практически не используется лишь: а) ангиография чревной артерии; б) лабораторные исследования; в) аускультация живота; г) обзорная рентгенография брюшной полости; д) пальцевое исследование прямой кишки.
43. Для низкой толстокишечной непроходимости характерно все, кроме: а) постепенного нарастания симптомов; б) вздутия живота; в) появление чаш Клойбера; г) задержки стула; д) быстрого (в течение суток) обезвоживания.
44. При острой обтурационной толстокишечной непроходимости наблюдается все, кроме: а) схваткообразных болей в животе; б) вздутия живота; в) постепенного развития перитонита; г) постоянных болей в животе; д) задержки стула и газов.
45. Не нарушается кровообращение в брыжейке кишки при: а) завороте; б) обтурации; в) узлообразовании; г) инвагинации;д) ущемлении.
46. Консервативное лечение острой кишечной непроходимости применяется только при: а) завороте; б) узлообразовании; в).обтурационной кишечной непроходимости; г) динамической непроходимости; д) обтурации желчным камнем.
47. Толстокишечная обтурационная непроходимость чаще всего вызывается: а) инородными телами; б) желчными камнями; в) злокачественными опухолями; г) спайками брюшной полости; д) гельминтами.
48. Нижней стенкой пахового канала является: а) поперечная фасция; б) нижний край наружной косой мышцы живота; в) жимбернатова связка; г) паховая связка; д) край подвздошной кости.
49. Рихтеровским называется ущемление: а) пристеночное; б) сигмовидной кишки в скользящей грыже; в) желудка в диафрагмальной грыже; г) Меккелева дивертикула; д) червеобразного отростка.
50. Пахово-мошоночную грыжу дифференцируют со всем, кроме: а) варикоцеле; б) опухоли семенного канатика; в) опухоли яичка; г) гидроцеле; д) аневризмы v. saphena magna.
51. При ущемленной абдоминальной грыже независимо от состояния больного показано: а) спазмолитики и теплая ванна; б) наблюдение; в) антибиотики и строгий постельный режим; г) обзорная рентгенография брюшной полости; д) экстренная операция.
52. О чем говорит тимпанический звук при перкуссии грыжевого выпячивания? а) о водянке яичка; б) о наличии петли кишки; в) о лимфадените; г) об опухоли; д) об изменениях в семенном канатике.
53. При ущемлении грыжи у больного с острым инфарктом миокарда показано: а) наблюдение, холод на живот; б) вправление грыжи; в) введение спазмолитиков; г) положение Тренделенбурга; д) экстренная операция.
54. Наличие яичка в грыжевом мешке характерно для грыжи: а) скользящей; б) ущемленной; в) бедренной; г) врожденной; д) косой паховой.
55. Прямую паховую грыжу характеризует слабость стенки: а) задней; б) верхней; в) передней; г) нижней; д) всех стенок.
56. Грыжевой мешок врожденной грыжи образован: а) париетальной брюшиной; б) брыжейкой кишки; в) влагалищным отростком брюшины; г) висцеральной брюшиной; д) поперечной фасцией;
57. Больному с ущемленной грыжей перед операцией проводят: а) паранефральную блокаду; б) очистительную клизму; в) блокаду семенного канатика; г) бритье области операции; д) промывание желудка.
58. При флегмоне грыжевого мешка операцию начинают: а) с вскрытия флегмоны; б) со срединной лапаротомии; в) с выделения грыжевого мешка из окружающих тканей; г) с пункции грыжевого мешка; д) с одновременной операции из двух доступов.
59. Этиопатогенетически обоснованным методом операции при неосложненной дуоденальной язве является: а) селективная проксимальная ваготомия; б) идеальная антрумэктомия; в) сочетание антрумэктомии с ваготомией; г) высокая (2/3 и более) резекция желудка; д) стволовая или селективная ваготомия.
60. Наиболее частым осложнением язвы передней стенки 12-перстной кишки является: а) перфорация; б) кровотечение; в) пенетрация в головку поджелудочной железы; г) малигнизация; д) все неверно.
61. Крайне редким осложнением язвы 12-перстной кишки является: а) перфорация; б) малигнизация; в) кровотечение; г) пенетрация; д) рубцовая деформация кишки.
62. Достоверным рентгенологическим признаком перфорации гастродуоденальной язвы является: а) высокое стояние диафрагмы; б) наличие свободного газа в брюшной полости; в) пневматизация кишечника; г) "чаши" Клойбера; д) увеличенный газовый пузырь желудка.
63. Срыгивание пенистой кровью ярко-красного цвета, усиливающееся при кашле, характерно для: а) кровоточащей язвы желудка; б) опухоли кардии; в) синдрома Маллори-Вейсса; г) легочного кровотечения; д) синдрома Рандю-Ослера.
64. Для перфоративной гастродуоденальной язвы характерно: а) внезапное начало с резких болей в эпигастрии; б) постепенное нарастание болевого синдрома; в) схваткообразные резкие боли; г) обильная многократная рвота; д) быстро нарастающая слабость, головокружение.
65. Наиболее частым осложнением пенетрирующей язвы желудка является: а) развитие стеноза привратника; б) малигнизация язвы; в) образование межорганного свища; г) профузное кровотечение; д) перфорация.
66. Характер оперативного вмешательства при прободной язве желудка определяет: а) возраст больного; б) локализация перфоративного отверстия; в) степень выраженности перитонита; г) срок с момента перфорации; д) все перечисленное.
67. Для выявления типичных отдаленных метастазов рака прямой кишки используется: а) лабораторное исследование; б) пальцевое исследование прямой кишки; в) лапароскопия; г) ректороманоскопия; д) ирригоскопия.
68. При раке прямой кишки на 12 см от анального отверстия без метастазов целесообразна: а) экстирпация прямой кишки по Кеню-Майлсу; б) операция Гартмана; в) передняя резекция прямой кишки; г) наложение цекостомы; д) наложение сигмостомы.
69. Токсикоанемическая форма характерна для рака толстой кишки: а) поперечно-ободочной; б) левых отделов; в) правых отделов; г) прямой; д) сигмовидной.
70. Наиболее тяжелой формой острого парапроктита является: а) ишиоректальный; б) ретроректальный; в) подслизистый; г) пельвиоректальный; д) подкожный.
71. Для исследования свищей прямой кишки применяются: а) наружный осмотр и пальпация; б) пальцевое исследование прямой кишки; в) прокрашивание свищевого хода и зондирование; г) фистулография; д) все перечисленное.
72. При кровотечении после дефекации в виде струйки крови и зуде в области анального отверстия можно думать: а) о параректальном свище; б) о геморрое; в) о раке прямой кишки; г) о полипе прямой кишки; д) о трещине анального канала.
73. К облигатным предракам ободочной кишки относят: а) ювенильные полипы; б) одиночный полип ободочной кишки; в) регионарный энтерит; г) терминальный илеит; д) диффузный семейный полипоз.
74. Основной гистологической формой рака толстой кишки является: а) скирр; б) перстневидноклеточный (слизистый); в) плоскоклеточный (ороговевающий); г) аденокарцинома; д) недифференцированный.
75. Для подтверждения диагноза трещины анального прохода используется: а) аноскопия; б) измерение давления в прямой кишке; в) колоноскопия; г) ректоскопия; д) ирригоскопия.
76. Наиболее информативным методом инструментальной диагностики острой кишечной непроходимости является: а) обзорная рентгенография брюшной полости; б) лапароскопия; в) ангиография; г) гастроскопия; д) колоноскопия.
77. Для поздней стадии перитонита характерно все, кроме: а) вздутия живота; б) гиповолемии; в) исчезновения кишечных шумов; г) гипопротеинемии; д) усиленной перистальтики.
78. Как устанавливается диагноз общего перитонита до операции? а) рентгенологически; б) анамнестически; в) лабораторным определением признаков воспалительной реакции; г) по клиническим признакам; д) по уровню секреции желудочного сока.
79. Эпителиальный копчиковый ход: а) связан с крестцом; б) связан с копчиком; в) оканчивается слепо в подкожной клетчатке межягодичной области; г) расположен между задней поверхностью прямой кишки и передней поверхностью крестца; д) сообщается с просветом прямой кишки.
80. Наиболее часто проявляется дисфагией рак желудка, локализующийся: а) в пилорическом отделе; б) в кардии; в) в теле желудка; г) по большой кривизне; д) в области дна.
81. Метастаз Крукенберга локализуется: а) в прямокишечно-пузырной складке; б) в пупке; в) в яичниках; г) между ножками кивательной мышцы; д) в печени.
82. Метастаз Вирхова локализуется: а) в печени; б) в прямокишечно-пузырной складке; в) в яичниках; г) между ножками кивательной мышцы; д) в легких.
83. Наиболее раннюю диагностику рака желудка обеспечивает: а) гастроскопия; б) поиск синдрома "малых признаков"; в) появление раковой триады по Мельникову; г) рентгенография желудка; д) обзорная рентгеноскопия брюшной полости.
84. Для острого пневмоторакса не характерна: а) одышка в покое; б) болевой синдром вплоть до шока; в) горизонтальный уровень жидкости в плевральной полости; г) тахикардия; д) изменение перкуторного звука.
85. Для выявления бронхоэктазов ведущее значение имеет: а) рентгенография легких; б) томография; в) бронхография; г) бронхоскопия; д) ультразвуковое исследование.
86. Наиболее частой причиной спонтанного пневмоторакса служит: а) абсцесс легкого; б) рак легкого; в) бронхоэктазы; г) буллезные кисты легкого; д) ателектаз легкого.
87. Неотложная помощь при клапанном пневмотораксе начинается: а) с дренажа плевральной полости; б) с трахеостомии; в) с блокады межреберных нервов; г) с обездвиживания грудной клетки; д) с блокады диафрагмального нерва.
88. При тампонаде сердца показана: а) пункция перикарда; б) переливание крови; в) мочегонные; г) гемостатическая терапия; д) антибиотики.
89. Проявлением тиреотоксикоза не является: а) симптом Греффе и Мебиуса; б) тахикардия; в) экзофтальм; г) тремор нижних конечностей; д) увеличение щитовидной железы.
90. К осложнениям варикозной болезни относят: а) пигментацию кожи; б) индурацию подкожной клетчатки; в) трофические язвы; г) тромбофлебит; д) слоновость.
91. Для выявления несостоятельности клапанов поверхностных вен используется проба: а) трехжгутовая (Шейниса); б) маршевая (Дельбе-Пертеса); в) Троянова-Тренделенбурга; г) Пратта; д) Тальмана.
92. При первичном варикозном расширении вен нижних конечностей показано: а) эластичное бинтование; б) хирургическое лечение; в) лечебная физкультура; г) массаж; д) рефлексотерапия.
93. Наиболее опасным осложнением тромбоза глубоких вен является: а) трофическая язва голени; б) эмболия легочной артерии; в) тромбофлебит поверхностных вен; г) облитерация глубоких вен; д) слоновость.
94. Клиническими симптомами тромбоэмболии легочной артерии являются все, кроме: а) боли за грудиной; б) коллапса; в) удушья; г) цианоза лица и верхней половины туловища; д) ослабления дыхания.
95. Наиболее точным методом диагностики тромбоэмболии легочной артерии является: а) обзорная рентгенография грудной клетки; б) ЭКГ; в) радиокардиография; г) фонокардиография; д) перфузионное сканирование легких.
96. Сущность пробы Оппеля состоит в: а) утомлении ног; б) реактивной гиперемии; в) побледнении подошвенной поверхности стопы; г) побледнении пальцев; д) боли в икроножных мышцах.
97. Синдром Лериша может быть причиной тромбоза: а) бедренной артерии; б) подколенной артерии; в) бифуркации аорты и подвздошной артерии; г) почечных артерий; д) тромбоэмболии легочной артерии.
98. Наиболее частой причиной острого артериального тромбоза является: а) облитерирующий тромбангиит; б) облитерирующий атеросклероз; в) пункция и катетеризация артерий; г) экстравазальная компрессия артерий; д) полицитемия.
99. Для острой артериальной недостаточности конечностей не характерно: а) отсутствие пульса; б) парастезии; в) трофические язвы голени; г) паралич конечностей; д) бледность кожи и боли.
100. При быстро прогрессирующей гангрене стопы необходимо: а) сделать множественные разрезы кожи стопы; б) срочно выполнить ампутацию; в) произвести шунтирование артерий; г) пытаться перевести влажную гангрену в сухую; д) проводить массивную антибиотикотерапию.
Вариант 2
1. Больной 35 лет, поступил в клинику с диагнозом острый панкреатит. Наиболее информативным тестом является исследование: а) амилазы крови; б) трипсиногена; в) аминотрансферазы; г) альдолазы; д) лактазы.
2. Больной поступил в клинику с подозрением на острый панкреатит. Укажите наиболее информативный метод диагностики заболевания: а) целиакография; б) ультразвуковое исследование; в) лапароцентез; г) термография; д) гастродуоденоскопия.
3. Механизм лечебного действия цитостатиков при остром панкреатите: а) блокада блуждающего нерва; б) уменьшение воспаления в железе; в) уменьшение болей; г) блокада белкового синтеза в железе; д) инактивация панкреатических ферментов.
4. У больного - клиническая картина острого панкреатита, нельзя исключить прободную язву желудка. Выберите достоверный лапароскопический признак деструктивного панкреатита: а) пневматизация кишечника; б) гиперемия брюшины; в) отек большого сальника; г) наличие крови в брюшной полости; д) бляшки стеатонекроза на брюшине.
5. Признаки инкреторной недостаточности поджелудочной железы при хроническом панкреатите: а) желтуха; б) частые потери сознания; в) высокое содержание сахара в крови и моче; г) увеличение печени, пальпируемый желчный пузырь; д) креаторея, стеаторея.
6. Больной в течение 15 лет страдает хроническим панкреатитом. Укажите простейший способ обнаружения кальциноза поджелудочной железы: а) эксплоративная лапаротомия; б) лапароскопия; в) ирригоскопия; г) холангиография; д) обзорная рентгенография брюшной полости.
7. В развитии острого панкреатита главенствующая роль принадлежит: а) микробной флоре; б) плазмоцитарной инфильтрации; в) микро-циркуляторным нарушениям; г) аутоферментной агрессии; д) венозному стазу.
8. Поперечная болевая резистентность передней брюшной стенки в проекции поджелудочной железы при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Керте; в) Грея-Турнера; г) Мондора; д) Воскресенского.
9. Болезненность при пальпации в левом реберно-позвоночном углу характерна для симптома: а) Воскресенского; б) Мейо-Робсона; в) Грюнвальда; г) Мондора; д) Грея-Турнера.
10. Развитие метеоризма у больных острым панкреатитом обусловлено: а) сдавлением 12-перстной кишки отечной головкой поджелудочной железы; б) частой неукротимой рвотой; в) парезом кишечника; г) дефицитом панкреатических гормонов; д) ферментативной недостаточностью поджелудочной железы.
11. Невозможность определения пульсации брюшного отдела аорты в эпигастрии при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Мондора; в) Кера; г) Куллена; д) Воскресенского.
12. К острому панкреатиту относятся все формы, кроме: а) отечного; б) псевдотумороз-ного панкреатита; в) жирового панкреонекроза; г) геморрагического панкреонекроза.
13. Основным в патогенетическом лечении острого панкреатита является: а) подавление секреторной функции поджелудочной железы; б) ликвидация гиповолемии; в) инактивация панкреатических ферментов; г) назогастральная декомпрессия желудочно-кишечного тракта; д) введение цитостатиков.
14. Инвагинация относится к непроходимости: а) спастической; б) паралитической; в) обтурационной; г) странгуляционной; д) смешанной.
15. Выявление геморрагического выпота в брюшной полости и очагов жирового некроза на брюшине позволяет думать: а) о повреждении полого органа; б) о разрыве печени; в) об остром панкреатите; г) о перфоративной язве желудка; д) о мезентериальном тромбозе.
16. Наиболее ранним и постоянным симптомом острой тонкокишечной непроходи-мости является: а) задержка стула и газов; б) усиление перистальтики;в) схваткообразные боли в животе; г) асимметрия живота; д) рвота.
17. При узлообразовании, ущемлении кишки и завороте: а) следует проводить консервативные мероприятия по разрешению непроходимости; б) показана экстренная операция; в) предпочтительна операция в "холодном" периоде; г) необходимо динамическое наблюдение; д) все ответы не верны.
18. При острой кишечной непроходимости практически не используется лишь: а) ангиография чревной артерии; б) лабораторные исследования; в) аускультация живота; г) обзорная рентгенография брюшной полости; д) пальцевое исследование прямой кишки.
19. Для низкой толстокишечной непроходимости характерно все, кроме: а) постепенного нарастания симптомов; б) вздутия живота; в) появление чаш Клойбера; г) задержки стула; д) быстрого (в течение суток) обезвоживания.
20. При острой обтурационной толстокишечной непроходимости наблюдается все, кроме: а) схваткообразных болей в животе; б) вздутия живота; в) постепенного развития перитонита; г) постоянных болей в животе; д) задержки стула и газов.
21. Не нарушается кровообращение в брыжейке кишки при: а) завороте; б) обтурации; в) узлообразовании; г) инвагинации;д) ущемлении.
22. Консервативное лечение острой кишечной непроходимости применяется только при: а) завороте; б) узлообразовании; в) обтурационной кишечной непроходимости; г) динамической непроходимости; д) обтурации желчным камнем.
23. Толстокишечная обтурационная непроходимость чаще всего вызывается: а) инородными телами; б) желчными камнями; в) злокачественными опухолями; г) спайками брюшной полости; д) гельминтами.
24. Нижней стенкой пахового канала является: а) поперечная фасция; б) нижний край наружной косой мышцы живота; в) жимбернатова связка; г) паховая связка; д) край подвздошной кости.
25. Рихтеровским называется ущемление: а) пристеночное; б) сигмовидной кишки в скользящей грыже; в) желудка в диафрагмальной грыже; г) Меккелева дивертикула; д) червеобразного отростка.
26. Наиболее информативным методом инструментальной диагностики острой кишечной непроходимости является: а) обзорная рентгенография брюшной полости; б) лапароскопия; в) ангиография; г) гастроскопия; д) колоноскопия.
27. Для поздней стадии перитонита характерно все, кроме: а) вздутия живота; б) гиповолемии; в) исчезновения кишечных шумов; г) гипопротеинемии; д) усиленной перистальтики.
28. Как устанавливается диагноз общего перитонита до операции? а) рентгенологически; б) анамнестически; в) лабораторным определением признаков воспалительной реакции; г) по клиническим признакам; д) по уровню секреции желудочного сока.
29. Эпителиальный копчиковый ход: а) связан с крестцом; б) связан с копчиком; в) оканчивается слепо в подкожной клетчатке межягодичной области; г) расположен между задней поверхностью прямой кишки и передней поверхностью крестца; д) сообщается с просветом прямой кишки.
30. Наиболее часто проявляется дисфагией рак желудка, локализующийся: а) в пилорическом отделе; б) в кардии; в) в теле желудка; г) по большой кривизне; д) в области дна.
31. Метастаз Крукенберга локализуется: а) в прямокишечно-пузырной складке; б) в пупке; в) в яичниках; г) между ножками кивательной мышцы; д) в печени.
32. Метастаз Вирхова локализуется: а) в печени; б) в прямокишечно-пузырной складке; в) в яичниках; г) между ножками кивательной мышцы; д) в легких.
33. Наиболее раннюю диагностику рака желудка обеспечивает: а) гастроскопия; б) поиск синдрома "малых признаков"; в) появление раковой триады по Мельникову; г) рентгенография желудка; д) обзорная рентгеноскопия брюшной полости.
34. Для острого пневмоторакса не характерна: а) одышка в покое; б) болевой синдром вплоть до шока; в) горизонтальный уровень жидкости в плевральной полости; г) тахикардия; д) изменение перкуторного звука.
35. Для выявления бронхоэктазов ведущее значение имеет: а) рентгенография легких; б) томография; в) бронхография; г) бронхоскопия; д) ультразвуковое исследование.
36. Наиболее частой причиной спонтанного пневмоторакса служит: а) абсцесс легкого; б) рак легкого; в) бронхоэктазы; г) буллезные кисты легкого; д) ателектаз легкого.
37. Неотложная помощь при клапанном пневмотораксе начинается: а) с дренажа плевральной полости; б) с трахеостомии; в) с блокады межреберных нервов; г) с обездвиживания грудной клетки; д) с блокады диафрагмального нерва.
38. При тампонаде сердца показана: а) пункция перикарда; б) переливание крови; в) мочегонные; г) гемостатическая терапия; д) антибиотики.
39. Проявлением тиреотоксикоза не является: а) симптом Греффе и Мебиуса; б) тахикардия; в) экзофтальм; г) тремор нижних конечностей; д) увеличение щитовидной железы.
40. К осложнениям варикозной болезни относят: а) пигментацию кожи; б) индурацию подкожной клетчатки; в) трофические язвы; г) тромбофлебит; д) слоновость.
41. Для выявления несостоятельности клапанов поверхностных вен используется проба: а) трехжгутовая (Шейниса); б) маршевая (Дельбе-Пертеса); в) Троянова-Тренделенбурга; г) Пратта; д) Тальмана.
42. При первичном варикозном расширении вен нижних конечностей показано: а) эластичное бинтование; б) хирургическое лечение; в) лечебная физкультура; г) массаж; д) рефлексотерапия.
43. Наиболее опасным осложнением тромбоза глубоких вен является: а) трофическая язва голени; б) эмболия легочной артерии; в) тромбофлебит поверхностных вен; г) облитерация глубоких вен; д) слоновость.
44. Клиническими симптомами тромбоэмболии легочной артерии являются все, кроме: а) боли за грудиной; б) коллапса; в) удушья; г) цианоза лица и верхней половины туловища; д) ослабления дыхания.
45. Наиболее точным методом диагностики тромбоэмболии легочной артерии является: а) обзорная рентгенография грудной клетки; б) ЭКГ; в) радиокардиография; г) фонокардиография; д) перфузионное сканирование легких.
46. Сущность пробы Оппеля состоит в: а) утомлении ног; б) реактивной гиперемии; в) побледнении подошвенной поверхности стопы; г) побледнении пальцев; д) боли в икроножных мышцах.
47. Синдром Лериша может быть причиной тромбоза: а) бедренной артерии; б) подколенной артерии; в) бифуркации аорты и подвздошной артерии; г) почечных артерий; д) тромбоэмболии легочной артерии.
48. Наиболее частой причиной острого артериального тромбоза является: а) облитерирующий тромбангиит; б) облитерирующий атеросклероз; в) пункция и катетеризация артерий; г) экстравазальная компрессия артерий; д) полицитемия.
49. Для острой артериальной недостаточности конечностей не характерно: а) отсутствие пульса; б) парастезии; в) трофические язвы голени; г) паралич конечностей; д) бледность кожи и боли.
50. При быстро прогрессирующей гангрене стопы необходимо: а) сделать множественные разрезы кожи стопы; б) срочно выполнить ампутацию; в) произвести шунтирование артерий; г) пытаться перевести влажную гангрену в сухую; д) проводить массивную антибиотикотерапию.
51. Пахово-мошоночную грыжу дифференцируют со всем, кроме: а) варикоцеле; б) опухоли семенного канатика; в) опухоли яичка; г) гидроцеле; д) аневризмы v. saphena magna.
52. При ущемленной абдоминальной грыже независимо от состояния больного показано: а) спазмолитики и теплая ванна; б) наблюдение; в) антибиотики и строгий постельный режим; г) обзорная рентгенография брюшной полости; д) экстренная операция.
53. О чем говорит тимпанический звук при перкуссии грыжевого выпячивания? а) о водянке яичка; б) о наличии петли кишки; в) о лимфадените; г) об опухоли; д) об изменениях в семенном канатике.
54. При ущемлении грыжи у больного с острым инфарктом миокарда показано: а) наблюдение, холод на живот; б) вправление грыжи; в) введение спазмолитиков; г) положение Тренделенбурга; д) экстренная операция.
55. Наличие яичка в грыжевом мешке характерно для грыжи: а) скользящей; б) ущемленной; в) бедренной; г) врожденной; д) косой паховой.
56. Прямую паховую грыжу характеризует слабость стенки: а) задней; б) верхней; в) передней; г) нижней; д) всех стенок.
57. Грыжевой мешок врожденной грыжи образован: а) париетальной брюшиной; б) брыжейкой кишки; в) влагалищным отростком брюшины; г) висцеральной брюшиной; д) поперечной фасцией;
58. Больному с ущемленной грыжей перед операцией проводят: а) паранефральную блокаду; б) очистительную клизму; в) блокаду семенного канатика; г) бритье области операции; д) промывание желудка.
59. При флегмоне грыжевого мешка операцию начинают: а) с вскрытия флегмоны; б) со срединной лапаротомии; в) с выделения грыжевого мешка из окружающих тканей; г) с пункции грыжевого мешка; д) с одновременной операции из двух доступов.
60. Этиопатогенетически обоснованным методом операции при неосложненной дуоденальной язве является: а) селективная проксимальная ваготомия; б) идеальная антрумэктомия; в) сочетание антрумэктомии с ваготомией; г) высокая (2/3 и более) резекция желудка; д) стволовая или селективная ваготомия.
61. Наиболее частым осложнением язвы передней стенки 12-перстной кишки является: а) перфорация; б) кровотечение; в) пенетрация в головку поджелудочной железы; г) малигнизация; д) все неверно.
62. Крайне редким осложнением язвы 12-перстной кишки является: а) перфорация; б) малигнизация; в) кровотечение; г) пенетрация; д) рубцовая деформация кишки.
63. Достоверным рентгенологическим признаком перфорации гастродуоденальной язвы является: а) высокое стояние диафрагмы; б) наличие свободного газа в брюшной полости; в) пневматизация кишечника; г) "чаши" Клойбера; д) увеличенный газовый пузырь желудка.
64. Срыгивание пенистой кровью ярко-красного цвета, усиливающееся при кашле, характерно для: а) кровоточащей язвы желудка; б) опухоли кардии; в) синдрома Маллори-Вейсса; г) легочного кровотечения; д) синдрома Рандю-Ослера.
65. Для перфоративной гастродуоденальной язвы характерно: а) внезапное начало с резких болей в эпигастрии; б) постепенное нарастание болевого синдрома; в) схваткообразные резкие боли; г) обильная многократная рвота; д) быстро нарастающая слабость, головокружение.
66. Наиболее частым осложнением пенетрирующей язвы желудка является: а) развитие стеноза привратника; б) малигнизация язвы; в) образование межорганного свища; г) профузное кровотечение; д) перфорация.
67. Характер оперативного вмешательства при прободной язве желудка определяет: а) возраст больного; б) локализация перфоративного отверстия; в) степень выраженности перитонита; г) срок с момента перфорации; д) все перечисленное.
68. Для выявления типичных отдаленных метастазов рака прямой кишки используется: а) лабораторное исследование; б) пальцевое исследование прямой кишки; в) лапароскопия; г) ректороманоскопия; д) ирригоскопия.
69. При раке прямой кишки на 12 см от анального отверстия без метастазов целесообразна: а) экстирпация прямой кишки по Кеню-Майлсу; б) операция Гартмана; в) передняя резекция прямой кишки; г) наложение цекостомы; д) наложение сигмостомы.
70. Токсикоанемическая форма характерна для рака толстой кишки: а) поперечно-ободочной; б) левых отделов; в) правых отделов; г) прямой; д) сигмовидной.
71. Наиболее тяжелой формой острого парапроктита является: а) ишиоректальный; б) ретроректальный; в) подслизистый; г) пельвио-ректальный; д) подкожный.
72. Для исследования свищей прямой кишки применяются: а) наружный осмотр и пальпация; б) пальцевое исследование прямой кишки; в) прокрашивание свищевого хода и зондирование; г) фистулография; д) все перечисленное.
73. При кровотечении после дефекации в виде струйки крови и зуде в области анального отверстия можно думать: а) о параректальном свище; б) о геморрое; в) о раке прямой кишки; г) о полипе прямой кишки; д) о трещине анального канала.
74. К облигатным предракам ободочной кишки относят: а) ювенильные полипы; б) одиночный полип ободочной кишки; в) регионарный энтерит; г) терминальный илеит; д) диффузный семейный полипоз.
75. Основной гистологической формой рака толстой кишки является: а) скирр; б) перстневидноклеточный (слизистый); в) плоскоклеточный (ороговевающий); г) аденокарцинома; д) недифференцированный.
76. Для подтверждения диагноза трещины анального прохода используется: а) аноскопия; б) измерение давления в прямой кишке; в) колоноскопия; г) ректоскопия; д) ирригоскопия.
77.Что из указанных средств и методов не следует применять при лечении гнойных ран в фазе гидратации? а) мазевые повязки; б) покой; в) антибиотикотерапию; г) промывание перекисью водорода; д) теплые марганцевые ванны.
78. Для фазы дегидратации в течении раневого процесса характерно: а)отек краев раны; б)гиперемия краев раны; в)дно раны покрыто фибрином; г)появление грануляций; д)лейкоцитарная инфильтрация тканей.
79. Лечение гнойных ран конечностей в фазе дегидратации: что не следует применять из указанного? а) витаминотерапию; б) сближение краев раны; в) повязки с гипертоническими растворами; г) переливание крови; д) повязки с мазью Вишневского.
80. Каковы оптимальные сроки для проведения первичной хирургической обработки раны? а) до 6 час; б) до 8 час; в) до 12 час; г) до 18 час; д) до 24 час.
81. Больному с AB(IV) группой крови по жизненным показаниям необходимо перелить кровь. Определить резус-фактор нет ни времени, ни возможности. Какой группы и "резуса" кровь предпочтительнее при этом перелить больному? а) AB(IV) резус-положительную; б) AB(IV) резус-отрицательную; в) В(III) резус-положительную; г) А(II) резус-отрицательную; д) О(I) резус-положительную.
82. Какой из ниже перечисленных возбудителей сепсиса наиболее часто дает метастазирование? а) стрептококк; б) стафилококк; в) пневмококк; г) гонококк; д) кишечная палочка.
83. Для острого аппендицита не характерен симптом: а) Ровзинга; б) Воскресенского; в) Мерфи; г) Образцова; д) Бартомье-Михельсона.
84. К перитонеальным симптомам при остром аппендиците относят симптомы: а) Воскресенского (симптом «рубашки»); б) Щеткина-Блюмберга; в) Раздольского; г) все названные симптомы; д) ни один из них.
85. Острый аппендицит следует дифференцировать со всеми перечисленными заболеваниями, кроме: а) гломерулонефрита; б) острого панкреатита; в) острого аднексита; г) острого гастроэнтерита; д) правосторонней почечной коликой.
86. Клинически острый аппендицит может быть принят: а) за сальпингит; б) за острый холецистит; в) за дивертикулит Меккеля; г) за внематочную беременность; д) за любую из этих видов патологии.
87. Первично-гангренозный аппендицит чаще всего встречается: а) у детей; б) у лиц с тяжелой травмой; в) у мужчин; г) у женщин; д) у лиц пожилого и старческого возраста.
88. Противопоказанием к экстренной аппендэктомии является: а) аппендикулярный инфильтрат; б) инфаркт миокарда; в) вторая половина беременности; г) геморрагический диатез; д) разлитой перитонит.
89. Для диагностики острого аппендицита используются методы: а) лапароскопия; б) клинический анализ крови; в) ректальное исследование; г) термография; д) все перечисленное верно.
90. Острый холецистит обычно начинается с: а) повышения температуры; б) появления рвоты; в) болей в правом подреберье; г) расстройства стула; д) тяжести в эпигастральной области.
91. Приступ печеночной (желчной) колики возникает: а) внезапно, остро; б) после продромального периода; в) исподволь, постепенно; г) после длительного голодания; д) после переохлаждения.
92. Нормальные показатели билирубина крови: а) 0,10-0,68 мкмоль/л; б) 8,55-20,52 мкмоль/л; в) 2,50-8,33 мкмоль/л; г) 3,64-6,76 мкмоль/л; д) 7,62-12,88 мкмоль/л.
93. Ширина холедоха в норме равна: а) до 0,5; б) 0,6-1,0 см; в) 1,1-1,5 см; г) 1,6-2,0 см; д) свыше 2,0 см;
94. Больному с гангренозным холециститом показано: а) консервативное лечение; б) отсроченная операция; в) принятие решения зависит от возраста больного; г) операция при отсутствии эффекта от консервативной терапии; д) экстренная операция.
95. Больной желтухой на фоне холедохолитиаза нуждается в: а) экстренной операции; б) консервативном лечении; в) срочной операции после предоперационной подготовки; г) катетеризации чревной артерии; д) плазмаферезе.
96. К осложнениям острого калькулезного холецистита не относят: а) варикозное расширение вен пищевода; б) механическую желтуху; в) холангит; г) подпеченочный абсцесс; д) перитонит.
97. При остром калькулезном холецистите может применяться: а) экстренная операция; б) срочная операция; в) консервативная терапия и в дальнейшем плановая операция; г) только консервативная терапия; д) все перечисленное.
98. Симптом Курвуазье не характерен для: а) острого калькулезного холецистита; б) рака головки поджелудочной железы; в) индуративного панкреатита; г) опухоли большого дуоденального соска; д) опухоли холедоха.
99. Для уточнения характера желтухи и причины ее возникновения не используется: а) компьютерная томография; б) внутривенная холецисто-холангиография; в) чрескожная чреспеченочная холангиография; г) эндоскопическая ретроградная панкреатохолангиография; д) УЗИ.
100. Наиболее оптимальный вид лечения холедохолитиаза у больных с постхолецист-эктомическим синдромом: а) эндоскопическая папилло-сфинктеротомия; б) холедохотомия; в) холедоходуоденоанастомоз; г) камнедробление; д) холедохоэнтеростомия.
Вариант 3
1. Пахово-мошоночную грыжу дифференцируют со всем, кроме: а) варикоцеле; б) опухоли семенного канатика; в) опухоли яичка; г) гидроцеле; д) аневризмы v. saphena magna.
2. При ущемленной абдоминальной грыже независимо от состояния больного показано: а) спазмолитики и теплая ванна; б) наблюдение; в) антибиотики и строгий постельный режим; г) обзорная рентгенография брюшной полости; д) экстренная операция.
3. О чем говорит тимпанический звук при перкуссии грыжевого выпячивания? а) о водянке яичка; б) о наличии петли кишки; в) о лимфадените; г) об опухоли; д) об изменениях в семенном канатике.
4. При ущемлении грыжи у больного с острым инфарктом миокарда показано: а) наблюдение, холод на живот; б) вправление грыжи; в) введение спазмолитиков; г) положение Тренделенбурга; д) экстренная операция.
5. Наличие яичка в грыжевом мешке характерно для грыжи:
а) скользящей; б) ущемленной; в) бедренной; г) врожденной; д) косой паховой.
6. Прямую паховую грыжу характеризует слабость стенки: а) задней; б) верхней; в) передней; г) нижней; д) всех стенок.
7. Грыжевой мешок врожденной грыжи образован: а) париетальной брюшиной; б) брыжейкой кишки; в) влагалищным отростком брюшины; г) висцеральной брюшиной; д) поперечной фасцией;
8. Больному с ущемленной грыжей перед операцией проводят: а) паранефральную блокаду; б) очистительную клизму; в) блокаду семенного канатика; г) бритье области операции; д) промывание желудка.
9. При флегмоне грыжевого мешка операцию начинают: а) с вскрытия флегмоны; б) со срединной лапаротомии; в) с выделения грыжевого мешка из окружающих тканей; г) с пункции грыжевого мешка; д) с одновременной операции из двух доступов.
10. Этиопатогенетически обоснованным методом операции при неосложненной дуоденальной язве является: а) селективная проксимальная ваготомия; б) идеальная антрумэктомия; в) сочетание антрумэктомии с ваготомией; г) высокая (2/3 и более) резекция желудка; д) стволовая или селективная ваготомия.
11. Наиболее частым осложнением язвы передней стенки 12-перстной кишки является: а) перфорация; б) кровотечение; в) пенетрация в головку поджелудочной железы; г) малигнизация; д) все неверно.
12. Крайне редким осложнением язвы 12-перстной кишки является: а) перфорация; б) малигнизация; в) кровотечение; г) пенетрация; д) рубцовая деформация кишки.
13. Достоверным рентгенологическим признаком перфорации гастродуоденальной язвы является: а) высокое стояние диафрагмы; б) наличие свободного газа в брюшной полости; в) пневматизация кишечника; г) "чаши" Клойбера; д) увеличенный газовый пузырь желудка.
14. Срыгивание пенистой кровью ярко-красного цвета, усиливающееся при кашле, характерно для: а) кровоточащей язвы желудка; б) опухоли кардии; в) синдрома Маллори-Вейсса; г) легочного кровотечения; д) синдрома Рандю-Ослера.
15. Для перфоративной гастродуоденальной язвы характерно: а) внезапное начало с резких болей в эпигастрии; б) постепенное нарастание болевого синдрома; в) схваткообразные резкие боли; г) обильная многократная рвота; д) быстро нарастающая слабость, головокружение.
16. Наиболее частым осложнением пенетрирующей язвы желудка является: а) развитие стеноза привратника; б) малигнизация язвы; в) образование межорганного свища; г) профузное кровотечение; д) перфорация.
17. Характер оперативного вмешательства при прободной язве желудка определяет: а) возраст больного; б) локализация перфоративного отверстия; в) степень выраженности перитонита; г) срок с момента перфорации; д) все перечисленное.
18. Для выявления типичных отдаленных метастазов рака прямой кишки используется: а) лабораторное исследование; б) пальцевое исследование прямой кишки; в) лапароскопия; г) ректороманоскопия; д) ирригоскопия.
19. При раке прямой кишки на 12 см от анального отверстия без метастазов целесообразна: а) экстирпация прямой кишки по Кеню-Майлсу; б) операция Гартмана; в) передняя резекция прямой кишки; г) наложение цекостомы; д) наложение сигмостомы.
20. Токсикоанемическая форма характерна для рака толстой кишки: а) поперечно-ободочной; б) левых отделов; в) правых отделов; г) прямой; д) сигмовидной.
21. Наиболее тяжелой формой острого парапроктита является: а) ишиоректальный; б) ретроректальный; в) подслизистый; г) пельвио-ректальный; д) подкожный.
22. Для исследования свищей прямой кишки применяются: а) наружный осмотр и пальпация; б) пальцевое исследование прямой кишки; в) прокрашивание свищевого хода и зондирование; г) фистулография; д) все перечисленное.
23. При кровотечении после дефекации в виде струйки крови и зуде в области анального отверстия можно думать: а) о параректальном свище; б) о геморрое; в) о раке прямой кишки; г) о полипе прямой кишки; д) о трещине анального канала.
24. К облигатным предракам ободочной кишки относят: а) ювенильные полипы; б) одиночный полип ободочной кишки; в) регионарный энтерит; г) терминальный илеит; д) диффузный семейный полипоз.
25. Основной гистологической формой рака толстой кишки является: а) скирр; б) перстневидноклеточный (слизистый); в) плоскоклеточный (ороговевающий); г) аденокарцинома; д) недифференцированный.
26. Больной 35 лет, поступил в клинику с диагнозом острый панкреатит. Наиболее информативным тестом является исследование: а) амилазы крови; б) трипсиногена; в) аминотрансферазы; г) альдолазы; д) лактазы.
27. Больной поступил в клинику с подозрением на острый панкреатит. Укажите наиболее информативный метод диагностики заболевания: а) целиакография; б) ультразвуковое исследование; в) лапароцентез; г) термография; д) гастродуоденоскопия.
28. Механизм лечебного действия цитостатиков при остром панкреатите: а) блокада блуждающего нерва; б) уменьшение воспаления в железе; в) уменьшение болей; г) блокада белкового синтеза в железе; д) инактивация панкреатических ферментов.
29. У больного - клиническая картина острого панкреатита, нельзя исключить прободную язву желудка. Выберите достоверный лапароскопический признак деструктивного панкреатита: а) пневматизация кишечника; б) гиперемия брюшины; в) отек большого сальника; г) наличие крови в брюшной полости; д) бляшки стеатонекроза на брюшине.
30. Признаки инкреторной недостаточности поджелудочной железы при хроническом панкреатите: а) желтуха; б) частые потери сознания; в) высокое содержание сахара в крови и моче; г) увеличение печени, пальпируемый желчный пузырь; д) креаторея, стеаторея.
31. Больной в течение 15 лет страдает хроническим панкреатитом. Укажите простейший способ обнаружения кальциноза поджелудочной железы: а) эксплоративная лапаротомия; б) лапароскопия; в) ирригоскопия; г) холангиография; д) обзорная рентгенография брюшной полости.
32. В развитии острого панкреатита главенствующая роль принадлежит: а) микробной флоре; б) плазмоцитарной инфильтрации; в) микро-циркуляторным нарушениям; г) аутоферментной агрессии; д) венозному стазу.
33. Поперечная болевая резистентность передней брюшной стенки в проекции поджелудочной железы при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Керте; в) Грея-Турнера; г) Мондора; д) Воскресенского.
34. Болезненность при пальпации в левом реберно-позвоночном углу характерна для симптома: а) Воскресенского; б) Мейо-Робсона; в) Грюнвальда; г) Мондора; д) Грея-Турнера.
35. Развитие метеоризма у больных острым панкреатитом обусловлено: а) сдавлением 12-перстной кишки отечной головкой поджелудочной железы; б) частой неукротимой рвотой; в) парезом кишечника; г) дефицитом панкреатических гормонов; д) ферментативной недостаточностью поджелудочной железы.
36. Невозможность определения пульсации брюшного отдела аорты в эпигастрии при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Мондора; в) Кера; г) Куллена; д) Воскресенского.
37. К острому панкреатиту относятся все формы, кроме: а) отечного; б) псевдотуморозного панкреатита; в) жирового панкреонекроза; г) геморрагического панкреонекроза.
38. Основным в патогенетическом лечении острого панкреатита является: а) подавление секреторной функции поджелудочной железы; б) ликвидация гиповолемии; в) инактивация панкреатических ферментов; г) назогастральная декомпрессия желудочно-кишечного тракта; д) введение цитостатиков.
39. Инвагинация относится к непроходимости: а) спастической; б) паралитической; в) обтурационной; г) странгуляционной; д) смешанной.
40. Выявление геморрагического выпота в брюшной полости и очагов жирового некроза на брюшине позволяет думать: а) о повреждении полого органа; б) о разрыве печени; в) об остром панкреатите; г) о перфоративной язве желудка; д) о мезентериальном тромбозе.
41. Наиболее ранним и постоянным симптомом острой тонкокишечной непроходимости является: а) задержка стула и газов; б) усиление перистальтики;в) схваткообразные боли в животе; г) асимметрия живота; д) рвота.
42. При узлообразовании, ущемлении кишки и завороте: а) следует проводить консервативные мероприятия по разрешению непроходимости; б) показана экстренная операция; в) предпочтительна операция в "холодном" периоде; г) необходимо динамическое наблюдение; д) все ответы не верны.
43. При острой кишечной непроходимости практически не используется лишь: а) ангиография чревной артерии; б) лабораторные исследования; в) аускультация живота; г) обзорная рентгенография брюшной полости; д) пальцевое исследование прямой кишки.
44. Для низкой толстокишечной непроходимости характерно все, кроме: а) постепенного нарастания симптомов; б) вздутия живота; в) появление чаш Клойбера; г) задержки стула; д) быстрого (в течение суток) обезвоживания.
45. При острой обтурационной толстокишечной непроходимости наблюдается все, кроме: а) схваткообразных болей в животе; б) вздутия живота; в) постепенного развития перитонита; г) постоянных болей в животе; д) задержки стула и газов.
46. Не нарушается кровообращение в брыжейке кишки при: а) завороте; б) обтурации; в) узлообразовании; г) инвагинации;д) ущемлении.
47. Консервативное лечение острой кишечной непроходимости применяется только при: а) завороте; б) узлообразовании; в).обтурационной кишечной непроходимости; г) динамической непроходимости; д) обтурации желчным камнем.
48. Толстокишечная обтурационная непроходимость чаще всего вызывается: а) инородными телами; б) желчными камнями; в) злокачественными опухолями; г) спайками брюшной полости; д) гельминтами.
49. Нижней стенкой пахового канала является: а) поперечная фасция; б) нижний край наружной косой мышцы живота; в) жимбернатова связка; г) паховая связка; д) край подвздошной кости.
50. Рихтеровским называется ущемление: а) пристеночное; б) сигмовидной кишки в скользящей грыже; в) желудка в диафрагмальной грыже; г) Меккелева дивертикула; д) червеобразного отростка.
51.Что из указанных средств и методов не следует применять при лечении гнойных ран в фазе гидратации? а) мазевые повязки; б) покой; в) антибиотикотерапию; г) промывание перекисью водорода; д) теплые марганцевые ванны.
52. Для фазы дегидратации в течении раневого процесса характерно: а) отек краев раны; б) гиперемия краев раны; в) дно раны покрыто фибрином; г) появление грануляций; д) лейкоцитарная инфильтрация тканей.
53. Лечение гнойных ран конечностей в фазе дегидратации: что не следует применять из указанного? а) витаминотерапию; б) сближение краев раны; в) повязки с гипертоническими растворами; г) переливание крови; д) повязки с мазью Вишневского.
54. Каковы оптимальные сроки для проведения первичной хирургичес-кой обработки раны? а) до 6 час; б) до 8 час; в) до 12 час; г) до 18 час; д) до 24 час.
55. Больному с AB(IV) группой крови по жизнен-ным показаниям необходимо перелить кровь. Определить резус-фактор нет ни времени, ни возможности. Какой группы и "резуса" кровь предпочтительнее при этом перелить больному? а) AB(IV) резус-положительную; б) AB(IV) резус-отрицательную; в) В(III) резус-положительную; г) А(II) резус-отрицательную; д) О(I) резус-положительную.
56. Какой из ниже перечисленных возбудителей сепсиса наиболее часто дает метастазирование? а) стрептококк; б) стафилококк; в) пневмококк; г) гонококк; д) кишечная палочка.
57. Для острого аппендицита не характерен симптом: а) Ровзинга; б) Воскресенского; в) Мерфи; г) Образцова; д) Бартомье-Михельсона.
58. К перитонеальным симптомам при остром аппендиците относят симптомы: а) Воскресенского (симптом «рубашки»); б) Щеткина-Блюмберга; в) Раздольского; г) все названные симптомы; д) ни один из них.
59. Острый аппендицит следует дифференцировать со всеми перечисленными заболеваниями, кроме: а) гломерулонефрита; б) острого панкреатита; в) острого аднексита; г) острого гастроэнтерита; д) правосторонней почечной коликой.
60. Клинически острый аппендицит может быть принят: а) за сальпингит; б) за острый холецистит; в) за дивертикулит Меккеля; г) за внематочную беременность; д) за любую из этих видов патологии.
61. Первично-гангренозный аппендицит чаще всего встречается: а) у детей; б) у лиц с тяжелой травмой; в) у мужчин; г) у женщин; д) у лиц пожилого и старческого возраста.
62. Противопоказанием к экстренной аппендэктомии является: а) аппендикулярный инфильтрат; б) инфаркт миокарда; в) вторая половина беременности; г) геморрагический диатез; д) разлитой перитонит.
63. Для диагностики острого аппендицита используются методы: а) лапароскопия; б) клинический анализ крови; в) ректальное исследование; г) термография; д) все перечисленное верно.
64. Острый холецистит обычно начинается с: а) повышения температуры; б) появления рвоты; в) болей в правом подреберье; г) расстройства стула; д) тяжести в эпигастральной области.
65. Приступ печеночной (желчной) колики возникает: а) внезапно, остро; б) после продромального периода; в) исподволь, постепенно; г) после длительного голодания; д) после переохлаждения.
66. Нормальные показатели билирубина крови: а) 0,10-0,68 мкмоль/л; б) 8,55-20,52 мкмоль/л; в) 2,50-8,33 мкмоль/л; г) 3,64-6,76 мкмоль/л; д) 7,62-12,88 мкмоль/л.
67. Ширина холедоха в норме равна: а) до 0,5; б) 0,6-1,0 см; в) 1,1-1,5 см; г) 1,6-2,0 см; д) свыше 2,0 см;
68. Больному с гангренозным холециститом показано: а) консервативное лечение; б) отсроченная операция; в) принятие решения зависит от возраста больного; г) операция при отсутствии эффекта от консервативной терапии; д) экстренная операция.
69. Больной желтухой на фоне холедохолитиаза нуждается в: а) экстренной операции; б) консервативном лечении; в) срочной операции после предоперационной подготовки; г) катетеризации чревной артерии; д) плазмоферезе.
70. К осложнениям острого калькулезного холецистита не относят: а) варикозное расширение вен пищевода; б) механическую желтуху; в) холангит; г) подпеченочный абсцесс; д) перитонит.
71. При остром калькулезном холецистите может применяться: а) экстренная операция; б) срочная операция; в) консервативная терапия и в дальнейшем плановая операция; г) только консервативная терапия; д) все перечисленное.
72. Симптом Курвуазье не характерен для: а) острого калькулезного холецистита; б) рака головки поджелудочной железы; в) индуративного панкреатита; г) опухоли большого дуоденального соска; д) опухоли холедоха.
73. Для уточнения характера желтухи и причины ее возникновения не используется: а) компьютерная томография; б) внутривенная холецистохолангиография; в) чрескожная чреспеченочная холангиография; г) эндоскопическая ретроградная панкреатохолангио-графия; д) УЗИ.
74. Наиболее оптимальный вид лечения холедохолитиаза у больных с постхолецист-эктомическим синдромом: а) эндоскопическая папилло-сфинктеротомия; б) холедохотомия; в) холедоходуоденоанастомоз; г) камнедробление; д) холедохоэнтеростомия.
75. Для подтверждения диагноза трещины анального прохода используется: а) аноскопия; б) измерение давления в прямой кишке; в) колоноскопия; г) ректоскопия; д) ирригоскопия.
76. Наиболее информативным методом инструментальной диагностики острой кишечной непроходимости является: а) обзорная рентгенография брюшной полости; б) лапароскопия; в) ангиография; г) гастроскопия; д) колоноскопия.
77. Для поздней стадии перитонита характерно все, кроме: а) вздутия живота; б) гиповолемии; в) исчезновения кишечных шумов; г) гипо-протеинемии; д) усиленной перистальтики.
78. Как устанавливается диагноз общего перитонита до операции? а) рентгенологически; б) анамнестически; в) лабораторным определением признаков воспалительной реакции; г) по клиническим признакам; д) по уровню секреции желудочного сока.
79. Эпителиальный копчиковый ход: а) связан с крестцом; б) связан с копчиком; в) оканчивается слепо в подкожной клетчатке межягодичной области; г) расположен между задней поверхностью прямой кишки и передней поверхностью крестца; д) сообщается с просветом прямой кишки.
80. Наиболее часто проявляется дисфагией рак желудка, локализующийся: а) в пилорическом отделе; б) в кардии; в) в теле желудка; г) по большой кривизне; д) в области дна.
81. Метастаз Крукенберга локализуется: а) в прямокишечно-пузырной складке; б) в пупке; в) в яичниках; г) между ножками кивательной мышцы; д) в печени.
82. Метастаз Вирхова локализуется: а) в печени; б) в прямокишечно-пузырной складке; в) в яичниках; г) между ножками кивательной мышцы; д) в легких.
83. Наиболее раннюю диагностику рака желудка обеспечивает: а) гастроскопия; б) поиск синдрома "малых признаков"; в) появление раковой триады по Мельникову; г) рентгенография желудка; д) обзорная рентгеноскопия брюшной полости.
84. Для острого пневмоторакса не характерна: а) одышка в покое; б) болевой синдром вплоть до шока; в) горизонтальный уровень жидкости в плевральной полости; г) тахикардия; д) изменение перкуторного звука.
85. Для выявления бронхоэктазов ведущее значение имеет: а) рентгенография легких; б) томография; в) бронхография; г) бронхоскопия; д) ультразвуковое исследование.
86. Наиболее частой причиной спонтанного пневмоторакса служит: а) абсцесс легкого; б) рак легкого; в) бронхоэктазы; г) буллезные кисты легкого; д) ателектаз легкого.
87. Неотложная помощь при клапанном пневмотораксе начинается: а) с дренажа плевральной полости; б) с трахеостомии; в) с блокады межреберных нервов; г) с обездвиживания грудной клетки; д) с блокады диафрагмального нерва.
88. При тампонаде сердца показана: а) пункция перикарда; б) переливание крови; в) мочегонные; г) гемостатическая терапия; д) антибиотики.
89. Проявлением тиреотоксикоза не является: а) симптом Греффе и Мебиуса; б) тахикардия; в) экзофтальм; г) тремор нижних конечностей; д) увеличение щитовидной железы.
90. К осложнениям варикозной болезни относят: а) пигментацию кожи; б) индурацию подкожной клетчатки; в) трофические язвы; г) тромбофлебит; д) слоновость.
91. Для выявления несостоятельности клапанов поверхностных вен используется проба: а) трехжгутовая (Шейниса); б) маршевая (Дельбе-Пертеса); в) Троянова-Тренделенбурга; г) Пратта; д) Тальмана.
92. При первичном варикозном расширении вен нижних конечностей показано: а) эластичное бинтование; б) хирургическое лечение; в) лечебная физкультура; г) массаж; д) рефлексотерапия.
93. Наиболее опасным осложнением тромбоза глубоких вен является: а) трофическая язва голени; б) эмболия легочной артерии; в) тромбофлебит поверхностных вен; г) облитерация глубоких вен; д) слоновость.
94. Клиническими симптомами тромбоэмболии легочной артерии являются все, кроме: а) боли за грудиной; б) коллапса; в) удушья; г) цианоза лица и верхней половины туловища; д) ослабления дыхания.
95. Наиболее точным методом диагностики тромбоэмболии легочной артерии является: а) обзорная рентгенография грудной клетки; б) ЭКГ; в) радиокардиография; г) фонокардиография; д) перфузионное сканирование легких.
96. Сущность пробы Оппеля состоит в: а) утомлении ног; б) реактивной гиперемии; в) побледнении подошвенной поверхности стопы; г) побледнении пальцев; д) боли в икроножных мышцах.
97. Синдром Лериша может быть причиной тромбоза: а) бедренной артерии; б) подколенной артерии; в) бифуркации аорты и подвздошной артерии; г) почечных артерий; д) тромбоэмболии легочной артерии.
98. Наиболее частой причиной острого артериального тромбоза является: а) облитерирующий тромбангиит; б) облитерирующий атеросклероз; в) пункция и катетеризация артерий; г) экстравазальная компрессия артерий; д) полицитемия.
99. Для острой артериальной недостаточности конечностей не характерно: а) отсутствие пульса; б) парастезии; в) трофические язвы голени; г) паралич конечностей; д) бледность кожи и боли.
100. При быстро прогрессирующей гангрене стопы необходимо: а) сделать множественные разрезы кожи стопы; б) срочно выполнить ампутацию; в) произвести шунтирование артерий; г) пытаться перевести влажную гангрену в сухую; д) проводить массивную антибиотикотерапию.
Вариант 4
1. Для подтверждения диагноза трещины анального прохода используется: а) аноскопия; б) измерение давления в прямой кишке; в) колоноскопия; г) ректоскопия; д) ирригоскопия.
2. Наиболее информативным методом инструментальной диагностики острой кишечной непроходимости является: а) обзорная рентгенография брюшной полости; б) лапароскопия; в) ангиография; г) гастроскопия; д) колоноскопия.
3. Для поздней стадии перитонита характерно все, кроме: а) вздутия живота; б) гиповолемии; в) исчезновения кишечных шумов; г) гипопротеинемии; д) усиленной перистальтики.
4. Как устанавливается диагноз общего перитонита до операции? а) рентгенологически; б) анамнестически; в) лабораторным определением признаков воспалительной реакции; г) по клиническим признакам; д) по уровню секреции желудочного сока.
5. Эпителиальный копчиковый ход: а) связан с крестцом; б) связан с копчиком; в) оканчивается слепо в подкожной клетчатке межягодичной области; г) расположен между задней поверхностью прямой кишки и передней поверхностью крестца; д) сообщается с просветом прямой кишки.
6. Наиболее часто проявляется дисфагией рак желудка, локализующийся: а) в пилорическом отделе; б) в кардии; в) в теле желудка; г) по большой кривизне; д) в области дна.
7. Метастаз Крукенберга локализуется: а) в прямокишечно-пузырной складке; б) в пупке; в) в яичниках; г) между ножками кивательной мышцы; д) в печени.
8. Метастаз Вирхова локализуется: а) в печени; б) в прямокишечно-пузырной складке; в) в яичниках; г) между ножками кивательной мышцы; д) в легких.
9. Наиболее раннюю диагностику рака желудка обеспечивает: а) гастроскопия; б) поиск синдрома "малых признаков"; в) появление раковой триады по Мельникову; г) рентгенография желудка; д) обзорная рентгеноскопия брюшной полости.
10. Для острого пневмоторакса не характерна: а) одышка в покое; б) болевой синдром вплоть до шока; в) горизонтальный уровень жидкости в плевральной полости; г) тахикардия; д) изменение перкуторного звука.
11. Для выявления бронхоэктазов ведущее значение имеет: а) рентгенография легких; б) томография; в) бронхография; г) бронхоскопия; д) ультразвуковое исследование.
12. Наиболее частой причиной спонтанного пневмоторакса служит: а) абсцесс легкого; б) рак легкого; в) бронхоэктазы; г) буллезные кисты легкого; д) ателектаз легкого.
13. Неотложная помощь при клапанном пневмотораксе начинается: а) с дренажа плевральной полости; б) с трахеостомии; в) с блокады межреберных нервов; г) с обездвиживания грудной клетки; д) с блокады диафрагмального нерва.
14. При тампонаде сердца показана: а) пункция перикарда; б) переливание крови; в) мочегонные; г) гемостатическая терапия; д) антибиотики.
15. Проявлением тиреотоксикоза не является: а) симптом Греффе и Мебиуса; б) тахикардия; в) экзофтальм; г) тремор нижних конечностей; д) увеличение щитовидной железы.
16. К осложнениям варикозной болезни относят: а) пигментацию кожи; б) индурацию подкожной клетчатки; в) трофические язвы; г) тромбофлебит; д) слоновость.
17. Для выявления несостоятельности клапанов поверхностных вен используется проба: а) трехжгутовая (Шейниса); б) маршевая (Дельбе-Пертеса); в) Троянова-Тренделенбурга; г) Пратта; д) Тальмана.
18. При первичном варикозном расширении вен нижних конечностей показано: а) эластичное бинтование; б) хирургическое лечение; в) лечебная физкультура; г) массаж; д) рефлексотерапия.
19. Наиболее опасным осложнением тромбоза глубоких вен является: а) трофическая язва голени; б) эмболия легочной артерии; в) тромбофлебит поверхностных вен; г) облитерация глубоких вен; д) слоновость.
20. Клиническими симптомами тромбоэмболии легочной артерии являются все, кроме: а) боли за грудиной; б) коллапса; в) удушья; г) цианоза лица и верхней половины туловища; д) ослабления дыхания.
21. Наиболее точным методом диагностики тромбоэмболии легочной артерии является: а) обзорная рентгенография грудной клетки; б) ЭКГ; в) радиокардиография; г) фонокардиография; д) перфузионное сканирование легких.
22. Сущность пробы Оппеля состоит в: а) утомлении ног; б) реактивной гиперемии; в) побледнении подошвенной поверхности стопы; г) побледнении пальцев; д) боли в икроножных мышцах.
23. Синдром Лериша может быть причиной тромбоза: а) бедренной артерии; б) подколенной артерии; в) бифуркации аорты и подвздошной артерии; г) почечных артерий; д) тромбоэмболии легочной артерии.
24. Наиболее частой причиной острого артериального тромбоза является: а) облитерирующий тромбангиит; б) облитерирующий атеросклероз; в) пункция и катетеризация артерий; г) экстравазальная компрессия артерий; л) полицитемия.
25. Для острой артериальной недостаточности конечностей не характерно: а) отсутствие пульса; б) парастезии; в) трофические язвы голени; г) паралич конечностей; д) бледность кожи и боли.
26. При быстро прогрессирующей гангрене стопы необходимо: а) сделать множественные разрезы кожи стопы; б) срочно выполнить ампутацию; в) произвести шунтирование артерий; г) пытаться перевести влажную гангрену в сухую; д) проводить массивную антибиотикотерапию.
27. Пахово-мошоночную грыжу дифференцируют со всем, кроме: а) варикоцеле; б) опухоли семенного канатика; в) опухоли яичка; г) гидроцеле; д) аневризмы v. saphena magna.
28. При ущемленной абдоминальной грыже независимо от состояния больного показано: а) спазмолитики и теплая ванна; б) наблюдение; в) антибиотики и строгий постельный режим; г) обзорная рентгенография брюшной полости; д) экстренная операция.
29. О чем говорит тимпанический звук при перкуссии грыжевого выпячивания? а) о водянке яичка; б) о наличии петли кишки; в) о лимфадените; г) об опухоли; д) об изменениях в семенном канатике.
30. При ущемлении грыжи у больного с острым инфарктом миокарда показано: а) наблюдение, холод на живот; б) вправление грыжи; в) введение спазмолитиков; г) положение Тренделенбурга; д) экстренная операция.
31. Наличие яичка в грыжевом мешке характерно для грыжи: а) скользящей; б) ущемленной; в) бедренной; г) врожденной; д) косой паховой.
32. Прямую паховую грыжу характеризует слабость стенки: а) задней; б) верхней; в) передней; г) нижней; д) всех стенок.
33. Грыжевой мешок врожденной грыжи образован: а) париетальной брюшиной; б) брыжейкой кишки; в) влагалищным отростком брюшины; г) висцеральной брюшиной; д) поперечной фасцией;
34. Больному с ущемленной грыжей перед операцией проводят: а) паранефральную блокаду; б) очистительную клизму; в) блокаду семенного канатика; г) бритье области операции; д) промывание желудка.
35. При флегмоне грыжевого мешка операцию начинают: а) с вскрытия флегмоны; б) со срединной лапаротомии; в) с выделения грыжевого мешка из окружающих тканей; г) с пункции грыжевого мешка; д) с одновременной операции из двух доступов.
36. Этиопатогенетически обоснованным методом операции при неосложненной дуоденальной язве является: а) селективная проксимальная ваготомия; б) идеальная антрумэктомия; в) сочетание антрумэктомии с ваготомией; г) высокая (2/3 и более) резекция желудка; д) стволовая или селективная ваготомия.
37. Наиболее частым осложнением язвы передней стенки 12-перстной кишки является: а) перфорация; б) кровотечение; в) пенетрация в головку поджелудочной железы; г) малигнизация; д) все неверно.
38. Крайне редким осложнением язвы 12-перстной кишки является: а) перфорация; б) малигнизация; в) кровотечение; г) пенетрация; д) рубцовая деформация кишки.
39. Достоверным рентгенологическим признаком перфорации гастродуоденальной язвы является: а) высокое стояние диафрагмы; б) наличие свободного газа в брюшной полости; в) пневматизация кишечника; г) "чаши" Клойбера; д) увеличенный газовый пузырь желудка.
40. Срыгивание пенистой кровью ярко-красного цвета, усиливающееся при кашле, характерно для: а) кровоточащей язвы желудка; б) опухоли кардии; в) синдрома Маллори-Вейсса; г) легочного кровотечения; д) синдрома Рандю-Ослера.
41. Для перфоративной гастродуоденальной язвы характерно: а) внезапное начало с резких болей в эпигастрии; б) постепенное нарастание болевого синдрома; в) схваткообразные резкие боли; г) обильная многократная рвота; д) быстро нарастающая слабость, головокружение.
42. Наиболее частым осложнением пенетрирующей язвы желудка является: а) развитие стеноза привратника; б) малигнизация язвы; в) образование межорганного свища; г) профузное кровотечение; д) перфорация.
43. Характер оперативного вмешательства при прободной язве желудка определяет: а) возраст больного; б) локализация перфоративного отверстия; в) степень выраженности перитонита; г) срок с момента перфорации; д) все перечисленное.
44. Для выявления типичных отдаленных метастазов рака прямой кишки используется: а) лабораторное исследование; б) пальцевое исследование прямой кишки; в) лапароскопия; г) ректороманоскопия; д) ирригоскопия.
45. При раке прямой кишки на 12 см от анального отверстия без метастазов целесообразна: а) экстирпация прямой кишки по Кеню-Майлсу; б) операция Гартмана; в) передняя резекция прямой кишки; г) наложение цекостомы; д) наложение сигмостомы.
46. Токсикоанемическая форма характерна для рака толстой кишки: а) поперечно-ободочной; б) левых отделов; в) правых отделов; г) прямой; д) сигмовидной.
47. Наиболее тяжелой формой острого парапроктита является: а) ишиоректальный; б) ретроректальный; в) подслизистый; г) пельвио-ректальный; д) подкожный.
48. Для исследования свищей прямой кишки применяются: а) наружный осмотр и пальпация; б) пальцевое исследование прямой кишки; в) прокрашивание свищевого хода и зондирование; г) фистулография; д) все перечисленное.
49. При кровотечении после дефекации в виде струйки крови и зуде в области анального отверстия можно думать: а) о параректальном свище; б) о геморрое; в) о раке прямой кишки; г) о полипе прямой кишки; д) о трещине анального канала.
50. К облигатным предракам ободочной кишки относят: а) ювенильные полипы; б) одиночный полип ободочной кишки; в) регионарный энтерит; г) терминальный илеит; д) диффузный семейный полипоз.
51. Основной гистологической формой рака толстой кишки является: а) скирр; б) перстневидноклеточный (слизистый); в) плоскоклеточный (ороговевающий); г) аденокарцинома; д) недифференцированный.
52. Больной 35 лет, поступил в клинику с диагнозом острый панкреатит. Наиболее информативным тестом является исследование: а) амилазы крови; б) трипсиногена; в) аминотрансферазы; г) альдолазы; д) лактазы.
53. Больной поступил в клинику с подозрением на острый панкреатит. Укажите наиболее информативный метод диагностики заболевания: а) целиакография; б) ультразвуковое исследование; в) лапароцентез; г) термо-графия; д) гастродуоденоскопия.
54. Механизм лечебного действия цитостатиков при остром панкреатите: а) блокада блуждающего нерва; б) уменьшение воспаления в железе; в) уменьшение болей; г) блокада белкового синтеза в железе; д) инактивация панкреатических ферментов.
55. У больного - клиническая картина острого панкреатита, нельзя исключить прободную язву желудка. Выберите достоверный лапароскопический признак деструктивного панкреатита: а) пневматизация кишечника; б) гиперемия брюшины; в) отек большого сальника; г) наличие крови в брюшной полости; д) бляшки стеатонекроза на брюшине.
56. Признаки инкреторной недостаточности поджелудочной железы при хроническом панкреатите: а) желтуха; б) частые потери сознания; в) высокое содержание сахара в крови и моче; г) увеличение печени, пальпируемый желчный пузырь; д) креаторея, стеаторея.
57. Больной в течение 15 лет страдает хроническим панкреатитом. Укажите простейший способ обнаружения кальциноза поджелудочной железы: а) эксплоративная лапаротомия; б) лапароскопия; в) ирригоскопия; г) холангиография; д) обзорная рентгенография брюшной полости.
58. В развитии острого панкреатита главенствующая роль принадлежит: а) микробной флоре; б) плазмоцитарной инфильтрации; в) микро-циркуляторным нарушениям; г) аутоферментной агрессии; д) венозному стазу.
59. Поперечная болевая резистентность передней брюшной стенки в проекции поджелудочной железы при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Керте; в) Грея-Турнера; г) Мондора; д) Воскресенского.
60. Болезненность при пальпации в левом реберно-позвоночном углу характерна для симптома: а) Воскресенского; б) Мейо-Робсона; в) Грюнвальда; г) Мондора; д) Грея-Турнера.
61. Развитие метеоризма у больных острым панкреатитом обусловлено: а) сдавлением 12-перстной кишки отечной головкой поджелудочной железы; б) частой неукротимой рвотой; в) парезом кишечника; г) дефицитом панкреатических гормонов; д) ферментативной недостаточностью поджелудочной железы.
62. Невозможность определения пульсации брюшного отдела аорты в эпигастрии при остром панкреатите носит название симптома: а) Мейо-Робсона; б) Мондора; в) Кера; г) Куллена; д) Воскресенского.
63. К острому панкреатиту относятся все формы, кроме: а) отечного; б) псевдотуморозного панкреатита; в) жирового панкреонекроза; г) геморрагического панкреонекроза.
64. Основным в патогенетическом лечении острого панкреатита является: а) подавление секреторной функции поджелудочной железы; б) ликвидация гиповолемии; в) инактивация панкреатических ферментов; г) назогастральная декомпрессия желудочно-кишечного тракта; д) введение цитостатиков.
65. Инвагинация относится к непроходимости: а) спастической; б) паралитической; в) обтурационной; г) странгуляционной; д) смешанной.
66. Выявление геморрагического выпота в брюшной полости и очагов жирового некроза на брюшине позволяет думать: а) о повреждении полого органа; б) о разрыве печени; в) об остром панкреатите; г) о перфоративной язве желудка; д) о мезентериальном тромбозе.
67. Наиболее ранним и постоянным симптомом острой тонкокишечной непроходимости является: а) задержка стула и газов; б) усиление перистальтики;в) схваткообразные боли в животе; г) асимметрия живота; д) рвота.
68. При узлообразовании, ущемлении кишки и завороте: а) следует проводить консервативные мероприятия по разрешению непроходимости; б) показана экстренная операция; в) предпочтительна операция в "холодном" периоде; г) необходимо динамическое наблюдение; д) все ответы не верны.
69. При острой кишечной непроходимости практически не используется лишь: а) ангиография чревной артерии; б) лабораторные исследования; в) аускультация живота; г) обзорная рентгенография брюшной полости; д) пальцевое исследование прямой кишки.
70. Для низкой толстокишечной непроходимости характерно все, кроме: а) постепенного нарастания симптомов; б) вздутия живота; в) появление чаш Клойбера; г) задержки стула; д) быстрого (в течение суток) обезвоживания.
71. При острой обтурационной толстокишечной непроходимости наблюдается все, кроме: а) схваткообразных болей в животе; б) вздутия живота; в) постепенного развития перитонита; г) постоянных болей в животе; д) задержки стула и газов.
72. Не нарушается кровообращение в брыжейке кишки при: а) завороте; б) обтурации; в) узлообразовании; г) инвагинации;д) ущемлении.
73. Консервативное лечение острой кишечной непроходимости применяется только при: а) завороте; б) узлообразовании; в).обтурационной кишечной непроходимости; г) динамической непроходимости; д) обтурации желчным камнем.
74. Толстокишечная обтурационная непроходимость чаще всего вызывается: а) инородными телами; б) желчными камнями; в) злокачественными опухолями; г) спайками брюшной полости; д) гельминтами.
75. Нижней стенкой пахового канала является: а) поперечная фасция; б) нижний край наружной косой мышцы живота; в) жимбернатова связка; г) паховая связка; д) край подвздошной кости.
76. Рихтеровским называется ущемление: а) пристеночное; б) сигмовидной кишки в скользящей грыже; в) желудка в диафрагмальной грыже; г) Меккелева дивертикула; д) червеобразного отростка.
77.Что из указанных средств и методов не следует применять при лечении гнойных ран в фазе гидратации? а) мазевые повязки; б) покой; в) антибиотикотерапию; г) промывание перекисью водорода; д) теплые марганцевые ванны.
78. Для фазы дегидратации в течении раневого процесса характерно:
а) отек краев раны; б) гиперемия краев раны; в) дно раны покрыто фибрином;
г) появление грануляций; д) лейкоцитарная инфильтрация тканей.
79. Лечение гнойных ран конечностей в фазе дегидратации: что не следует применять из указанного? а) витаминотерапию; б) сближение краев раны; в) повязки с гипертоническими растворами; г) переливание крови; д) повязки с мазью Вишневского.
80. Каковы оптимальные сроки для проведения первичной хирургической обработки раны? а) до 6 час; б) до 8 час; в) до 12 час; г) до 18 час; д) до 24 час.
81. Больному с AB(IV) группой крови по жизненным показаниям необходимо перелить кровь. Определить резус-фактор нет ни времени, ни возможности. Какой группы и "резуса" кровь предпочтительнее при этом перелить больному? а) AB(IV) резус-положительную; б) AB(IV) резус-отрицательную; в) В(III) резус-положительную; г) А(II) резус-отрицательную; д) О(I) резус-положительную.
82. Какой из ниже перечисленных возбудителей сепсиса наиболее часто дает метастазирование? а) стрептококк; б) стафилококк; в) пневмококк; г) гонококк; д) кишечная палочка.
83. Для острого аппендицита не характерен симптом: а) Ровзинга; б) Воскресенского; в) Мерфи; г) Образцова; д) Бартомье-Михельсона.
84. К перитонеальным симптомам при остром аппендиците относят симптомы: а) Воскресенского (симптом «рубашки»); б) Щеткина-Блюмберга; в) Раздольского; г) все названные симптомы; д) ни один из них.
85. Острый аппендицит следует дифференцировать со всеми перечисленными заболеваниями, кроме: а) гломерулонефрита; б) острого панкреатита; в) острого аднексита; г) острого гастроэнтерита; д) право-сторонней почечной коликой.
86. Клинически острый аппендицит может быть принят: а) за сальпингит; б) за острый холецистит; в) за дивертикулит Меккеля; г) за внематочную беременность; д) за любую из этих видов патологии.
87. Первично-гангренозный аппендицит чаще всего встречается: а) у детей; б) у лиц с тяжелой травмой; в) у мужчин; г) у женщин; д) у лиц пожилого и старческого возраста.
88. Противопоказанием к экстренной аппендэктомии является: а) аппендикулярный инфильтрат; б) инфаркт миокарда; в) вторая половина беременности; г) геморрагический диатез; д) разлитой перитонит.
89. Для диагностики острого аппендицита используются методы: а) лапароскопия; б) клинический анализ крови; в) ректальное исследование; г) термография; д) все перечисленное верно.
90. Острый холецистит обычно начинается с: а) повышения температуры; б) появления рвоты; в) болей в правом подреберье; г) расстройства стула; д) тяжести в эпигастральной области.
91. Приступ печеночной (желчной) колики возникает: а) внезапно, остро; б) после продромального периода; в) исподволь, постепенно; г) после длительного голодания; д) после переохлаждения.
92. Нормальные показатели билирубина крови: а) 0,10-0,68 мкмоль/л; б) 8,55-20,52 мкмоль/л; в) 2,50-8,33 мкмоль/л; г) 3,64-6,76 мкмоль/л; д) 7,62-12,88 мкмоль/л.
93. Ширина холедоха в норме равна: а) до 0,5; б) 0,6-1,0 см; в) 1,1-1,5 см; г) 1,6-2,0 см; д) свыше 2,0 см;
94. Больному с гангренозным холециститом показано: а) консервативное лечение; б) отсроченная операция; в) принятие решения зависит от возраста больного; г) операция при отсутствии эффекта от консервативной терапии; д) экстренная операция.
95. Больной желтухой на фоне холедохолитиаза нуждается в: а) экстренной операции; б) консервативном лечении; в) срочной операции после предоперационной подготовки; г) катетеризации чревной артерии; д) плазмоферезе.
96. К осложнениям острого калькулезного холецистита не относят: а) варикозное расширение вен пищевода; б) механическую желтуху; в) холангит; г) подпеченочный абсцесс; д) перитонит.
97. При остром калькулезном холецистите может применяться: а) экстренная операция; б) срочная операция; в) консервативная терапия и в дальнейшем плановая операция; г) только консервативная терапия; д) все перечисленное.
98. Симптом Курвуазье не характерен для: а) острого калькулезного холецистита; б) рака головки поджелудочной железы; в) индуративного панкреатита; г) опухоли большого дуоденального соска; д) опухоли холедоха.
99. Для уточнения характера желтухи и причины ее возникновения не используется: а) компьютерная томография; б) внутривенная холецистохолангиография; в) чрескожная чреспеченочная холангиография; г) эндоскопическая ретроградная панкреатохолангио-графия; д) УЗИ.
100. Наиболее оптимальный вид лечения холедохолитиаза у больных с постхолецистэктомическим синдромом: а) эндоскопическая папилло-сфинктеротомия; б) холедохотомия; в) холедоходуоденоанастомоз; г) камне-дробление; д) холедохоэнтеростомия.
О Т В Е Т Ы – ВАРИАНТ «1»
Вопрос |
Ответ |
1 |
а |
2 |
г |
3 |
в |
4 |
а |
5 |
б |
6 |
б |
7 |
в |
8 |
г |
9 |
а |
10 |
д |
11 |
д |
12 |
а |
13 |
д |
14 |
в |
15 |
а |
16 |
б |
17 |
б |
18 |
д |
19 |
в |
20 |
а |
21 |
д |
22 |
а |
23 |
б |
24 |
а |
25 |
а |
Вопрос |
Ответ |
26 |
б |
27 |
г |
28 |
д |
29 |
в |
30 |
д |
31 |
г |
32 |
б |
33 |
б |
34 |
в |
35 |
д |
36 |
б |
37 |
а |
38 |
д |
39 |
в |
40 |
в |
41 |
б |
42 |
а |
43 |
д |
44 |
г |
45 |
б |
46 |
г |
47 |
в |
48 |
г |
49 |
а |
50 |
д |
Вопрос |
Ответ |
51 |
д |
52 |
б |
53 |
д |
54 |
г |
55 |
а |
56 |
в |
57 |
г |
58 |
б |
59 |
а |
60 |
а |
61 |
б |
62 |
б |
63 |
г |
64 |
а |
65 |
г |
66 |
д |
67 |
в |
68 |
в |
69 |
в |
70 |
г |
71 |
д |
72 |
б |
73 |
д |
74 |
г |
75 |
а |
Вопрос |
Ответ |
76 |
а |
77 |
д |
78 |
г |
79 |
в |
80 |
б |
81 |
в |
82 |
г |
83 |
а |
84 |
в |
85 |
в |
86 |
г |
87 |
а |
88 |
а |
89 |
д |
90 |
г |
91 |
в |
92 |
б |
93 |
б |
94 |
д |
95 |
д |
96 |
в |
97 |
в |
98 |
б |
99 |
в |
100 |
б |
О Т В Е Т Ы – ВАРИАНТ «2»
Вопрос |
Ответ |
1 |
а |
2 |
б |
3 |
г |
4 |
д |
5 |
в |
6 |
д |
7 |
г |
8 |
б |
9 |
б |
10 |
в |
11 |
д |
12 |
б |
13 |
а |
14 |
д |
15 |
в |
16 |
в |
17 |
б |
18 |
а |
19 |
д |
20 |
г |
21 |
б |
22 |
г |
23 |
в |
24 |
г |
25 |
а |
Вопрос |
Ответ |
26 |
а |
27 |
д |
28 |
г |
29 |
в |
30 |
б |
31 |
в |
32 |
г |
33 |
а |
34 |
в |
35 |
в |
36 |
г |
37 |
а |
38 |
а |
39 |
д |
40 |
г |
41 |
в |
42 |
б |
43 |
б |
44 |
д |
45 |
д |
46 |
в |
47 |
в |
48 |
б |
49 |
в |
50 |
б |
Вопрос |
Ответ |
51 |
д |
52 |
д |
53 |
б |
54 |
д |
55 |
г |
56 |
а |
57 |
в |
58 |
г |
59 |
б |
60 |
а |
61 |
а |
62 |
б |
63 |
б |
64 |
г |
65 |
а |
66 |
г |
67 |
д |
68 |
в |
69 |
в |
70 |
в |
71 |
г |
72 |
д |
73 |
б |
74 |
д |
75 |
г |
Вопрос |
Ответ |
76 |
а |
77 |
а |
78 |
г |
79 |
в |
80 |
а |
81 |
б |
82 |
б |
83 |
в |
84 |
г |
85 |
а |
86 |
д |
87 |
д |
88 |
а |
89 |
д |
90 |
в |
91 |
а |
92 |
б |
93 |
б |
94 |
д |
95 |
в |
96 |
а |
97 |
д |
98 |
а |
99 |
б |
100 |
а |
О Т В Е Т Ы – ВАРИАНТ «3»
Вопрос |
Ответ |
1 |
д |
2 |
д |
3 |
б |
4 |
д |
5 |
г |
6 |
а |
7 |
в |
8 |
г |
9 |
б |
10 |
а |
11 |
а |
12 |
б |
13 |
б |
14 |
г |
15 |
а |
16 |
г |
17 |
д |
18 |
в |
19 |
в |
20 |
в |
21 |
г |
22 |
д |
23 |
б |
24 |
д |
25 |
г |
Вопрос |
Ответ |
26 |
а |
27 |
б |
28 |
г |
29 |
д |
30 |
в |
31 |
д |
32 |
г |
33 |
б |
34 |
б |
35 |
в |
36 |
д |
37 |
б |
38 |
а |
39 |
д |
40 |
в |
41 |
в |
42 |
б |
43 |
а |
44 |
д |
45 |
г |
46 |
б |
47 |
г |
48 |
в |
49 |
г |
50 |
а |
Вопрос |
Ответ |
51 |
а |
52 |
г |
53 |
в |
54 |
а |
55 |
б |
56 |
б |
57 |
в |
58 |
г |
59 |
а |
60 |
д |
61 |
д |
62 |
а |
63 |
д |
64 |
в |
65 |
а |
66 |
б |
67 |
б |
68 |
д |
69 |
в |
70 |
а |
71 |
д |
72 |
а |
73 |
б |
74 |
а |
75 |
а |
Вопрос |
Ответ |
76 |
а |
77 |
д |
78 |
г |
79 |
в |
80 |
б |
81 |
в |
82 |
г |
83 |
а |
84 |
в |
85 |
в |
86 |
г |
87 |
а |
88 |
а |
89 |
д |
90 |
г |
91 |
в |
92 |
б |
93 |
б |
94 |
д |
95 |
д |
96 |
в |
97 |
в |
98 |
б |
99 |
в |
100 |
б |
О Т В Е Т Ы – ВАРИАНТ «4»
Вопрос |
Ответ |
1 |
а |
2 |
а |
3 |
д |
4 |
г |
5 |
в |
6 |
б |
7 |
в |
8 |
г |
9 |
а |
10 |
в |
11 |
в |
12 |
г |
13 |
а |
14 |
а |
15 |
д |
16 |
г |
17 |
в |
18 |
б |
19 |
б |
20 |
д |
21 |
д |
22 |
в |
23 |
в |
24 |
б |
25 |
в |
Вопрос |
Ответ |
26 |
б |
27 |
д |
28 |
д |
29 |
б |
30 |
д |
31 |
г |
32 |
а |
33 |
в |
34 |
г |
35 |
б |
36 |
а |
37 |
а |
38 |
б |
39 |
б |
40 |
г |
41 |
а |
42 |
г |
43 |
д |
44 |
в |
45 |
в |
46 |
в |
47 |
г |
48 |
д |
49 |
б |
50 |
д |
Вопрос |
Ответ |
51 |
г |
52 |
а |
53 |
б |
54 |
г |
55 |
д |
56 |
в |
57 |
д |
58 |
г |
59 |
б |
60 |
б |
61 |
в |
62 |
д |
63 |
б |
64 |
а |
65 |
д |
66 |
в |
67 |
в |
68 |
б |
69 |
а |
70 |
д |
71 |
г |
72 |
б |
73 |
г |
74 |
в |
75 |
г |
Вопрос |
Ответ |
|
76 |
а |
|
77 |
а |
|
78 |
г |
|
79 |
в |
|
80 |
а |
|
81 |
б |
|
82 |
б |
|
83 |
в |
|
84 |
г |
|
85 |
а |
|
86 |
д |
|
87 |
д |
|
88 |
а |
|
89 |
д |
|
90 |
в |
|
91 |
а |
|
92 |
б |
|
93 |
б |
|
94 |
д |
|
95 |
в |
|
96 |
а |
|
97 |
д |
|
98 |
а |
|
99 |
б |
|
100 |
а |
|
Тестовые задания для итогового контроля (факультет иностранных студентов)
Complication of bilateral lumbar sympathectomy -
Retro grade ejaculation
Inability to sustain an erectin
Dry ejaculation
Dribbling micturition
Commonest cause of abdominal aortic aneurysm -
Atherosclerosis
Marfan's syndrome
Thrombosis
Endocarditis
Management of a cause of iliac artery embolism requires-
Embolectomy
Injection of vasodilators
Hypotensive therapy
Sympathectomy
Treatment of acute femoral embolus is –
Warfarin
Heparin
Immediate embolectomy
Embolectomy after 5 days bed rest
The sequence of symptoms in pulmonary embolism is-
Fever, pain, dyspnoea
Fever, dyspnoea
Dyspnoea, pain, haemoptysis
Dyspnoea, cough, purulent sputum
If a patients known to have an abdomial aortic aneurysm complains of severe back pain it usually means –
Associated pancreatitis
Pressure on spinal cord
Impending rupture
Englargement of sac
Earliest sign of deep vein thrombosis is-
Calf tenderness
Rise in temperature
Swelling of calf muscle
Roman's sign
Best method for diagnosis of deep vein thrombosis is –
Doppler examination
Plethysmography
Contrast phlebography
I 131 Fibrinogen studies
Investigation of choice for diagnosis of deep vein thrombosis –
Venogram
Doppler
Isotope scan
Homans sign
What is acceptable in the management of femoral vein thrombosis -
Bed rest and spiral elastic bandages
A venogram
Thrombectomy
Embolectomy
A mobin udin umbrella inserted into the vein
Brodie -Trendlenburg test demonstrates-
Mid - thigh perforation
Deep vein thrombosis
Sapheno — femoral incompetence
Calf perforators
Complications of Meckel's diverticulum include-
Hemorrhage
Intussusception
Strangulation
All are correct
Ulcerative colitis almost always involves the ... -
Caecum
Sigmoid
Right colon
Rectum
The following is true of mesentric artery thrombosis-
Mostely embolic in nature
Shock is present
Extensive infarction of whole of small bowel and cecum is seen
Good prognosis
Commonest site of diverticulosis is … colon -
Ascending
Transverse
Sigmoid
Descending
The commonest presentation of meckel's diverticulum is -
Bleeding
Obstruction
Diveticulitis
Intussception
Most common indication for laparotomy in intestine a) Peritonitis
b) Intestinal obstruction
c) Doubtful diagnosis
d) Lower GI bleeding
The best investigation for colorectal carcinoma -
Exfoliative cytology
Air contrast barium enema
Ultrasound
Colonoscopy and biopsy
True about carcinoma colon is -
Left side present with anemia
Solitary liver metastasis is not a contraindication to surgery
Most common site is ascending colon
Right side are usually stenosing variety
Treatment of pouch of Douglas abscess is -
Laparotomy
Posterior colpotomy
Antibiotics
Extraperitoneal drainage
Commonest site of primary of Kurkenberg tumour is-
Breast
Colon
Stomach
Small intestine
Gas most suited for laproscopy is -
Air
Nitrogen
CO
Oxygen
Carbon dioxide
Least irritant fluid to peritoneum -
Blood
Urine
Bile
Pancreatic fluid
The commonest organism seen in peritonitis is -
Escherichia coli
Clostridium welchii
Staphylococci
Klebsiella
Hemobilia is characterised by -
Jaundice
Biliary colic
Malena
Fever
A gall stone gets impacted most commonly in which part of common bile duct -
Supraduodenal
Retroduodenal
Ampulla of vater
Common hepatic duct
Best diagnostic tool in obstructive jaundice is -
ERCP
Ultrasound
PTC
Blood tests
Klatskin tumour is tumour -
At the juncture of cystic duct and bile duct
At bile duct
At ampulla of vater
At the junction of the bile duct
Investigation of choice of case of obstructive jaundice
USG
Plain X-ray
CT scan
ERCP
Laparoscopic cholecystectomy is best avoided in patient with -
Hypertension
Diabetes
Obesity
COPD (chronic obstructive pulmonary disease)
Meckel's diverticulum is -
Ductus venosus
Vitello intestinal duct
Left umbilical vein
Obliterated umbilical artery
Commonest type of hernia is -
Femoral
Inguinal
Ventral
Epigastric
Hiatus
Causes of recurrent hernia -
Absorbable sutures
Sliding hernia
Missed sac
Infection
Strangulation is most common with which hernia -
Femoral
Inguinal
Obturator
Epigastric
Ventral hernia is a/an -
Incisional hernia
Umbilical hernia
Femoral hernia
Inguinal hernia
Mayo's operation is done for -
Spigelian hernia
Femoral hernia
Richer's hernia
Umbilical hernia
Carcinoma stomach is associated with blood group
A
B
AB
O
Commonest site of peptic ulcer perforation -
Anterior aspect of the first part of duodenum
Posterior aspect of the 1st part of duodenum
Greater cuvature of the stomach
Lesser curvature of the stomach
Anterior apect of 2nd of duodenum
Barium meal picture of carcinoma stomach is -
Filling defect
Loss of rugosity
Small capacity of stomach
Delayed emptying of barium
All
Haemorrhage from a bleeding duodenal ulcer is due to the erosion of........ artery –
Superior pancreatic duodenal
Gastroduodenal
Right gastric
Left gastric
In pyloric stenosis the following changes occur-
Hypokalemic hyponatremic alkalosis
Hyperkalaemia
Acidosis with hyponartremic alkalosis
Hyperchloremic acidosis
The treatment of peptic ulcer involves -
Antacids
Ranitidine
Sucralfate
All
Anemia is greater in which of the following gastric resection-
BillRoth II
BillRoth I
Both of the above are equal
Neither of the above
The treatment of choice of hypertropnic pyloric stenosis of adults is –
Pyloromytomy
Pyloroplasty
Billroth I gastrectomy
Highly selective vagotomy
Investigation of choice in peptic ulcer perforation is
USG
X-Ray abdomen
Paracentasis
CTscan
All of following may be associated with peptic ulcer
Alcoholic cirrhosis
Zollinger ellison syndrome
Plummer vinson syndrome
Primary Hyperparathyrodism
Investigation of choice for an early gastric carcinoma-
Endoscopic ultrasound
Stained endoscopic biopsy
Barium meal
CT scan
Dumping syndrome occurs due to –
Small stomach
Hyperosmolar load in intestine
Vagolytic action
Excesive intake of food
Earliest symptoms of carcinoma rectum-
Pain
Alteration of bowel habits
Bleeding PR
Tenesmus
Anterior resection is contra indicated in the following-
Age more than 60 years)
Undifferentiated carcinoma
Melanin in liver
Cancer is less than 5 cm from anorectal margin
Distal clearance in surgery for carcinoma rectum is-
2 cm
5 cm
10 cm
8cm
Treatment of carcinoma rectum 5 cm from anal verge without nodal metastasis is -
Abdominoperineal resection
Radiotherapy
Endoscopic resection
Chemotherapy
Rectal polyps usually present with -
Obstruction
Perforation
Bleeding
Malignant change
Appendicular artery is a branch of :
ilieocolic artery
Right colic artery
Middle colic artery
Posterior cecal artery
Earliest symptoms in acute appendicitis is -
Pain
Fever
Vomiting
Rise of pulse rate
Commonest position of the appendix -
Retrocaecal
Preileal
Postileal
Pelvic
Subcaecal
Oschner sherren regime is used in management of-
Appendicular abscess
Chronic appendicitis
Appendicular mass
Acute appendicitis
Acute appendicitis is due to -
Faecoliths
Worms of ileo-caecal region
Streptococcal infections
Abuse of puragatives
None of the above
Acute appendicitis is best diagnosed by -
History
Physical examination
X-ray abdomen
Ba meal
All of the following signs are not seen in acute appendicitis except -
Rovsing's
Murphy's sign
Boa's sign
Mack wen's sign
Most common cause of colonic obstruction is -
Volvulus
Hernia
Adhesions
Neoplasm
Commonest cause of acute intestinal obstruction is -
Adhesions
Volvulus
Inguinal hernias
Internal hernias
Apex of volvulus of Sigmoid colon in plain X – ray abdomen is at the - a) Left iliac fossa
b) Right iliac fossa
c) Right hypochondrium
d) Left hypochondrium
Apex of volvulus of cecum in plain X - ray abdomen is at the-
Left iliac fossa
Right iliac fossa
Right hypochondrium
Left hypochondrium
Best investigation of acute mechanical intestinal obstruction is -
X-Ray abdomen
Barium enema
Proctosigmoidoscopy
Flatus tube
Paralytic ileus is caused by -
Peritonitis
Hyperkalemia
Acute intestinal obstruction
Head injury
Primary feature of small intestinal obstruction -
Fever
High peristalsis with colic
Abdominal distension
Empty rectum
Treatment of choice of acute obstruction due to left sided colonic carcinoma in a 70 year old male is -
Left sided colectomy
Total colectomy
Hartman's procedure
Defunctioning colostomy
Best way to diagnose lower intestinal obstruction -
Pain abdomen
Abdominal distension
Profuse vomiting
Multiple air gas shadows on X – ray
Commonest type of anorectal abscess is -
Ischio rectal
Submucous
Pelvi-rectal
Perinala
Cancer of the anus is commonly -
Adenocarcinoma
Squamous carcinoma
Melanoma
Sarcoma
Commonest cause of bleeding PR in a male between 20-40 yrs is -
Carcinoma Rectum
Internal haemorrhoids
Fissure in anus
Rectal polyp
Commonest complication following haemorrhoidectomy is -
Haemorrhage
Infection
Faecal impaction
Urinary Retention
The treatment of choice in fistula in anus -
Anal dilatation
Fissurotomy
Fistulectomy
Fistulotomy
Internal sphincterotomy is the treatment of choice for-
Piles
Fistula
Fissure-in-ano
Carcinoma
Best investigation to diagnose piles is -
Proctosigmoidoscopy
Barium enema
Ultrasound
Proctoscopy
Best diagnostic aid in blunt trauma abdomen is-
CTscan
4 quadrant aspiration
Peritoneal lavage
Ultrasound
Treatment of choice for stab injury caecum –
Caecostomy
Ileo-transverse anastomosis
Transverse colostomy
Sigmoid colostomy
In penetrating injury of abdomen commonly affected is -
Liver
Large bowel
Duodenum
Small intestines
Initial treatment in a management of trauma -
Airway
IV fluids
Fracture stabilization
Do not shift
Death in blunt trauma chest is due to –
Rupture oesophagus
Tracheobronchial injury
Pulmonary contusions
Chylothorax
Which one of the following veins should be avoided for intravenous infusion in the management of abdominal trauma -
Cubital
Cephalic
Long saphenous
External jugular
Most common cause of acute pancreatitis is
Biliary tract diseases
Alcoholism
Post traumatic
Idiopathic
Most common cause of pancreatic pseudocyst formation is -
Trauma
Pancreatitis
Neoplastic
None of the above
Commonest complication of pseudocyst of the pancreas is -
Rupture into periotoneum
Rupture into colon
Haemorrhage
Infection
Treatment of congenital cyst of head of pancreas -
Total excision
Partial excision
Marsupialization
Observe and medical treatment
Which one of the following types of pancreatitis has the best prognosis -
Gall stone pancreatitis
Alcoholic pancreatitis
Idiopathic pancreatitis
Traumatic pancreatitis
Somatostatin is secreted by –
A cells
B cells
D cells
Dl cells
Serum amalyse levels raised in all except -
Duodenal ulcer perforation
Pancreatitis
Appendicitis
Small bowel strangulation
Which one of the following is best avoided in the treatment of acute pancreatitis
Antibiotics
Nasogastric suction
Anticholinergics
Morphine
Ответы
C
A
A
C
C
D
A
A
B
A,C
C
D
D
A,C
C
A
B
D
B
B
C
E
A
A
A,B,C
C
A
D
A
C
B
B
A,B,C,D
A
A
D
A
A
E
B
A
D
A
B
B
C
B
B
C
B,D
A
A
C
A
A
A
C
A,B
B
A
D
A
D
B
A
A
B
C
D
D
B
B
D
D
C
D
A
B
D
A
B
D
A
B
D
C
A
C
C
C
Схема учебно-клинической истории болезни хирургического больного и перечень заболеваний больных, представляемых на курацию студентам
С Х Е М А
Учебно-клинической истории болезни
Общая часть
Ф.И.О.;
Возраст;
Место работы, профессия;
Домашний адрес;
Дата поступления (час поступления указывается при экстренной госпитализации);
Указать: госпитализация в плановом порядке или по неотложным показаниям;
ДИАГНОЗЫ.
1) Диагноз при поступлении (в условиях неполного обследования больного может быть сформулирован с указанием синдрома, например: механическая желтуха, гастродуоденальное кровотечение, кишечная непроходимость).
2) Заключительный клинический диагноз:
а) основное заболевание;
б) осложнения основного заболевания;
в) фоновая патология;
г) сопутствующие заболевания.
Операция (дата и час операции, название).
Фамилия, имя, отчество куратора, № группы, сроки курации.
Жалобы и анамнез.
Жалобы при поступлении.
Жалобы на момент начала курации больного.
Анамнез заболевания (при ургентной хирургической патологии излагается с момента ухудшения состояния пациента): как началось данное заболевание, причины болезни по мнению больного, динамика развития клинических проявлений; лечение до поступления в стационар и его результаты.
Анамнез жизни: социально-бытовой (жилище, питание, личная гигиена, материальная обеспеченность, нервно-психические потрясения); перенесенные заболевания; эпид. анамнез; вредные привычки (наркомания, алкоголизм, курение); а также профессиональный, наследственный; аллергологический и гинекологический анамнез.
Данные объективного исследования
Общее состояние больного (сознание, рефлексы, параличи, парезы, трофические расстройства);
Рост, вес, телосложение;
Температура тела;
Кожные покровы и слизистые (цвет, тургор кожи, сухость, потливость, рубцы, отеки);
Состояние питания (подкожная клетчатка);
Мускулатура (хорошее развитие, дряблая);
Костно-суставная система (нормальное развитие, имеются деформации костей и суставов, непропорциональное телосложение, анкилозы).
Лимфатическая система: шейные, подмышечные, кубитальные, мезентериальные, подвздошные, паховые и подколенные лимфоузлы.
Сердечно-сосудистая система (+ патологическая пульсация, варикозное расширение подкожных вен).
Голова и шея: а) зрачки сужены, расширены равномерно, неравномерно, реакция на свет и аккомодацию; б) полость рта: язык, зубы, миндалины; в) щитовидная железа.
Грудь: форма грудной клетки, оценка состояния молочных желез, тип дыхания, перкуссия и аускультация легких; границы и тоны сердца, пульс, артериальное давление; функциональные пробы (проба Штанге-Саабразе).
Исследование живота (осмотр, пальпация, перкуссия, аускультация). Форма и объем живота. Передняя брюшная стенка (болезненность, напряжение мышц, грыжевые выпячивания). Желудок, кишечник, печень, селезенка. Задний проход (осмотр, пальцевое исследование).
Мочеполовая система (пальпация почек, области мочеточников, мочевого пузыря).
Status localis (выделяется у пациентов с заболеваниями, при которых патологический очаг определяется визуально или хорошо доступен пальпаторному исследованию, а именно – у больных с грыжами, проктологическими заболеваниями, кожными проявлениями заболеваний, патологией щитовидной железы и т.п.).
Данные срочных клинико-инструментальных методов исследования: общий анализ крови, общий анализ мочи, анализ крови и анализ мочи на сахар, -амилазу, обзорная R-графия грудной клетки и брюшной полости (у больных, госпитализированных по неотложным показаниям).
Предварительный диагноз (разделы IV и V у планово госпитализированных больных могут быть опущены).
Назначения согласно установленному предварительному диагнозу (стол питания, режим, лекарственные препараты - доза, метод и количество введений).
План предполагаемого обследования больного.
Данные дополнительных (уточняющих патологию) клинико-инструментальных методов исследования.
Основной клинический диагноз.
Осложнения основного заболевания.
Фоновая патология.
Сопутствующие заболевания.
Обоснования основного заболевания и его осложнений путем последовательного рассмотрения полученных данных (анамнестических, объективных, лабораторно-инструментальных).
Вероятная этиология и патогенез основного заболевания у курируемого больного.
Обоснование выбора метода лечения у курируемого больного.
Общие принципы консервативного и (или) оперативного лечения заболевания у курируемого больного.
Дневники ежедневного наблюдения и лечения.
У оперированных оформляются следующие разделы:
Предоперационный эпикриз (пишется в дневнике наблюдения накануне операции). В эпикризе указываются: характер поступления больного в клинику (плановый, экстренный), основные жалобы, особенности развития заболевания, важные сведения из анамнеза жизни, объективные данные и результаты лабораторно-инструментальных методов исследования, на основании которых поставлен диагноз. В эпикризе должны быть отмечены изменения в других органах и системах, которые влияют на определение показаний и противопоказаний к операции. В заключение указываются предполагаемые метод обезболивания и объем операции, операционно-анестезиологический риск по одной из классификаций, проведенная предоперационная подготовка.
Протокол оперативного вмешательства (анестезиологическое пособие, название и описание операции, операционная бригада).
Описание удаленного операционного препарата и данных морфологического исследования.
Послеоперационный диагноз.
Послеоперационные назначения.
Дневники ежедневного послеоперационного наблюдения и лечения.
Эпикриз: должен содержать основные сведения из жалоб, анамнеза, объективных и лабораторных данных, на основании которых поставлен диагноз и определено показание к тому или иному методу лечения, в том числе - к операции. Необходимо отметить состояние и изменения со стороны основных систем организма, а также характер проведенного лечения (конкретно) и его результаты: изменения в состоянии больного, лабораторных данных и т.п. В случае оперативного лечения должно быть описано, что обнаружено во время операции, какая операция выполнена с оценкой течения послеоперационного периода. Заканчивается эпикриз рекомендациями по дообследованию (при необходимости) и дальнейшему лечению.
Прогноз для здоровья, для жизни, для труда.
Литература (источники), использованная при написании истории болезни (монографии, руководства, журнальные статьи, электронный адрес и название публикации в Интернете, при ссылке на лекции - ученое звание, Ф.И.О. лектора, тема лекции, год).
ФОРМА НАПИСАНИЯ ИСТОЧНИКОВ ЛИТЕРАТУРЫ:
Крылов Н.Н. Хроническая анальная трещина // Вестник хирургической гастроэнтерологии. – 2008. – №1. – С.5-11.
Кукош М.В., Петров М.С. Острый деструктивный панкреатит. – Нижний Новгород, 2006. – 124с.
Лелянов А.Д., Жинко Ю.Н., Логоватовский О.В. и др. Проблемы лечения некротизирующей инфекции мягких тканей // Клиническая больница скорой медицинской помощи (к 110-летию основания). – Смоленск: Универсум, 2007. – С. 213-223.
Липатов В.А. Диагностика острого аппендицита. – http://www.trimm.ru
Прудков М.И.Основы миниинвазивной хирургии. – Екатеринбург, 2007. – 64с.
Семенов С.В., Казаков И.П. Применение озона в интенсивной терапии разлитого перитонита // Озон в биологии и медицине: Тезисы 5-й Всероссийской научно-практической конференции. – Нижний Новгород, 2003. – С.181-182.
Хроническая дуоденальная непроходимость. – Лекция проф. С.А.Касумьяна (2009).
Шевченко А.А. Клинический уход за хирургическими больными. Уроки доброты. – 2008. – 416с.
Thomson A., Miles A. Manual of surgery. – Volume first: General Surgery. – Sixth Edition. – London, 2006. – 565p.
Felice G., Privitera A., Klaumann M. Doppler-Guided hemorrhoidal artery ligation: an alternative to htmorrhoidectomy // Diseases of the colon and rectum. – 2005. – Vol.48, №11. – P.2090-93.
АЛГОРИТМЫ ВЫПОЛНЕНИЯ
ОСНОВНЫХ ВРАЧЕБНЫХ МАНИПУЛЯЦИЙ
Субъективные методы исследования
1. Расспрос больного.
Распросс больного следует вести по строгому плану, изучая последовательно жалобы больного и его субъективное состояние, анамнез настоящего заболевания, анамнез жизни, данные о наследственности.
Объективные методы исследования
1. Осмотр.
Осмотр делится на общий и местный, хотя это деление в значительной степени условно. Общий осмотр дает представление о состоянии сознания больного, его положении, психическом облике, общем виде, состоянии кожных покровов и видимых слизистых оболочек. Местный осмотр предусматривает последующий детальный осмотр отдельных частей тела: головы, лица, шеи, полости рта, грудной клетки, живота, конечностей.
При проведении осмотра больного требуется соблюдение ряда обязательных условий:
1) должно быть соответствующее освещение (достаточная сила света, концентрация освещения, прямое направление лучей и т. д.). Лучше всего удается выявлять различные изменения при дневном оевещении. Если нет возможности использовать для осмотра дневной свет, то следует применять рассеянный белый искусственный свет от сильного источника.
2) осмотр следует производить систематически и по плану. Для этого больного надо полностью раздеть. Выявляя при осмотре (а также при других физических методах исследования) тот или иной патологический симптом, надо правильно локализовать его на поверхности тела, для чего необходимо пользоваться клинической топографией.
3) Для правильной постановки диагноза большую помощь может оказать осмотр выделений больного: мокроты, мочи, кала, рвотных масс.
Осмотр аноректальной области относится к местным видам осмотра. Для этого необходимо руками развести ягодицы и осмотреть задний проход, крестцово-копчиковую область и промежность. При осмотре следует попросить больного натужиться, что позволит выявить невидимые при обычном состоянии геморроидальные узлы, выпадение слизистой оболочки кишки, низко расположенные опухолевые образования кишки.
2. Пальпация.
Для успешного применения этого способа исследования необходимо соблюдать ряд технических условий:
1. Очень важно выбрать правильное положение больного. Оно должно быть таким, чтобы ощупывающие пальцы могли легко найти доступ к тому или иному внутреннему органу. В зависимости от того какой орган ощупывается, положение может быть различным: лежа (на спине, на боку, на животе), стоя, коленно-локтевое. Пальпации очень мешает напряжение мышечного слоя. Для расслабления этого напряжения нередко приходится просить больного изменить положение туловища или конечностей (так, для расслабления мышц передней брюшной стенки пациент, лежа на спине, должен согнуть ноги в тазобедренных и коленных суставах).
2. Другим важным условием для успешной пальпации является соответствующее положение врача. Оно должно быть удобным и обеспечивать свободу движений руки. Удобнее всего врачу сидеть справа от больного лицом к нему. Руки исследующего должны быть теплыми, гибкими, нежными, ногти коротко острижены. Движения – легкими, эластичными и осторожными.
При ощупывании органов брюшной полости нередко приходится пользоваться дыхательными движениями брюшной стенки. Дышать больной должен глубоко, через рот, применяя брюшное дыхание.
В медицинской практике применяются такие виды пальпации, как поверхностная, глубокая, проникающая и др.
Поверхностная пальпация совершается ладонями, свободно положенными плашмя, при этом ощупываемая область почти не продавливается. Этот способ позволяет произвести ориентировочное исследование соответствующей области и является предварительным этапом пальпации.
Глубокая пальпация является основным видом этого метода исследования. Она совершается пальцами с применением существенного давления (следует надавливать только пальцами, сохраняя более или менее пассивной руку).
Достаточную информацию об органе брюшной полости удается получить с помощью глубокой скользящей пальпации по В.П.06разцову, Н.Д.Стражеско.
Проникающая пальпация осуществляется двумя-тремя пальцами, проникающими глубоко в полость на ограниченном пространстве.
Бимануальная пальпация выполняется обеими руками исследующего (обычно левая рука приближает к правой исследуемый орган, что позволяет охватить его руками).
Толчкообразная пальпация часто позволяет обнаружить наличие жидкости в полости. Тремя-четырьмя пальцами, прижатыми друг к другу и установленными над соответствующим участком тела, делают несколько коротких и сильных нажимающих движений (толчков).
С помощью пальпации определяется упругость и влажность кожи, температура тела. Она позволяет выявить всевозможные поверхностно расположенные опухоли, обнаружить наличие отечности тканей, воспалительных инфильтратов, мышечных атрофий.
3. Перкуссия.
В хирургической практике применяют следующие виды перкуссии: непосредственная, посредственная, сравнительная и топографическая.
Непосредственная перкуссия производится одним или двумя пальцами по определенной исследуемой области тела. При таком способе перкуссии большое значение имеет осязание, позволяющее ощутить сопротивление перкутируемых тканей. Наибольшее распространение при непосредственной перкуссии получил способ Образцова, при котором перкуссия выполняется ударом указательного пальца правой руки при соскальзывании его со среднего пальца – метод щелчка.
Посредственная перкуссия. Врачи используют дигитальный опособ перкуссии – выстукивание пальцем по пальцу. Перкуссионные удары следует наносить средним пальцем правой руки, который должен быть согнут и не соприкасаться с другими пальцами, по среднему или указательному пальцу левой руки, по его средней или ногтевой фаланге. Удар производится не за счет пястно-фалангового сочленения, а за счет лучезапястного сустава.
Сравнительная перкуссия ставит своей задачей сравнение анатомически одинаково расположенных перкуторных объектов.
Топографическая перкуссия преследует цель разграничить те или иные перкутируемые анатомические образования.
Какую бы задачу ни преследовала перкуссия, она требует соблюдения следующих общих правил:
1) удобнее всего перкутировать больного в положении сидя или стоя;
2) в помещении необходимо соблюдать тишину.
4. Аускультация.
Аускультация предусматривает выслушивание звуков, возникающих в организме самостоятельно: дыхательных, сердечных тонов и шумов кишечной перистальтики.
По способу выслушивания различают непосредственную и посредственную аускультацию. Непосредственная аускультация проводится путем прикладывания уха врача к телу больного. Посредственная аускультация осуществляется с помощью специальных приборов — стетоскопа, фонендоскопа.
Для получения наиболее достоверных данных при аускультации необходимо соблюдать определенные условия:
1) полнейшая тишина в помещении;
2) выслушивать надо обнаженное тело, ибо одежда может издавать побочные шумы;
3) стетоскоп (фонендоскоп) следует плотно прикладывать к телу;
4) врач и больной должны принять удобное для каждого положение: легкие лучше выслушивать при вертикальном положении больного; сердце и живот — в положении лежа; при выслушивании органов грудной клетки у женщин им надо предложить отвести грудные железы кверху и несколько кнаружи;
5) дыхание больного при выслушивании грудной клетки должно быть спокойным, глубоким, обычного темпа. Выслушивание проводится на протяжении всего дыхательного акта — от вдоха до выдоха;
6) при выслушивании сердца дыхание больного должно быть более поверхностным, а еще лучше, если исследуемый на некоторое время задержит его, чтобы дыхательные шумы не мешали выслушивать.
5. Клиническая антропометрия.
Клиническая антропометрия – способ изучения человека при помощи измерений.
Каждый врач должен знать размеры своего пальца (ширину, длину его фаланги), ширину кисти, чтобы использовать их в случае необходимости измерения размеров органов или патологических участков на поверхности тела.
6. Определение характера пульса.
Место определения пульса, как правило, это лучевая артерия кнутри от лучевой кости, несколько выше лучезапястного сгиба.
Если по какой-либо причине пальпировать лучевую артерию не удается, пульс можно определить на сонных, височных, бедренных, плечевых артериях.
Принято различать следующие свойства пульса: частоту, ритм, наггряжение, наполнение, величину, форму.
Частота пульса – число пульсовых ударов в минуту. В норме число пульсовых волн у мужчин в среднем равно 70, у женщин – 80 уд./мин. При неправильном ритме пульса счет пульсовых ко-лебаний надо проводить на протяжении минуты.
Ритм пульса определяется чередованием пульсовых ударов, следующих друг за другом через равные промежутки времени с одинаковыми амплитудами. Ритм пульса является отражением сокращения левого желудочка сердца.
Различают правильный, ритмичный пульс и неправильный, аритмичный пульс. Пульсовые волны в норме бывают равны между собой – равномерный пульс, в патологических условиях они имеют различную величину – неравномерный пульс.
Экстрасистолия – появление за нормальным пульсовым ударом дополнительного, меньшего по наполнению и сопровождающегося более длительной паузой.
Мерцательная аритмия – полная неправильность ритма. Число пульсовых ударов при мерцательной аритмии, как правило, меньше числа сердечных сокращений, определяемых аускультацией сердца. Эта разность носит название дефицита пульса.
Напряжение пульса определяется той степенью давления, которое оказывают на сосуд ощупывающие его пальцы, чтобы полностью прекратить пульсовую волну. Это свойство пульса дает представление о величине артериального давления внутри ощупываемой артерии. При этом различают напряженный, твердый пульс, встречающийся при гипертонической болезни, и нена-пряженный, мягкий пульс, наблюдающийся при падении кровяного давления.
По наполнению различают полный пульс и пустой. Пульс малого наполнения, мягкий, едва прощупываемый называется нитевидным.
Величина пульса складывается из оценки его наполнения и напряжения. Она наиболее полно определяет достаточность работы сердца и зависит от разницы степени напряжения артерий в момент систолы и в момент диастолы. По величине различают большой и малый пульс.
Форма пульса определяется характером подъема и падения давления внутри артерии во время прохождения пульсовой волны. Пульс, при котором отмечается быстрый подъем пульсовой волны и быстрое падение, носит название быстрого, скачущего. Пульс, характеризующийся медленным подъемом и медленным падением пульсовой волны, называется медленным. Кроме того, по форме выделяют еще так называемый дикротический пульс, когда за главной пульсовой волной ощущается еще одна отчетливая новая волна, как бы вторая пульсовая волна меньшей силы.
7. Измерение артериального давления.
В нормальных условиях уровень систолического артериального давления равен 110-140 мм рт. ст., уровень диастолического давления – 60-90 мм рт. ст. Измерение артериального давления производихся в плечевой артерии с помощью специальных аппаратов.
Существуют два способа определения величины артериального давления: пальпаторный способ Рива-Роччи и аускультативный способ Короткова. Каким бы способом ни исследовалось артериальное давление, обязательным условием является расположение сдавливающей плечевую артерию манжетки на уровне сердца; при этом больной может либо сидеть, либо лежать.
Измерение АД по Рива-Роччи. После наложения манжетки тонометра на плечевую артерию в средней трети плеча (удобнее всего накладывать манжетку на правое плечо) пальцы левой руки исследователя помещаются на лучевую артерию в месте, где обычно пальпируется пульс. В правую руку исследователь берет грушу аппарата. Постепенно наполняя манжетку воздухом, следят за моментом исчезновения пульса на лучевой артерии и определяют силу сдавления манжетки по шкале прибора. Показания шкалы прибора будут соответствовать максимальному систолическому давлению. Далее, уменьшая давление в манжетке, вновь отмечают момент появления пульса на лучевой артерии (уровень максимального, систолического давления), а затем определяют момент четкого прощупывания пульса на лучевой артерии. Показания шкалы манометра в этот момент будут соответствовать минимальному, диастолическому давлению.
Измерение АД по Короткову. Манжетка тонометра накладывается на правое плечо пациента на расстоянии 2 см выше локтевого сгиба. Пальпаторно определяется плечевая артерия, и на это место ставят головку фонендоскопа. В манжетку нагнетается воздух до полного исчезновения пульса на лучевой артерии. Постепенно выводя воздух из манжетки, выслушивают плечевую артерию в области плечевого сгиба. Показания шкалы манометра в момент появления сосудистого тона будут соответствовать максимальному, систолическому давлению. Продолжая уменьшать давление воздуха в манжетке и слушая тоны сосуда на плече, определяют момент исчезновения тонов. Показания шкалы манометра при этом будут соответствовать минимальному, диастолическому давлению.
8. Измерение венозного давления.
Венозное давление обычно измеряется прямым (кровавым) способом с помощью флеботонометра Вальдмана. Нулевое деление шкалы аппарата устанавливается на уровне нижнего края грудной мышцы в подмышечной впадине, что соответствует уровню правого предсердия. После введения иглы, соединенной с аппаратом, в локтевую вену снимается зажим с трубки и поступающая в нее кровь поднимает уровень жидкости в манометрической трубке до метки, определяющей величину венозного давления.
Дигитальный метод дополнительного исследования
Пальцевое исследование прямой кишки.
Пальцевому исследованию прямой кишки обязательно преджествует осмотр аноректальной области. Пальцевое исследование прямой кишки лучше всего проводить в колено-локтевом положении исследуемого и на боку. В положении «на корточках» палец удается ввести в просвет прямой кишки на несколько сантиметров выше. Врач всегда должен четко представлять цель исследования.
Технические приемы и интерпретация результатов исследования. На правую руку надевают резиновую перчатку, второй палец смазывают вазелином и винтообразным движением вводят его в прямую кишку. В момент введения пальца в кишку оценивается состояние тонуса сфинктера прямой кишки (в норме сфинктер должен плотно охватывать палец). Введя палец в кишку, врач определяет болезненные участки кишки, наличие опухолевых образований на ее стенке, а также выявляет состояние органов и тканей, расположенных в непосредетвенной близости к стенке прямой кишки (предстательная железа у мужчин, матка у женщин, параректальная клетчатка, лимфатические узлы). Необходимо обратить внимание на содержание просвета кишки – наличие каловых масс, слизи, гноя и крови.
Инструментальные манипуляции
1. Исследование прямой кишки с помощью ректального зеркала.
Перед введением ректального зеркала в прямую кишку его бранши необходимо тщательно смазать вазелином на всем протяжении. При осторожном и медленном введении ректального зеркала в кишку после расширения браншей до 2,5 см удается осмотреть переднюю, заднюю и боковые стенки кишки.
Ано- и ректоскпия.
Необходимым условием для успешного проведения ректоскопии является хорошая очистка кишечника. Для ректо(ано)скопии больной должен принять коленно-локтевое положение. Тубус ректо(ано)скопа необходимо густо смазать вазелином. Ректо(ано)сколическое исследование состоит из двух моментов: введение ректо(ано)скопа в просвет прямой кишки и осмотр. При введении ректо(ано)скопа в кишку врач должен сконцентрировать свое внимание на процессе продвижения тубуса на максимальную глубину. При этом необходимо помнить, что никогда не следует применять силу, так как легко повредить стенку прямой кишки.
Смазанный вазелином тубус ректо(ано)скопа с мандреном вводится на глубину 5 см параллельно поверхности стола, на котором располагается больной. Затем после удаления мандрена производится осмотр при аноскопии или при ректоскопии укрепляется защитная крышка со стеклом, смотровой конец ректоскопа опускается книзу, а ректальный конец в этот момент подни-мается кверху вдоль крестцового изгиба ампулы кишки. Включив свет и раздувая кишку, надо осторожно продвигать ректо(ано)скоп вперед. На уровне 12 см (от 11 до 13 см) положение тубуса ректоскопа вновь выравнивается почти до горизонтальной линии. На глубине 13 см при продвижении в сигмовидную кишку кишечный конец тубуса ректоскопа круто направляется книзу, а смотровой конец – кверху. В таком положении ректоскоп продвигается дальше в просвет сигмовидной кишки.
После того как ректо(ано)скоп максимально введен в просвет кишки, приступают к извлечению его и тщательному осмотру всех стенок кишки с внутренней стороны. Извлечение трубки ректо(ано)скопа производят так, чтобы кишечный ее конец совершал спиралеобразное движение. Заметив какие-либо изменения на стенке кишки, отмечается место их расположения относительно анального отверстия по сантиметровым отметкам на наружной поверхности тубуса.
3. Катетеризация мочевого пузыря заключается во введении катетера в мочевой пузырь через мочеиспускательный канал (уретру) с целью: 1) выведения из пузыря мочи, если последняя не выделяется естественным путем; 2) промывания просвета пузыря; 3) введения в просвет пузыря лекарственных препаратов; 4) извлечения из пузыря мочи для исследования.
Для катетеризации мочевото пузыря применяются различные катетеры: резиновый (Нелатона), из плотной резины с конически изогнутым клювом (Тиммана), Эластический с изогнутым клювом (Мерсье), катетер Фоллея, металлический мужской и женский. Металлические катетеры могут быть использованы в тех случаях, когда катетеризация эластическими катетерами не удается. Катетеризация мочевого пузыря должна производиться в асептических условиях. Руки хирурга и мочевой катетер должны быть стерильны. Наружное отверстие мочеиспускательного канала должно быть обработано раствором соответствующего антисептика.
Техника введения резинового катетера. Пинцетом катетер захватывается несколько выше окошка, павильон катетера держат между V и IV пальцами. Хорошо смазанный стерильным вазелиновым маслом катетер вводят в мочеиспускательный канал и медленно продвигают по уретре. Проведение катетера через мембранную часть уретры может быть затруднено из-за спазма наружного сфинктера. В таких случаях следует немного выждать, заставить больного глубоко дышать, расслабить мышцы живота и промежности и, постепенно преодолевая препятствие, проводить катетер в мочевой пузырь. О том, что катетер прошел в просвет мочевого пузыря говорит появление из него мочи.
Резиновый катетер может быть оставлен в полости мочевого пузыря на продолжительное время в виде так называемого постоянного катетера. Для этого катетер фиксируют к половому члену марлевыми полосками или полосками лейкопластыря. Для длительной катетеризации мочевого пузыря лучше использовать специальный катетер Фоллея.
Введение металлического катетера у мужчин проводится в четыре этапа:
I этап – держа катетер с направленным вниз клювом в горизонтальном положении над животом больного, вводят его в отверстие мочеиспускательного канала, стараясь, чтобы он прошел по задней стенке канала.
II этап – проведя катетер через передний отдел мочеиспускательного канала, правой рукой продвигают катетер дальше, постепенно поднимая его наружный конец, в то время как левой рукой наклоняют половой член к животу и несколько натягивают его навстречу продвигающемуся по уретре катетеру, пока клюв катетера не достигнет лонного сочленения. В этот момент клюв катетера подходит к заднему отделу мочеиспускательного канала, причём правая рука ощущает, что катетер как бы стремится принять вертикальное положение.
III этап – проводя катетер по каналу, ощущают, что клюв его упирается в мочевую диафрагму. Катетер с половым членом переводят в вертикальное положение, левым указательным пальцем нащупывают его клюв со стороны промежности и, оказывая на него некоторое давление, направляют к передней стенке канала.
IV этап – осторожно продвигая катетер вперед по каналу, ошущают, как клюв его проскальзывает в перепончатый отдел мочеиспуокательного канала (сопротивление продвижению катетера уменьшается). Теперь наружный конец катетера постепенно отводится от живота. При этом катетер ставится сначала в вертикальное положение к линии живота, а затем под тупым углом, открытым кверху. Соответственно изменяется и положение полового члена. Выведение металлического катетера из мочевого пузыря производится в обратном порядке.
4. Венесекция.
Венесекция – вскрытие просвета вены путем рассечения ее стенки. К этой манипуляции приходится прибегать в тех случаях, когда подкожная вена не дифференцируется, а больной нуждается в экстренном введении лекарственных веществ в вену.
Для венесекции вена должна быть обнажена путем рассечения над ней кожи и подкожной клетчатки. Поэтому для выполнения венесекции необходимо иметь: раствор для анестезии кожи, шприц для анестезии, скальпель, сосудистые зажимы, шовный материал для манипуляций на вене и для зашивания тканей, иглодержатель и иглы для наложения швов, катетер для интубирования вены, ножницы.
Манипуляция при венесекции проводится с соблюдением всех правил асептики. Руки хирурга, используемый материал и инструменты должны быть стерильны.
Техника венесекции. Местом для обнажения вены обычно является область локтевого сгиба. После обработки кожи раствором соответствующего антисептика производится анестезия ее и подкожной клетчатки. Убедившись, что анестезия наступила, производят разрез кожи и подкожной клетчатки над веной. Направление разреза должно быть поперечным по отношению к оси конечности, это позволит легче обнаружить вену. Для обнаружения вены в подкожной клетчатке последняя разводится с помощью зажима. Вену необходимо взять на держалки. Для этого с помощью зажима под вену подводятся две лигатуры, одна из которых располагается ближе к периферии вены, другая – ближе к центру ее. Периферической нитью вена перевязывается, а центральная нить служит держалкой для вены. С помощью этой держалки вена приподнимается, несколько натягивается, что позволяет ее фиксировать. После этого стенка вены рассекается ножницами. Следует быть очень осторожным, чтобы не пересечь вену полностью. В отверстие стенки вены вставляется специальный катетер, который фиксируется в просвете вены нитью, расположенной у центрального конца. Рана кожи в области локтевого сгиба зашивается до катетера. На нее накладывается асептическая повязка.
Очень важно следить за тем, чтобы в просвете катетера не было пузырьков воздуха.
5. Пункция плевральной полости.
Манипуляция проводится с соблюдением всех правил асептики. Руки хирурга, используемый материал и инструменты должны быть стерильны.
Технические принадлежности: шприц с иглой и раствор анестетика для проведения местной анестезии; шприц для отсасывания жидкости из плевральной полости; специальную пункционную иглу достаточного калибра и длины; мерную емкость для определения количества эвакуируемой жидкости; предметные стекла для приготовления мазков; стерильные пробирки с ватными пробками для бактериологического исследования содержимого плевральной полости; антисептики для обработки участка кожи в зоне пункции.
Место пункции. Пункция плевральной полости производится в том месте, где обнаруживается скопление жидкости. Однако наиболее подходящими местами для пункции плевральной полости являются следующие точки: под VIII и IX ребром по лопаточной линии, под VII ребром по средней подмышечной линии. При большом количестве жидкости в плевральной полости, что приводит к смещению диафрагмы книзу, проколы можно делать на одно межреберье ниже, при высоком стоянии куполов диафрагмы проколы надо делать выше.
Техника прокола. Пункцию плевральной полости удобнее всего делать в сидячем положении. Больного надо посадить на стул, прислонив его к спинке здоровой половиной грудной клетки. Рука больного, соответствующая стороне прокола, должна быть поднята и в этом положении удерживаться помощником. Это обеспечивает расширение межреберных промежутков. Кожу в зоне манипуляции обрабатывают раствором йода. Место пункции анестезируется. Прокол делают специальной иглой, соединенной с резиновой трубкой или специальным устройством с регулирующим краником, имеющими канюлю для подсоединения шприца. После того как конец иглы прошел в мягкие ткани грудной клетки, подсоединяется шприц. При применении резиновой трубки в момент отсоединения шприца на нее накладывается зажим, при использовании специального устройства с регулирующим краником – последний устанавливается в закрытое положение. Игла продвигается в глубь тканей в сторону плевральной полости в перпендикулярном направлении, из плевральной полости извлекается быстрым движением. Место пункции обрабатывается дополнительно антисептиком.
6. Пункция полости перикарда.
Манипуляция проводится с соблюдением всех правил асептики. Руки хирурга, используемый материал и инструменты должны быть стерильны.
Технические принадлежности: шприц емкостью 5-10 см3; тонкие, точно подобранные к шприцу, безукоризненно гладкие, хорошо отточенные, с коротко срезанным острием иглы; измерительный сосуд; антисептики для обработки кожных покровов; раствор анестетика и шприц для местной анестезии.
Место пункции: 1) непосредственно у верхушки мечевидного отростка или у левого края его – субстернальный прокол; 2) IV или V межреберье слева, вблизи левого края абcолютной тупости сердца – межреберный прокол; 3) IV или V межреберье справа на расстоянии не менее 3 см от края грудины.
Подготовка к пункции. Прежде чем произвести пункцию полости перикарда, надо окончательно убедиться в том, что в полости сердечной сорочки имеется скопление жидкости и что в намеченном для пункции месте сердце не прилегает к грудной стенке – проводится эхокардиографическое исследование (ранее – успешно применялось рентгенологическое исследование).Наличие даже незначительного шума трения перикарда или едва заметной пульсации говорит о том, что сердце находится очень близко к грудной клетке и в этом месте пунктировать перикард не следует.
Больному придают полусидячее положение в постели с надежной поддержкой для головы. Место прокола анестезируют (например:1 % раствором новокаина), кожу в зоне вмешательства обрабатывают раствором соответствующего антисептика.
Техника пункции полости перикарда. При субстернальном проколе врач располагается справа от больного, кладет пальцы левой кисти на нижнюю треть грудины, устанавливая концевую фалангу указательного пальца у намеченного места прокола. Правой рукой берет иглу длиной 10-12 см и вкалывает ее в место прокола, направляя острие кверху под очень острым углом к передней поверхности надчревья. В таком положении игла проводится через кожу, подкожную клетчатку и фасцию живота снизу вверх – первое направление. Затем, еще более наклонив иглу к брюшной стенке, ее направляют вверх, так чтобы она оказалась непосредственно кзади от задней поверхности мечевидного отростка – второе направление. Проведя иглу в этом направлении на расстоянии около 2 см, ее направляют несколько кзади – третье направление и, проведя вперед, попадают в полость перикарда. Как только игла попадет в полость перикарда, наполненную жидкостью, последняя начинает выделяться через иглу.
Субстернальный прокол наименее опасен.
Межреберный прокол. Направление иглы при проколе межреберья у правого края грудины перпендикулярно к поверхности кожи, а при проколе в V или VI межреберье слева иглу следует направлять несколько снизу вверх; длина иглы 5-6 см. Продвижение иглы через грудную стенку должно быть очень осторожное, медленное, ибо слой жидкости в полости перикарда в месте прокола через межреберье очень небольшой и игла может попасть в сердце. Введя иглу на глубину 0,5-1 см, надо надеть на нее шприц и потянуть поршень наружу. При отсутствии в просвете шприца жидкости, не снимая шприц и вытягивая наружу поршень, продолжают медленное продвижение иглы дальше. Благодаря такому приему, как только игла попадет в слой жидкости, последняя немедленно заполняет шприц. Обычно это происходит, когда игла проникает на глубину 2-2,5 см. Если в шприце находится чистая кровь, значит игла попала в полость сердца. Ее немедленно надо извлечь.
Отсасываемую из полости перикарда жидкость отправляют для химичеокого и бактериологического исследования. Измеряют общее количество эвакуираванной жидкости.
7. Пункция брюшной полости (лапароцентез).
Технические принадлежности: шприц емкостью 5-10 мл с тонкой иглой для анестезии брюшной стенки и раствор анестетика (например:0,25% раствор новокаина); скальпель; толстый пуговчатый зонд; сосуд емкостью до 10 л для собирания эвакуируемой жидкости; перевязочный материал (марлевые шарики, салфетки); иглодержатель, игла и шовный материал; пробирки и предметные стекла для выполнения лабораторных исследований удаляемой жидкости; брюшной троакар.
Место прокола брюшной стенки – подчревная область: 1) более предпочтительно – по средней линии живота на середине раостояния между пупком и лобком (ниже прокол делать опасно, так как можно повредить мочевой пузырь и матку у женщин); 2) кнаружи от середины линии, соединяющей пупок с левой передневерхней остью (линия Монро-Рихтера).
Техника манипуляции. Перед проколом брюшной стенки необходимо освободить мочевой пузырь и очистить кишечник. Больному производится премедикация (например: вводится 1 мл 1% раствора промедола). Прокол брюшной стенки следует делать в сидячем положении. В этом положении свободная жидкость брюшной полости скапливается в нижней ее половине, а петли тонкого кишечника смещаются в верхнюю половину брюшной полости. Больного сажают на стул так, чтобы была опора для спины. Между его раздвинутых ног ставят ведро для собирания эвакуируемой жидкости, на колени стелят клеенку, край которой опускаетюя в ведро. В тех случаях, когда больной не может сидеть, прокол брюшной стенки выполняется в лежачем положении. При этом место пункции должно находиться на левой половине передней брюшной стенки, а больному придают положение на левом боку.
Придав больному соответствующее положение, производят обработку кожи соответствующим антисептиком и делают анестезию тканей в области прокола. После этого производится продольный разрез кожи в предполагаемой точке прокола длиной 0,5-1 см. Троакар с вставленным в него стилетом берется в правую руку так, чтобы рукоятка стилета упиралась в ладонь, а указательный палец располагался у конца троакара на расстоянии, приблизительно равном предполагаемой толщине брюшной стенки. Острие стилета вводится в разрез брюшной стенки перпендикулярно к поверхности кожи. Троакар вводится в брюшную стенку энергичным движением, после чего вращательным движением проводится в ее ткани на намеченную глубину. Проникновение инструмента в брюшную полость обычно четко ощущается рукой по внезапному прекращению сопротивления. Когда конец троакара окажется в брюшной полости, надо, поддерживая его канюлю пальцами левой руки, быстро извлечь стилет правой рукой. При этом из канюли начинает активно поступать жидкость. Скорость истечения жидкости нужно регулировать так, чтобы опорожнение брюшной полости происходило медленно. Во время эвакуации жидкости из брюшной полости помощник, находящийся сзади больного, сдавливает его живот полотенцем для создания постоянного давления в брюшной полости.
Состояние больного должно быть постоянным предметом внимания врача во время лапароцентеза. Следует следить за пульсом и при первых признаках его падения немедленно прекратить ток жидкости. Так же поступают и при появлении симптомов коллапса. Больной укладывается на спину в положение с приподнятым нижним концом туловища, проводятся соответствующие лечебные мероприятия.
Окончание операции. Врач захватывает кожу с подкожной клетчаткой с обеих сторон от места прокола брюшной стенки между пальцами левой руки, а правой рукой быстро извлекает канюлю из брюшной полости. Рана на брюшной стенке обрабатывается соответствующим антисептиком и ушивается 1-2 швами. Сверху накладывается асептическая повязка.
Общее количество жидкости, которое можно эвакуировать из брюшной полости за одну процедуру, определяется состоянием больного и техническими особенностями; если осложнений нет, можно эвакуировать до 7-10 л и более.
8. Пункция коленного сустава.
Положение больного лежа на спине с вытянутой ногой. Место вкола – медиальный край надколенника на середине его высоты. При скоплении жидкости в верхнем завороте сустава проникнуть в него можно у верхнего края надколенника по средней оси бедра.
Для удобства манипуляции следует левой рукой снизу с обеих сторон обхватить сустав и отдавить выпот кверху, чтобы переместить его в верхний заворот.
9. Блокады анестетиками.
Общие положения при проведении блокад анестетиками. Блокады должны выполняться в условиях строгой асептики. Для блокад используют растворы анестетиков, подогретые до температуры тела больного (36-37° С). После блокады больной должен соблюдать абсолютный покой.
Паранефральная (поясничная) блокада заключается во введении раствора анестетика в зону паранефральной клетчатки. Техника: больной укладывается на стол на валике в положении на противоположном зоне блокады боку. Место вкола иглы находится в углу, образованном XII ребром и длинными мышцами спины. Кожа поясничной области обрабатывается соответствующим раствором антисептика, а в месте вкола иглы анестезируется. После этого в правую руку берут шприц, наполненный раствором анестетика, с длинной иглой, проводят прокол кожи в зоне анестезии, продвигают иглу в глубокие ткани поясничной области, все время медленно посылая впереди нее раствор анестетика. При прохождении иглы через апоневротическую ткань ощущается препятствие, которое преодолевается с некоторым усилием. Удерживая широкий конец иглы в левой руке между большим и указательным пальцами, надо часто снимать шприц с иглы и определять момент, когда из иглы перестанет вытекать раствор анестетика, что будет указывать на правильное положение острого конца иглы в межфасциальном почечном пространстве, где раствор анестетика будет свободно распространяться в тканях.
Как только будет установлено правильное положение иглы, начинают дозированное введение анестетика (например: 0,25% раствора новокаина в количестве 100-150 мл). Закончив введение новокаина, иглу быстрым движением извлекают из тканей. Кожу обрабатывают соответствующим антисептиком, на место вкола иглы накладывают асептическую повязку.
При проведении блокады возможно повреждение ткани почки, что проявляется появлением выделения из иглы крови. В таком случае вводить новокаин нельзя, так как это еще больше травми-рует почечную ткань. Правильность техники выполнения паранефральной блокады определяется правилом – «из иглы ни капли жидкости, ни капли крови». Блокада чаще производится с двух сторон.
Блокада круглой связки печени.
Техника: больной лежит в положении «на спине». Кожа живота обрабатывается соответствующим антисептиком. Тонкой иглой производится анестезия кожи по средней линии живота в точке на два поперечных пальца выше пупка. Через образовавшийся желвак длинной иглой, надетой на шприц, наполненный анестетиком, прокалываются кожа, подкожная клетчатка и апоневроз белой линии живота. При проколе апоневроза ощущается достаточно легко преодолеваемое сопротивление ткани. Как только кончик иглы проникнет под апоневроз, введение иглы прекращают и в предбрюшинную клетчатку вводят до 80-100 мл раствора анестетика (например: 0,25% раствора новокаина). При остром панкреатите количество вводимого анестетика может быть увеличено, но не более 350 мл в расчете на 0,25% раствор новокаина. По окончании введения анестетика игла извлекается из тканей, место пункции обрабатывается соответствующим антисептиком и на кожу накладывается асептическая повязка.
При правильно выполненной блокаде круглой связки печени боли в зоне правого подреберья стихают, а в зоне введения анестетика не должен пальпироваться инфильтрат в подкожной клетчатке.
Блокада области пахового канала по М. Ю. Лорин-Эпштейну.
Техника: у мужчин 20 мл раствора анестетика (например: 0,5% раствора новокаина) вводят в толщу семенного канатика. Для этого после обработки кожи паховой области раствором соответствующего антисептика, указательный палец левой руки вводится через корень мошонки в наружное отверстие пахового канала. Кожа над концом указательного пальца анестезируется раствором анестетика через тонкую иглу, а затем, не вынимая пальца из кольца пахового канала, толстой иглой, прокалываются кожа, подкожная клетчатка и апоневроз наружной косой мышцы живота над концом указательного пальца. Когда кончик иглы пройдет через ткань апоневроза, начинают вводить 0,5% раствор новокаина.
У женщин таким же раствором новокаина инфильтрируют ткани, прилегающие к надкостнице лобковой кости и большой половой губе, где прикрепляется круглая связка матки.
Словарь терминов и персоналий (глоссарий)
Абластика – принципы оперирования, предусматривающие предупреждение диссеминации опухолевых клеток с целью профилактики рецидива и метастазирования злокачественной опухоли. Основной принцип – удаление опухоли единым блоком с путями лимфооттока в пределах здоровых тканей.
Абсцесс – полость, заполненная гноем и отграниченная от окружающих тканей и органов пиогенной мембраной. Острый абсцесс быстро развивается, сопровождается резко выраженными местными воспалительными изменениями с нарушением общего состояния больного. Хронический абсцесс протекает медленно при мало выраженных общих и местных симптомах гнойного воспаления, возникает при некоторых инфекционных болезнях (туберкулез, актиномикоз и др.) или при проникновении маловирулентных возбудителей гнойной инфекции.
Абсцесс Броди.
B.C.Brodie (1783–1862), английский хирург.
Броди абсцесс – хронический остеомиелит, вызванный маловирулентными штаммами стафилококков и протекающий с образованием небольшой, хорошо отграниченной гнойной полости в губчатом веществе длинной трубчатой кости (наиболее часто – в эпифизе большеберцовой кости).
Абсцессотомия – хирургическая операция вскрытия абсцесса.
Аденокарцинома – злокачественная опухоль, происходящая и построенная из железистого эпителия.
Аденома – доброкачественная опухоль, возникающая из железистого эпителия и сохраняющая структурное сходство с исходной тканью.
Ампутация – хирургическая операция отсечения конечности или периферической ее части с пересечением костей или удаление органа (полового члена, матки, молочной железы).
Анастомоз – 1) в анатомии: естественное соединение двух полых органов (например: сосудов, протоков); 2) в хирургии: созданное оперативным путем сообщение между полыми органами, кровеносными сосудами или полостями тела.
Антибластика – совокупность мероприятий, направленных на уничтожение опухолевых клеток в операционной ране с целью профилактики рецидива и метастазирования удаляемой злокачественной опухоли (использование электрохирургического инструмента, лекарственных средств и т.п.).
Антисептика – комплекс лечебно-профилактических мероприятий, направленных на уничтожение микробов в ране, другом патологическом образовании или в организме в целом.
Анус (anus) – задний проход. Anus praeternaturalis (син.: задний проход противоестественный) – искусственно созданный путем хирургической операции наружный свищ толстой кишки, через который ее содержимое выделяется полностью.
Апоневроз Denonvilliers (Денонвиллье апоневроз, fasciae peritoneoperinealis, lamina Tyrrelly, брюшно-промежностная фасция) – фасциальная перегородка в малом тазу, расположенная фронтально между прямой кишкой сзади и половыми органами имочевым пузырем спереди (у мужчин – fasciae rectovesicalis, у женщин – fasciae rectovaginalis).
Асептика – система мероприятий, направленная на предупреждение внедрения возбудителей инфекции в рану, ткани, орнаы, полости тела больного при хирургических операциях, перевязках, эндоскопии и других лечебных и диагностических процедурах.
Болезнь Крона.
Синонимы: болезнь гранулематозная, Morbus Crohn, morbus Dalzeil, ileitis regionalis, ileitis terminals, enteritis regionalis, ileitis ulcerosa stenosans chronica.
Crohn Burrill (род. в 1884 г.), американский врач.
Крона с. – хроническое сегментарное воспаление какого-либо участка пищеварительного тракта (чаще – дистального отдела подвздошной кишки); болезнь Крона с локализацией в терминальном отделе тонкой кишки начинается обычно в возрасте 15-35 лет, несколько чаще встречается у мужчин; характерна триада: боль в правой половине живота, повторные или постоянные поносы, значительное ухудшение самочувствия. Иногда во время обострении появляются симптомы, напоминающие острый аппендицит. В пораженной части стенки кишки –изъязвления с воспалительным перипроцессом, способствующим сужению просвета. Во время обострении – лейкоцитоз со сдвигом влево, тромбоцитоз; обычны также гипохромная анемия, увеличение СОЭ, снижение активности протромбина, уменьшение концентрации калия и кальция в крови; стеаторея. Болезнь может осложниться местным нагноением, фистулами с прободением, стенозом.
Болезнь Пертеса
Perthes G.C. (1869–1927), немецкий хирург.
Синонимы: Легга-Кальве-Пертеса болезнь, остеохондрит головки бедра, псевдококсалгия.
Пертеса болезнь – наследственный асептический некроз головки бедренной кости, чаще односторонний, возникающий преимущественно у мальчиков в возрасте 6-10 лет; приводит к деформации головки и шейки бедренной кости и развитию коксартроза.
Шейерманна-мау болезнь
Scheuermann H.W. (1877–1960), датский хирург-ортопед.
Mau K. (1890–1958), немецкий хирург-ортопед.
Синонимы: кифоз остеохондропатический, кифоз подростковый, кифоз юношеский, кифоз учеников-подмастерьев, Шморля болезнь)
Шейерманна-Мау болезнь – осрохондропатия опофизов грудных, преимущественно 7-10 позвонков; проявляется стойким кифозом этого отдела позвоночника и компенсаторным лордозом шейного и поясничного отдела.
Болезнь Burger.
Синонимы: мигрирующий тромбофлебит, болезнь Винивартера (Winiwarter)-Бюргера, болезнь Бильрота(Billroth)-Винивартера-Бюргера, облитерирующий тромбангиит.
Buerger Leo (1879–1943), американский терапевт;
Winiwarter Felix von (1848–1917), австрийский хирург.
Бюргера болезнь – мигрирующий сегментарный тромбофлебит подкожных вен нижних (реже верхних) конечностей сопровождается субфебрилитетом. Синхронно или метахронно появляются признаки нарушения артериального кровообращения: повышенная чувствительность нижних конечностей к холоду, парестезии, гиперестезии, перемежающая хромота, боль, некроз, гангрена пальцев. Течение заболевания прогрессирующее, рецидивирующее. Болеют чаще молодые мужчины.
Болезнь Gregoir.
Синонимы: острый подвздошно-бедренный венозный тромбоз.
Грегуара болезнь – острая боль в конечности, быстро развивающийся отек и цианоз – основные признаки заболевания. Может вторично присоединиться нарушение артериального кровообращения с развитием так называемой венозной гангрены (из-за сдавления артерий отеком). В пораженной конечности депонируется большое количество жидкой части крови, что может привести к гиповолемии и шоку. По окончании острого периода возникает постфлебитический синдром.
Болезнь Raynaud.
Morbus Raynaud, gangraena Raynaud, gangraena symmetrica.
Raynaud Maurice (1834–1881), французский невропатолог.
Рейно (Рено) б. – приступообразно возникающие парестезии конечностей, жжение и боль. Приступ длится от нескольких минут до нескольких часов. Различают 3 стадии:
I – стадия «белого пальца» – острая ишемия;
II – «синего пальца» – присоединяется атония капилляров и стаз в них крови;
III – стадия гангрены – появляются пузыри с кровянистым содержимым, на месте которых развивается некротическая язва, мумификация одного или нескольких пальцев. Определяют спазм сосудов глазного дна. Этиология не известна. Заболевание начинается между 18 и 30 годами, болеют преимущественно женщины (5:1). Провоцирующими факторами являются холод, травма, психические переживания, курение.
Врачебная ответственность – юридическая ответственность врача за правонарушения в профессиональной или профессионально-правовой деятельности.
Врачебная ошибка – ошибка врача при исполнении своих профессиональных обязанностей, которая явилась следствием добросовестного заблюждения, не могла быть им предусмотрена и предотвращена, т.е. не являлась следствием халатного отношения врача к своим обязанностям, его невежества или злоумышленного действия. Врачебная ошибка не влечет за собой дисциплинарного, административного или уголовного наказания.
Врачебная тайна – совокупность сведений о болезни, а также об интимной исемейной жизни больного, ставших известными медицинским работникам при выполнении ими своих профессиональных обязанностей и не подлежащих разглашению. Врачебная тайна охраняется законом, сведения о болезни сообщаются лишь государственным органам здравоохранения, если этого потребуют интересы охраны здоровья населения, а следственным и судебным органам – по их требованию.
Врачебное преступление – профессинальное или профессионально-должностное деяние (действие или бездействие) врача, рассматриваемое уголовным законодательством как преступление.
Время свертывания крови – показатель активности свертывающей системы крови, равный времени от момента контакта крови с чужеродной поверхностью in vitro до формирования сгустка.
Гангрена – вид некроза, при котором омертвевшие ткани либо мумифицируются (сухая гангрена), либо подвергаются гнилостному распаду (влажная гангрена). При сухой гангрене слабо выражена интоксикация и имеется склонность к отграничению. Влажная гангрена характеризуется общей интоксикацией и малой склонностью к отграничению.
Гастростомия – хирургическая операция создания наружного свища желудка с целью искусственного кормления больного при непроходимости пищевода или для его функционального выключения.
Гастротомия – хирургическая операция вскрытия полости желудка.
Гемангиома – доброкачественная опухоль, развивающаяся из кровяносных сосудов.
Гематомезис – рвота, при которой рвотные массы представлены кровью.
Гематокрит (син.: гематокритное число) – отношение объема форменных элементов крови к объему плазмы. Гематокрит дает представление об общем объеме эритроцитов, характеризует степень гемоконцентрации или гидремии.
Гной (pus) – мутный экссудат желтовато-желтоватого цвета, состоящий из богатой белком жидкости, распадающихся лейкоцитов, погибших клеток воспаленной ткани и (обычно) патогенных микроорганизмов.
Грыжа Cooper.
Купера гр. – бедренная грыжа с двухкамерным грыжевым мешком, который состоит из 2 частей: подкожной на уровне подкожной фасции и подфасциальной, проходящей через решетчатую фасцию.
Грыжа (hernia) – выпячивание органа или его части через отверстия в анатомических образованиях под кожу, в межмышечные пространства или во внутренние карманы и полости.
Грыжа Hesselbach.
Hesselbch F.K. (1759–1816), немецкий анатом и хирург.
Гессельбаха гр. – бедренная грыжа мышечной лакуны выходит под паховую связку, опускаясь во влагалище подвздошно-поясничной мышцы. Над ней находится портняжная мышца, натягивающая широкую фасцию бедра, впереди шейки грыжевого мешка лежит артерия, огибающая подвздошную кость. Особенностью этой грыжи является ее плоская форма.
Грыжа Littré.
Littré A. (1658–1725), французский хирург.
Литтре грыжа – грыжа (чаще паховая или бедренная), содержащая в грыжевом мешке дивертикул Меккеля. Он может находиться в грыжевом мешке в свободном состоянии, может быть сращен с ним или ущемлен в грыжевом кольце.
Грыжа Maydl.
Синонимы: W-образная грыжа, грыжа с двойной петлей.
Майдля гр. – ретроградное ущемление брыжейки, кишки, находящейся в брюшной полости, а не в грыжевом мешке, с развитием гангрены внутрибрюшной петли.
Грыжа Richter.
Richter A.G. (1742–1812), немецкий хирург.
Рихтера гр. – пристеночное ущемление кишечной петли (без брыжейки): в грыжевом мешке ущемляется только часть окружности кишечной стенки, чаще противоположная линии прикрепления брыжейки; может проявляется явлениями частичной кишечной непроходимости.
Грыжа Treitz.
Синоним: околодвенадцатиперстная грыжа, парадуоденальная грыжа, мезентерикопариетальная грыжа.
Трейтца гр. – внутренняя (ложная) грыжа, связанная с ущемлением кишки в трейтцевом канале. В анамнезе у таких больных упорный запор. Различают грыжу левостороннюю (чаще) и правостороннюю. Грыжевое содержимое включает несколько петель или всю тонкую кишку. Клинически проявляется картиной высокой кишечной непроходимости. Грыжу чаще обнаруживают на операции или секции. На высоте приступа в животе обнаруживают шаровидное, подвижное, с четкими контурами образование. При ощупывании самое болезненное место соответствует грыжевым воротам. Они могут располагаться на линии, начинающейся слева над пупком и направляющейся вправо вниз к подвздошной ямке. Ущемление прекращается в положении больного на правом боку, в положении стоя боль усиливается.
Демпинг-синдром (англ.: dumping-syndrome)
Syndromus postgastrectomiae, jejunum-syndromus, hypersecretio nutritiva, albatross-syndrome (англ.).
To dump (англ.) – выбросить.
Демпинг-синдром – комплекс желудочно-кишечных и циркуляторных расстройств после еды, главным образом у больных с резецированным желудком, особенно при высокой резекции и после гастроэктомии: в течение 15 мин после еды чувство давления и полноты в эпигастральной области, тошнота, рвота жидкостью с примесью желчи, урчание в животе; потливость, приливы жара, усталость, недомогание, дрожание конечностей, сердцебиение, головная боль; больные вынуждены часто посещать врача («они кружатся около врача подобно раненому альбатросу»). Упомянутые явления объясняются перерастяжением пищевыми массами культи желудка и двенадцатиперстной кишки и наличием большого количества гиперосмолярных масс в двенадцатиперстной кишке, которые способствуют быстрому переходу жидкости из плазмы, что обуславливает развитие гиповолемии вплоть до коллапса.
Дивертикул – выпячивание стенки полого органа (кишки, пищевода, мочеточника и др.), сообщающееся с его полостью.
Дивертикул истинный – дивертикул, образованный за счет всех слоев стенки органа.
Дивертикул ложный – дивертикул, образованный за счет выпячивания только слизистой оболочки и подслизистого слоя через дефект мышечного слоя стенки органа.
Дивертикул подвздошной кишки (меккелев дивертикул) – непостоянно встречающийся дивертикул нижней трети подвздошной кишки, являющийся остатком не полностью редуцированного желточного стебля (канал в желточном стебельке выстлан энтодермальным эпителием и соединяет полость средней кишки зародыша с желточной полостью).
Дивульсия – насильственное расширение суженного просвета естественного канала или полости с применением какого-либо дилататора.
Диссектор – хирургический инструмент в виде зажима, предназначенный для тупого разделения тканей при их препаровке и выделении трубчатых органов, а также для временного пережатия кровеносных сосудов, протоков и захвата лигатур при хирургических вмешательствах.
Диссеминация – распространение возбудителя инфекционной болезни из первичного очага или опухолевых клеток из основного узла по кровеносным и лимфатическим путям в пределах одного органа или всего организма.
Дистония – патологическое изменение тонуса.
Дисфагия – общее название расстройств глотания.
Дормиа петля – инструмент для извлечения конкрементов из мочеточника, представляющий собой корзиночку из нескольких проволочных петель, втянутую в трубку мочеточникового катетера; при выводе из трубки петли корзиночки расправляются, конкремент входит в просвет между ними, подтягивается к торцу катетера и извлекается.
Дренаж (син.: дренажная система) – устройство или приспособление, предназначенное для выведения жидкостей из ран, естественных и патологоческих полостей тела.
Дренаж Бюлау
Bülau G. (1958–1900), немецкий врач.
Бюлау дренаж – способ удаление жидкости и воздуха из плевральной полости с помощью трубчатого дренажа, вводимого путем прокола грудной стенки троакаром и действующего по принципу сообщающихся сосудов с односторонне работающим клапаном (чаще – из пальца хирургических перчаток).
Дренаж Керра
Kehr Hans (1862–1916), немецкий хирург.
Керра дренаж – Y-образный трубчатый дренаж, состоящий из трех колен, расположенных в виде буквы «Y»; применяется при операциях на желчных путях (два коротких верхних колена вводят в просвет желчного протока, а длинное нижнее выводят в операционную рану).
Дренирование – лечебный метод, заключающийся в создании возможности постоянного оттока жидкости из полых органов, полостей тела, ран и абсцессов.
Дуглас-абсцесс – отграниченное скопление гноя в прямокишечно-пузырном углублении у мужчин или в прямокишечно-маточном углублении у женщин.
Жане шприц – шприц для промываний, отличающийся значительной емкостью (100-200мл); на конце штока и на кольце, охватывающем стеклянный цилиндр, имеются припаянные кольца для удобства работы.
Желтуха механическая (обтурационная) – желтуха, обусловленная механическим препятствием оттоку желчи по желчевыводящим путям; характеризуется повышенным содержанием в крови прямого билирубина, холестерина, желчных кислот, уменьшением выделения стеркобилина с калом.
Живот острый – клиническое понятие, объединяющее ряд острых заболеваний органов брюшной полости, подлежащих срочному хирургическому вмешательству; термин может употребляться только в рамках предварительного диагноза при направлении в стационар.
Заднепроходная область – задняя часть области промежности, расположенная между копчиком и линией, соединяющие седалищные бугры.
Заднепроходные столбы – продольные складки слизистой оболочки заднепроходного канала.
Заживление вторичным натяжением – заживление раны путем постепенного заполнения раневой полости, содержащей гной, грануляционной тканью с последующей эпителизацией и образованием рубца; характерно для инфицированных или зияющих ран.
Заживление первичным натяжением – заживление раны путем соединения ее стенок свертком фибрина с образованием на поверхности струпа, под которым происходит быстрое замещение фибрина грануляционной тканью, эпителизация и образование узкого линейного рубца.
Зажим Микулича
Mikulicz-Radeski J.F. (1850–1905), немецкий хирург.
Микулича зажим – инструмент для прикрепления операционного белья к брюшине, представляющий собой зажим с кремальерой, имеющий на изогнутых по плоскости рабочих губках поперечные насечки и зубцы на концах.
Зажим Пайра
Payr E. (1871–1946), немецкий хирург.
Пайра зажим – хирургический раздавливающий зажим, применяемый при резекции желудка; имеет четырехшарнирный запирающий замок, а на концах рабочих губок прорезь и фиксирующий штифт, предохраняющий их от перекоса.
Зажим Пеана
Pean J.E. (1830–1898), французский хирург.
Пеана зажим – кровоостанавливающий зажим с кремальерой и плоскоовальными губками с насечкой.
Зажим Billroth
Billroth Th. (1829–1894), венский хирург.
Бильрота зажим – хирургический зажим с кремальерой и длинными узкими равномерными рабочими губками, имеющий по плоскости рабочих губок поперечные насечки без зубцов на концах.
Зажим Kocher
Kocher E.Th. (1841–1917), швейцарский хирург.
Кохера зажим – кровоостанавливающий зажим с длинными узкими рабочими губками, имеющими острые зубцы, причем единственный зубец одной губки входит между двумя зубцами второй губки.
Зоб – патологически увеличенная щитовидная железа.
Зоб диффузный – зоб, характеризующийся равномерным увеличением железы.
Зоб диффузно-узловой – зоб, характеризующийся равномерным увеличением железы с одновременным наличием в ней одного или более узлов.
Зоб узловой – зоб, при котором ткань щитовидной железы имеет вид узлов.
Зоб эутиреоидный – зоб, не сопровождающийся нарушениями функции щитовидной железы.
Зоб диффузный токсический – болезнь, характеризующаяся диффузным увеличением щитовидной железы и повышением её функции; проявляется нарушением обмена веществ, часто экзофтальмом, похуданием, тахикардией.
Зоб спорадический – болезнь, характеризующаяся возникновением зоба, как правило, без выраженных нарушений функции железы, развивающаяся у лиц, проживающих вне эндемичных по зобу районов.
Зоб эндемический – болезнь, характеризующаяся возникновением зоба, поражающая население определенных географических районов с недостаточностью йода в окружающей среде.
Зоб фиброзный (Риделя струма, Риделя тиреоидит, зоб каменный, тиреоидит фиброзный) – хронический тиреоидит, характеризующийся первичным разрастанием волокнистой соединительной ткани с вторичной гибелью фолликулярного эпителия щитовидной железы; фиброз может распространяться на окружающие ткани, имитируя злокачественную опухоль.
Зоб лимфоматозный (Хасимото зоб, зоб лимфоцитарный, тиреоидит лимфоматозный) – тиреоидит аутоиммунной природы, клинически проявляющийся зобом и симптомами гипотиреоза.
Зонд - инструмент в виде тонкого стержня, предназначенный для проведения диагностических или лечебных процедур в различных полостях и каналах тела человека.
Зоб желобоватый – односторонний металлический зонд V-образной формы в поперечном сечении, служащий проводником режущего инструмента и защищающий от повреждения им глубжележащей ткани.
Зоб пуговчатый – зонд в виде стержня, заканчивающегося утолщениями сферической формы; обычно изготовляется из мягких металлов (сплавов), что позволяет легко придавать пуговчатому зонду нужные изгибы.
Идиопатический – возникающий без видимых причин, характеризующийся неясным происхождением.
Изотонический раствор – раствор, осмотическое давление которого равно осмотическому давлению плазмы крови (например: 0,9% водный раствор хлорида натрия, 4,5-5% водный раствор глюкозы).
Иммобилизация – создание полной неподвижности или уменьшенной подвижности одной или нескольких частей тела при повреждениях и некоторых заболеваниях.
Иммунодиагностика – диагностика заболеваний или нарушений защитных функций организма с использованием методов, основанных на специфическом взаимодействии антигена с антителом.
Инфекция хирургическая – общее название болезней и патологических процессов инфекционного происхождения, при которых хирургические мероприятия имеют решающее лечебное значение (флегмоны, костно-суставной туберкулез и др.) или играют существенную профилактическую роль (столбняк, раневая инфекция).
Инфильтрат – участок ткани, характеризующийся скоплением обычно не свойственных ему клеточных элементов, увеличенным объемом и повышенной плотностью; иногда термин «инфильтрат» используется для обозначения участка ткани, инфильтрированного каким-либо веществом (напр., раствором анестезирующего средства).
Ирригоскопия – рентгенологическое исследование толстой кишки при ретроградном заполнении ее контрастной взвесью.
Ихорозный – гнилостный, характеризующийся разложением тканей с образованием дурно пахнущих газов.
Карбункул – острое гнойно-некртическое воспаление нескольких расположенных рядом сальных желез и волосяных фолликулов, распространяющееся на окружающую кожу и подкожную клетчатку.
Киста – патологическая полость в органе, стенка которой образована фиброзной тканью (ложная киста) или выстлана эпителием или эндотелием (истинная киста).
Киста эхинококковая – ложная киста, представляющая собой пузырную личиночную стадию эхинококкоза. Стенка кисты образована фиброзной тканью, выстланной гомогенными массами хитина.
Клизма – введение жидкости в толстую кишку через задний проход с лечебной или диагшностической целью.
Клизма гипертоническая – послабляющая клизма с введением небольшого объема гипертонического раствора в прямую кишку через задний проход.
Клизма очистительная – лечебная клизма с введением большого объема воды, иногда с добавлением глицерина, растительного масла или мыльного раствора, производимая для разжижения и удаления содержимого толстой кишки.
Клизма сифонная – клизма, при которой через зонд, введенный через задний проход на 20-25 см (предположительно в сигмовидную кишку), вводят большой объем жидкости и немедленно выводят через тот же зонд, повторяя процедуру со сменой воды 10-15 раз; применяется с целью полного опорожнения толстой кишки, а также для лечения динамической непроходимости кишечника. В проведении сифонной клизмы принимает участие врач. Количество выводимой жидкости должно быть сопоставимо с вводимым объемом воды. Задержка жидкости в толстой кишке опасна развитием осложнений.
Колика – приступ резких схваткообразных болей, чаще при заболеваниях органов брюшной полости.
Ксено- – составная часть сложных слов, означающая «чужой», «чужеродный», «необычный».
Культя – часть конечности или органа, оставшаяся после ампутации (в т.ч. после травматической или врожденной).
Лапаро- - составная часть сложных слов, означающая «относящийся к брюшной полости или к животу».
Лапароцентез – эвакуация из брюшной полости скопившейся в ней жидкости путем прокола брюшной стенки (пункцией брюшной полости).
Лимфатический узел Cloquet
Синоним: лимфатический узел Пирогова – Розенмюллера.
Клоке узел – лимфатический узел, расположенный в овальной ямке бедра. При увеличении симулирует невправимую бедренную грыжу.
Линия Damoiseau.
Синоним: симптом Эллиса – Дамуазо.
Дамуазо линия – линия начинается у позвоночного столба, затем поднимается дугообразно кверху, достигая наивысшей точки по лопаточной или на уровне задней подкрыльцовой линии, с последующим постепенным опусканием книзу. Наиболее низким уровнем ее расположения является грудинная линия. Определяют при выпотах в плевральную полость.
Малигнизация – приобретение клетками нормальной или патологически измененной ткани (например: доброкачественной опухоли) свойств клеток злокачественной опухоли.
Мацерация – размягчение и разрыхление тканей вследствие длительного воздействия на них жидкости.
Меккелев дивертикул.
J.F.Meckel junior (1781–1833), немецкий анатом.
Меккелев дивертикул – дивертикул подвздошной кишки.
Метастаз – очаг опухолевого или воспалительного процесса, развившийся в результате переноса патологического материала (клеток, микроорганизмов и т.п.) из другого очага этого процесса в том же организме.
Метастазы Krukenberg.
Krukenberg H. (1863–1935), немецкий хирург.
Крукенберга метастазы – в пупок и яичники при раке желудка у женщин.
Метастазы Schnitzler.
Шнитцлера метастазы – в область пузырно-прямокишечной клетчатки при IV стадии опухолей пищевого канала. Определяют при ректальном исследовании.
Метастазы Virchow.
Virchow Rudolf (1821–1902), немецкий патолог.
Вирхова метастазы – возможный признак рака желудка: наличие одного или нескольких плотных безболезненных лимфатических узлов над левой ключицей вблизи прикрепления грудино-ключично-сосцевидной мышцы. Иногда прикрыт ключицей.
Метастатический узел Sorgius.
Синоним: железа Соргиуса, узел Соргиуса,
Соргиуса с. – при раке молочной железы у наружного края большой грудной мышцы прощупывают лимфатический узел величиной от горошины до лесного ореха.
Метастатический узел Troisier.
Труазье с. – признак рака молочной железы: лимфатический узел, который расположен в медиальном отделе надключичного треугольника у места слияния внутренней яремной и подключичной вен. Поражение узла Труазье указывает на предшествующие ему метастазы в парастернальных или медиастинальных лимфатических узлах, то есть на значительное распространение рака молочных желез.
Метеоризм – вздутие живота вследствие скопления газов в кишечнике.
Некротомия – рассечение некротизированных тканей; прменяется для облегчения доступа кислорода к ним при анаэробной инфекции или для ускорения высушивания тканей при влажной гангрене.
Некрэктомия – иссечение омертвевших тканей, не затрагивающее жизнеспособные ткани.
Нобля операция – хирургическая операция: фиксация петель тонкой кишки друг к другу в порядке, соответствующем их нормальному расположению в брюшной полости; предложена для профилактики непроходимости кишечника при спаечной болезни.
Ножницы Cooper.
Cooper A.P. (1768–1841), английский хирург и анатом.
Купера ножницы – хирургические ножницы, у которых концы рабочих ветвей закруглены и изогнуты по плоскости.
Ножницы Richter
Richter A.G. (1742–1812), немецкий хирург.
Ножницы Рихтера (синоним: ножницы, изогнутые по ребру) – хирургические ножницы с рабочими концами, изогнутые под углом 25-300 к оси симметрии инструмента.
Операция – лечебное или диагностическое мероприятие, связанное с травмированием тканей и органов больного.
Операция паллиативная – операция, производимая при невозможности излечения и имеющая целью облегчение страданий больного или улучшение функции пораженного органа.
Операция плановая – операция, выполнение которой может быть заранее назначено на определенный день или отсрочено без существенного ущерба для здоровья больного.
Операция пробная – операйия, при которой после осуществления оперативного доступа устанавливается нецелесообразность и (или) невозможность выполнения оперативного приема.
Операция радикальная – операция, посредством которой может быть достигнуто полное излечение больного.
Операция срочная – операция, которая должна быть произведена в короткий срок от начала заболевания (в пределах нескольких суток – до 72 часов).
Операция экстренная – операция, производимая немедленно после осмотра больного при состоянии, угрожающем в данный момент его жизни.
Опухоль – патологическое разрастание тканей, состоящих из качественно изменившихся клеток, ставших атипичными в отношении дифференцировки, характера роста и передающих эти свойства при последующем делении.
Опухоль ворсинчатая – аденома толстой кишки, характеризующаяся экзофитным ростом с образованием сосочков; отличается высокой склонностью к малигнизации.
Опухоль доброкачественная – опухоль, обладающая преимущественно экспансивным ростом, отодвигающая и раздвигающая (или сжимающая) окружающие ткани, не разрушая их, и не дающая, как правило, метастазов.
Опухоль злокачественная – опухоль, обладающая инфильтративным ростом, прорастающая в окружающие ткани, разрушающая их, способная к метастазированию.
Остеомиелит гематогенный острый – остеомиелит, возникающий в результате проникновения возбудителей гнойной инфекции в кость по кровеносному руслу, с развитием очага гнойного воспаления чаще в метафизе длинной трубчатой кости.
Остеомиелит гематогенный хронический – остеомиелит, развивающийся как исход острого гематогенного остеомиелита после прорыва гноя через мягкие ткани и ограничения процесса в кости; проявляется наличием секвестров и гнойных свищей.
Остеомиелит первично-хронический – общее название форм остеомиелита, характеризующихся постепенным развитием и вялым течением с преобладанием гиперпластических и склеротических процессов.
Панариций – острое гнойное воспаление тканей пальца.
Пандактилит – гнойное воспаление всех тканей пальца кисти.
Паронихия – воспаление околоногтевых тканей.
Патогенез – 1) учение об общих закономерностях развития течения и исхода болезней; 2) механизм развития конкретной болезни, патологического процесса или состояния.
Паховая область – парная область переднебоковой стенки живота, ограниченная сверху межостной линией, медиально – вертикальной линией, проводимой по латеральному краю прямой мышцы живота, латерально и снизу – паховой складкой.
Паховая складка – бороздка кожи, расположенная на границе паховой области и передней поверхности бедра, отчасти соответствует паховой связке.
Паховое кольцо глубокое – внутреннее отверстие пахового канала, расположенное на его задней стенке соответственно латеральной паховой ямке; образовано поперечной фасцией в месте ее перехода на семенной канатик.
Паховое кольцо поверхностное – наружное отверстие пахового канала, расположенное медиальнее и выше лобкового бугорка, образованное медиально и латерально ножками апоневроза наркжной косой мышцы живота, латерально и сверху – его межножковыми волокнами, медиально и снизу – загнутой связкой.
Паховый канал – щель между мышцами передней брюшной стенки, расположенная над внутренней половиной паховой связки; у мужчин содержит семенной канатик, у женщин – круглую связку матки.
Паховый промежуток – естественный дефект мышечного слоя брюшной стенки в межмедиальной части паховой области. Ограниченный сверху нижним краем внутренней косой мышцы живота, а иногда и поперечной мышцей живота, снизу и латерально – медиальной частью паховой связки, медиально – латеральным краем влагалища прямой мышцы живота.
Перитонизм – совокупность слабо выраженных признаков раздражения брюшины, не связанного с ее инфицированием (например: при кровоизлиянии в брюшинную полость).
Перитонит – воспаление брюшины.
Перфорация – возникновение сквозного дефекта в стенке полового органа.
Пинцет – инструмент с двумя пластинчатыми пружинящими браншами, предназначенный для захватывания и удерживания тканей, а также различных материалов и предметов, когда прикосновение к ним пальцами не желательно или невозможно.
Пинцет анатомический – пинцет, бранши которого имеют на рабочей стороне неглубокие поперечные насечки.
Пинцет хирургический – пинцет, у которого для прочного удержания захваченной ткани одна бранша имеет на конце два зубца, а вторая – один зубец, совмещающийся при смыкании пинцета с впадиной между зубцами первой бранши.
Пиогенный – вызывающий нагноение, обусловленный нагноением.
Пирогова-Пароны пространство
Н.И. Пирогов (1810–1881), отечественный хирург.
F. Parona, итальянский хирург, 19 век.
Пирогова-Пароны пространство – клетчаточное пространство в нижней трети передней области предплечья, ограниченная спереди длинным сгибателем большого пальца и глубоким сгибателем пальцев, а сзади – квадратным пронатором и межкостной перепонкой.
Пневмоторокс – наличие воздуха или газа в плевральной полости; возникает в результате травмы, патологического процесса или создается искусственно с лечебной целью.
Полип – патологическое образование, выступающее над поверхностью органа и связанное с ним ножкой или своим основанием.
Проба Борисова.
Борисов А. В. (1862–?), русский хирург.
Борисова п. — дифференциально-диагностический признак почечной колики и острого живота: после орошения поясничной области хлорэтилом боль уменьшается или исчезает в случае почечной колики.
Проба Оппеля.
Оппеля п. – признак недостаточности периферического артериального кровообращения: больной в положении лежа на спине поднимает нижние конечности, разогнутые в коленных суставах до угла 45°, и удерживает их в таком положении 1 мин. При недостаточности периферического артериального кровообращения в области подошвы на стороне поражения наступает побледнение, которое в норме отсутствует. Чем раньше возникает побледнение (следят по секундомеру) и чем сильнее оно выражено, тем сильнее нарушено кровообращение.
Проба Lowwel – Loubry.
Лувель – Лобри п. – признак тромбофлебита (флеботромбоза): в положении больного стоя, его просят натужно покашлять. При наличии свежего тромбофлебита или флеботромбоза на месте тромбированной вены голени или бедра появляется четко локализованная боль.
Проба Opitz – Ramines.
Opitz Hans (родился в 1888 г.), немецкий педиатр.
Опитца-Раминеса п. – симптом положителен при тромбофлебите глубоких вен голени: больному в положении лежа на спине накладывают выше колена манжетку сфигмоманометра и накачивают в нее воздух до уровня 52 гПа (40 мм рт. ст.). При этом происходит повышение венозного давления в дистальном отделе конечности. При наличии флебита боль усиливается в подколенной области или в икроножных мышцах.
Пролежень – некроз мягких тканей (кожи с подкожной клетчаткой, слизистой оболочки, стенки полого органа или кровеносного сосуда и др.), возникающий вследствие ишемии, вызванной продолжительным непрерывным механическим давлением на них.
Псевдополип – утолщение слизистой оболочки кишки около язвы или рубца, внешне напоминающее полип.
Пункция перикарда по Ларрею.
Larrey D.J. (1766–1842), французский хирург.
Ларрея прокол перикарда – пункция перикарда в углу между VII реберным хрящем и основанием мечевидного отростка; применяется при экссудативных перикардитах.
Разрез – рассечение кожи или слизистой оболочки и подлежащих мягких тканей для доступа к определенной анатомической области в ходе хирургической операции или для вскрытия очага воспалительного процесса.
Разрез Мак-Бернея-Волковича-Дьяконова.
Ch.McBurnea (1845–1914), американский хирург.
Волкович Н.М. (1858–1928), советский хирург.
Дьяконов П.И. (1855–1908), отечественный хирург.
Мак-Бернея-Волковича-Дьяконова разрез – косой разрез в правой подвздошной области между наружной и средней третью линии, проводимой от правой верхней передней ости к пупку, с раздвиганием волокон внутренней косой и поперечных мышц; наиболее распространенный операционный доступ при аппендэктомии.
Разрез Kocher.
Kocher E.Th. (1841–1917), швейцарский хирург.
Кохера разрез – операционный доступ к печени и желчному пузырю в виде разреза передней брюшной стенки от мечевидного отростка до X правого ребра.
Рак – злокачественная опухоль, развивающаяся из эпителиальной ткани.
Рана – нарушение целостности кожи или слизистых оболочек на всю их толщину (часто и глубжележащих тканей и органов), вызванное механическим воздействием.
Раневая полость – пространство, ограниченное стенками и дном раны; размеры и форма Р.п. определяются характером раны и степенью ее зияния.
Раневой канал – раневая полость, глубина которой значительно превосходит ее поперечные размеры.
Раневой процесс – совокупность клинических, патофизиологических, биохимических, бактериологических и морфологических изменений, характеризующих динамику заживления раны.
Ранение – механическое воздействие на ткани и органы, влекущее нарушение их целости с образованием раны; нанесение операционной раны термином Р. не обозначают.
Ранорасширитель – инструмент, предназначенный для расширения краев раны; снабжен устройством для фиксации его рабочих частей (напр., зеркал, крючков) в разведенном положении.
Распатор – хирургический инструмент, предназначенный для отделения надкостницы от кости.
Рассечение – разделение тканей с помощью какого-либо острого инструмента.
Ректоскопия – метод исследования прямой кишки путем осмотра поверхности ее слизистой оболочки с помощью ректального зеркала или ректоскопа.
Рестеноз – повторное сужение просвета какого-либо органа после его расширения оперативным путем.
Связка Жимбернатова (лакунарная связка) – часть сухожильных волокон, отделяющихся от паховой связки. Связка идет внутрь и кнаружи к гребню лобконой кости, ограничивает с медиальной стороны сосудистую лакуну.
Симптом Бартомье-Михельсона.
Михельсон Абрам Иосифович (1902–1971), советский хирург и уролог.
Бартомье-Михельсона с. – признак острого аппендицита: болезненность при пальпации правой подвздошной области, усиливающаяся в положении больного лежа на левом боку.
Симптом Берштейна.
Синоним: «генитальный симптом».
Берштейн П. Л. (1878 – 1923), российский хирург.
Берштейна с. – возможный признак перфоративной язвы желудка или двенадцатиперстной кишки: подтягивание яичек к наружным отверстиям паховых каналов, половой член поворачивается головкой кверху, параллельно передней брюшной стенке, в результате рефлекторного сокращения поверхностной фасции живота и мышцы, поднимающей яичко.
Симптом Боткина.
Синоним: холецисто-коронарный синдром.
Боткина с. – кардиалгия, наблюдаемая при холецистите. Проявляется колющей, схваткообразной болью в области сердца, левой лопатки и левого плеча, иррадиирующей из верхней половины живота. Часто предшествует желчной колике или сопровождает ее. Могут быть изменения на ЭКГ.
Симптом Волковича – Kocher.
Волкович Николай Маркианович (1858–1928), российский хирург.
Волковича – Кохера с. – признак острого аппендицита: боль, первоначально возникающая в подложечной области (иногда непосредственно под мечевидным отростком), спустя несколько часов локализуется в правой подвздошной области.
Симптом Воскресенского (симптом «рубашки»).
Воскресенский Владимир Михайлович (1902–1951), российский хирург.
Воскресенского с. – признак острого аппендицита: при быстром проведении ладонью по передней брюшной стенке (поверх рубашки) от правого реберного края вниз больной испытывает боль.
Симптом Воскресенского.
Воскресенский Владимир Михайлович (1902–1951), российский хирург.
Воскресенского с. – возможный признак острого панкреатита: исчезновение пульсации брюшной аорты в подчревной области.
Симптом Грекова.
Греков Иван Иванович (1867–1934), российский хирург.
Грекова с. – ранний признак прободения язвы желудка или двенадцатиперстной кишки: замедление пульса сразу же после прободения.
Симптом Дзбановского-Чугуева.
Дзбановского – Чугуева с. – определяют визуально в первые часы после перфорации язвы желудка или двенадцатиперстной кишки: поперечные втянутые бороздки на передней брюшной стенке, соответствующие перемычкам прямых мышц живота.
Симптом Михельсона.
Михельсон Абрам Иосифович (1902–1971), советский хирург и уролог.
Михельсона с. – признак острого аппендицита у беременных: усиление боли в правой половине живота в положении больной на правом боку (вследствие давления матки на воспаленный очаг).
Симптом Образцова.
Образцов Василий Парменович (1849–1920), русский терапевт.
Образцова с. – признак холецистита: боль при глубокой пальпации при вдохе.
Симптом Образцова.
Образцов Василий Парменович (1849–1920), русский терапевт.
Образцова с. – признак хронического аппендицита: усиление боли во время пальпации в илеоцекальной области, при этом правая нога приподнята.
Симптом Обуховской больницы, симптом Hochenegg.
Обуховская больница – старейшая больница в Санкт-Петербурге, основана в 1779 году.
Обуховской больницы с. – признак заворота сигмовидной кишки: расширенная и пустая ампула прямой кишки при ректальном исследовании.
Симптом Пастернацкого.
Пастернацкий Федор Игнатьевич (1845–1902), русский терапевт.
Пастернацкого с. – почечной патологии: при нанесении коротких ударов боковой поверхностью кисти по поясничной области ниже XII ребра возникает боль с последующим кратковременным появлением или усилением эритроцитурии. Симптом положителен при нарушении оттока мочи из почки, при воспалительных процессах почки и околопочечной клетчатки, при поражениях позвоночного столба и воспалении ретроперитонеально расположенного червеобразного отростка.
Симптом Промптова.
Промптова с. – свидетельствует о гинекологическом заболевании: болезненность матки при отодвигании ее кверху пальцами, введенными во влагалище или прямую кишку. Используют для дифференциальной диагностики с острым аппендицитом, при котором этот симптом, как правило, отрицательный.
Симптом Раздольского.
Раздольский Иван Яковлевич, советский невропатолог.
Раздольского с. – возможный признак острого аппендицита: при перкуссии брюшной стенки молоточком или пальцем выявляется болезненность в правой подвздошной области.
Симптом Раздольского
Раздольский Иван Яковлевич, советский невропатолог.
Раздольского с. – при остром панкреатите: боль при перкуссии над поджелудочной железой.
Симптом Розанова, симптом “ваньки-встаньки”.
Розанов Владимир Николаевич (1872–1934), российский хирург.
Розанова с. – признак внутрибрюшного кровотечения при разрыве селезенки: больной лежит на левом боку с поджатыми к животу бедрами; при попытке повернуть больного на спину или другой бок он тотчас же переворачивается и занимает прежнее положение.
Симптом Ситковского - Ортнера.
Ситковский Петр Порфирьевич (1882–1933), российский хирург.
Ситковского - Ортнера с. – признак острого аппендицита: при положении больного на левом боку в илеоцекальной области появляется боль.
Симптом Склярова
Склярова с. – признак непроходимости толстой кишки: в растянутой и раздутой сигмовидной кишке определяется шум плеска.
Cимптом Спасокукоцкого.
Спасокукоцкий Сергей Иванович (1870–1943), российский хирург.
Спасокукоцкого с. – возможный признак кишечной непроходимости: аускультативно определяется звук падающей капли.
Симптом Спижарного.
Спижарный Иван Константинович (1857–1924), российский хирург.
Спижарного с. – признак прободения при гастродуоденальных язвах: исчезновение печеночной тупости и появление высокого тимпанита над печенью.
Симптом Чугаева, “струны аппендицита”.
Чугаев Анатолий Андреевич, русский хирург.
Чугаева с. – признак острого аппендицита: при пальпации удается, прощупать сокращенные, пучки наружной косой мышцы живота, напоминающие натянутые струны.
Симптом Штернберга.
Штернберга с. – определяют при мезадените: боль, возникающая при пальпации по ходу корня брыжейки, то есть по косой линии Штернберга, идущей из правой боковой области в левую подреберную. Служит для дифференциальной диагностики между хроническим аппендицитом и мезаденитом.
Симптом Яуре – Розанова.
Яуре Г. Г., российский хирург;
Розанов Владимир Николаевич (1872–1934), российский хирург.
Яуре с. – признак ретроцекального аппендицита: болезненность в правой поясничной области, в области треугольника Пти.
Симптом Allen.
Аллена с. – кратковременная боль в груди, одышка, тахикардия. Наблюдают при эмболии мелких ветвей легочной артерии.
Симптом Bartomier.
Бартомье с. – признак хронического аппендицита: усиление или появление боли при пальпации правой подвздошной области в положении больного лежа на левом боку.
Симптом Bartomier – Михельсона.
Михельсон Абрам Иосифович (1902–1971), советский хирург и уролог.
Бартомье – Михельсона с. – признак острого аппендицита: болезненность при пальпации правой подвздошной области, усиливающаяся в положении больного лежа на левом боку.
Симптом Ваеуеr.
Байера с. – ассиметрия вздутия живота. Наблюдают при завороте сигмовидной кишки.
Симптом Bergmann.
Бергманна с – признак желудочно-кишечного кровотечения при язвенной болезни: исчезновение боли вслед за начавшимся кровотечением.
Симптом Blumberg, симптом Блюмберга–Щеткина.
Blumberg Moritz (1873–1955), немецкий хирург.
Блюмберга с. – признак воспаления или раздражения брюшины: при медленном надавливании рукой на живот больной почти не испытывает боли; острая боль появляется при быстром отнятии руки.
Симптом Clark
Clark A. (1807–1887), американский врач.
Кларка с. – исчезновение печеночной тупости при перфорации желудка или двенадцатиперстной кишки.
Симптом Co-Tui.
Co-Tui F.W. (род. в 1896 г.), американский хирург.
Ко Туи с. – смещение желобка на передней брюшной стенке, соответствующего белой линии, и пупка в сторону локализации острого патологического процесса в брюшной полости.
Симптом Cullen.
Cullen Thomas Stephen (1868–1953), американский хирург.
Куллена с. – наблюдается у больного острым панкреатитом: желтовато цианотичная окраска в области пупка
Симптом Courvoisier.
Courvoisier Louis (1843—1918), швейцарский хирург.
Курвуазье с. – возможный признак нарушения проходимости общего желчного протока: сильно увеличенный желчный пузырь у больных с механической желтухой.
Симптом Dalrimple.
Дальримпля с. – признак базедовой болезни: широкая глазная щель, лагофтальм.
Симптом De Quervaine.
Де Кервена с. – признак перфорации желудка или двенадцатиперстной кишки: появление тупого перкуторного звука в нижних и боковых отделах живота, чаще справа в связи с затеканием желудочного содержимого и перитонеальной экссудации.
Симптом De Quervaine.
Синоним: симптом «указательного пальца».
F. de Quervain (1868–1940), швейцарский хирург.
Де Кервена с. – при рентгенологическом исследовании вследствие тонического сокращения стенки желудка образуется складка слизистой оболочки в виде указательного пальца, направленного в сторону «ниши» на малой кривизне желудка.
Симптом Dieulafoy.
Dieulafoy Georges (1839–1911), французский врач.
Дьелафуа с. – характерно для перфоративных гастродуоденальных язв: острая «кинжальная» боль в животе.
Симптом Eleker – Brunner, френикус-симптом.
Элекера – Бруннера с. – признак перфорации желудка или двенадцатиперстной кишки: боли иррадиируют вверх в область надплечья, ключицы, лопатки в связи с раздражением нервных окончаний диафрагмального нерва.
Симптом Frostberg.
Frostberg Nils, шведский рентгенолог.
Фростберга с. – определяемая рентгенологически (релаксационная дуоденография) деформация вогнутого контура нисходящего отдела двенадцатиперстной кишки в виде перевернутой цифры три. Образуется в результате втяжения папиллярной и парапапиллярной части двенадцатиперстной кишки в головку поджелудочной железы при хроническом панкреатите, раке головки поджелудочной железы.
Симптом Graefe.
Грефе с. – признак базедовой болезни: отставание верхнего века при взгляде вниз.
Симптом Gobiet.
Гобье с. – выявляемые рентгенологически у больных острым панкреатитом: рефлекторный парез и вздутие толстой кишки, особенно поперечной ободочной кишки. Чаши Клойбера отсутствуют.
Симптом Grey – Turner.
Грея - Турнера с. – наблюдается при остром панкреатите цианоз кожи живота.
Симптом Grunwald.
Грюнвальда с. – возможный признак острого панкреатита: экхимозы или петехии вокруг пупка, в ягодичных областях вследствие поражения периферических сосудов.
Симптом Halsted.
Halsted William Stewart (1852–1922), американский хирург.
Холстеда с. – признак острого панкреатита: слабосинюшный или мрамороподобный цвет кожи живота и периферических частей тела (токсическое поражение капилляров).
Симптом Haudek.
Симптом “ниши”.
Haudek Martin (1880–1931), австрийский рентгенолог.
Хаудека с. – рентгенологический признак язвы желудка: дефект ткани, заполненный введенным в желудок контрастным веществом, напоминает нишу.
Симптом Hohmann.
Hohmann Georg (1880–1970), немецкий ортопед.
Хомана с. – признак тромбофлебита голени: появление болей в икроножной мышце при тыльном сгибании стопы. Больной лежит на спине, ноги полусогнуты в суставах колен. Производят тыльное сгибание стопы в голеностопном суставе. Боль в икроножных мышцах, которую при этом ощущает больной, свидетельствует о тромбозе глубоких вен. Боль возникает при сдавливании тромбированных вен икроножными мышцами.
Симптом Joffroy.
Joffroy A. (1844–1908), французский врач.
Жоффруа с. – отсутствие морщин при попытке наморщить лоб, наблюдающееся у больных диффузным токсическим зобом.
Симптом Kehr.
Kehr Hans (1862–1916), немецкий хирург.
Кера с. – признак холецистита: боль при вдохе во время пальпации правого подреберья. (Точка Керра – точка, расположенная на пересечении наружного края правой прямой мышцы живота и реберной дуги. Соответствует проекции желчного пузыря. Болезненная при его заболеваниях.)
Симптом Kiwull.
Кивуля с. – признак непроходимости толстой кишки (при завороте сигмовидной и слепой кишок): в растянутой и раздутой сигмовидной кишке определяется металлическая звучность.
Симптом Kloiber.
Kloiber H., немецкий рентгенолог.
Клойбера с. – рентгенологический признак кишечной непроходимости: при обзорной рентгеноскопии брюшной полости обнаруживаются горизонтальные уровни жидкости и газовые пузыри над ними.
Симптом Kocher
Kocher E.Th. (1841–1917), швейцарский хирург.
Кохера с. – боль в области эпигастрия в первые часы заболевания острым аппендицитом.
Симптом Körte.
Körte Werner (1853–1937), немецкий хирург.
Кёрте с. – признак острого панкреатита: наличие болезненности и резистентности брюшной стенки, соответствующих области проекции поджелудочной железы (зона высотой 6-7 см, заключенная между двумя горизонатальными линиями, одна из которых соответствует уровню пупка, другая – на 6-7 см выше пупка).
Симптом Kulenkampff.
Kulenkampff С., немецкий врач.
Куленкампфа с. – признак внутрибрюшного кровотечения: перкуссия по мягкой или почти мягкой брюшной стенке вызывает сильную болезненность.
Симптом Kulenkampff.
Kulenkampff С., немецкий врач.
Куленкампфа с. – признак прободения при гастродуоденальных язвах: при пальцевом ректальном исследовании определяется болезненность дугласова пространства, вызванная скоплением перитонеального экссудата и желудочного содержимого.
Симптом Lennander.
Леннандера с. – наблюдают при остром деструктивном аппендиците: разность температуры более 1°С в подкрыльцовой ямке и прямой кишке.
Симптом Mayo - Robson.
Mayo-Robson Arthur (William) (1853–1933), английский хирург.
Мейо-Робсона с. – признак острого панкреатита: боль при пальпации в левом реберно-позвоночном углу.
Синдром McGinn – White.
McGinn Sylvester, американский врач;
White Paul Dudley (1886–1973), американский кардиолог.
Мак-Гинна – Уайта с. – ЭКГ-симптомокомплекс у больных с эмболией легочной артерии: глубокие S1 и QIII, резко отрицательные ТIII.
Симптом McFadden.
Мак-Фаддена с. – возможный признак мезаденита: болезненность у наружного края правой прямой мышцы живота (2–4 см ниже пупка).
Симптом Michaelis.
Михаэлиса с. – указывает на возможность эмболии легочных сосудов: повышение температуры тела у больных тромбофлебитом.
Симптом Moebius.
Moebius Paul Julius (1853–1907), немецкий невропатолог.
Мебиуса с. – признак тиреотоксикоза: при фиксации взгляда на близком предмете (конвергенция) глаза не могут долго находиться в положении конвергенции и один из них вскоре отходит кнаружи.
Симптом Mondor.
Mondor Henri (1885–1962), французский хирург.
Мондора с. – признак острого панкреатита: наличие фиолетовых пятен на коже лица и туловища.
Симптом Mosess.
Мозеса с. – признак трмбофлебита глубоких вен: голень сдавливают (умеренно!) руками в передне-заднем направлении, а затем с боков. Появление боли при сдавлении спереди - назад указывает на тромбофлебит глубоких вен голени.
Симптом Murphy.
Murphy John Benjamin (1857–1916), американский хирург.
Мерфи с. – признак патологии желчного пузыря: равномерно надавливая большим пальцем руки на область желчного пузыря, предлагают больному сделать глубокий вдох; при этом у него “захватывает” дыхание и отмечается значительная боль в этой области.
Симптом Mussy-Георгиевского.
Мюсси – Георгиевского с. – признак поражения желчного пузыря (часто – острого холецистита): болезненность при пальпации между ножками грудино-ключично-сосцевидной мышцы.
Синдром Ogilvie (Pseudoobstructio coli).
Ogilvie Heneage (1887–1971), английский хирург
Огилви с. – картина ложной закупорки толстого кишечника в результате расстройств симпатической иннервации: увеличенный живот, расширенная толстая кишка, исхудание, запоры. Патологические изменения в толстом кишечнике не обнаруживаются; обычно наблюдается при злокачественных опухолях различной другой локализации, дающих метастазы в симпатические ганглии.
Симптом Ortner.
Ortner Norbert, австрийский терапевт.
Ортнера с. – признак заболевания печени и желчевыводящих путей: поколачивание краем ладони по правой реберной дуге вызывает боль.
Симптом Rosenbach.
Rosenbach Ottomar (1851–1907), немецкий терапевт.
Розенбаха с. – возможный признак гипертиреоза: мелкое и быстрое дрожание опущенных век.
Симптом Rovsing.
Rovsing Niels Thorkild (1862–1927), датский хирург.
Ровзинга с. – признак аппендицита или тифлита: при пальпации левой подвздошной области и одновременном надавливании на нисходящий отдел ободочной кишки давление через газы передается на илеоцекальную область, что сопровождается болью.
Симптом Stellwag.
Stellwag Carion Karl (1823–1904), австрийский офтальмолог.
Штельвага с. – признак тиреотоксикоза и паркинсонизма: редкое и неполное мигание.
Симптом Trendelenburg.
Trendelenburg Friedrich (1844–1924), немецкий хирург.
Тренделенбурга с. – наблюдают при перитоните: резко напряженная передняя брюшная стенка с подтянутыми к паховым отверстиям яичками (вследствие сокращения m. cremaster).
Симптом Trendelenburg.
Trendelenburg Friedrich (1844–1924), немецкий хирург.
Тренделенбурга с. – признак разрыва селезенки: малый пульс, бледность кожи и слизистых оболочек, рефлекторное напряжение брюшных мышц, подтянутая кверху мошонка и выпрямленный половой член указывают на внутрибрюшное кровотечение.
Симптом Watil.
Watil Eduard (1833–1890), немецкий хирург.
Валя с. – признак непроходимости кишечника: локальный метеоризм или выпячивание отдела кишечника выше уровня препятствия (видимая ассиметрия живота, прощупываемая кишечная выпуклость, видимая глазом перистальтика, слышимый при перкуссии тимпанит).
Симптом Westermark.
Westermark Nils (род. 1892), шведский рентгенолог.
Вестермарка с. – рентгенологический признак эмболии легочной артерии: повышение прозрачности легочной ткани в зоне разветвления тромбированной артериальной ветви, выбухание конуса и дуги легочной артерии, увеличение размеров правого желудочка. Определяют рентгенологически при тромбоэмболии легочной артерии.
Симптом Wood.
Вуда с. – электрокардиографический комплекс у больных с эмболией легочной артерии: отрицательный зубец Т в отведении V1, V2, V3, который нормализуется в течение 3—6 нед. выраженные S и Q.
Синдром Савицкого.
Синоним; синдром малых признаков Савицкого.
Савицкого с. – наблюдают у больных раком желудка: слабость, утомляемость, снижение трудоспособности, понижение аппетита, отвращение к мясу, рыбе.
Синдром Brock.
Синоним: ложное ущемление Брока.
Брока с. – ряд острых заболеваний брюшной полости при наличии грыж брюшной стенки сопровождается симптомами, которые симулируют ущемление грыжи. В грыжевом мешке, имеющем сообщение со свободной брюшной полостью, происходят вторичные изменения, связанные с поступлением в полость грыжевого мешка экссудата из брюшной полости (при прободении язвы желудка или тонкой кишки холецистите). Ранее вправимая грыжа становится невправимой.
Синдром Courvoisier-Terrier.
Courvoisier Louis (1843–1918), швейцарский хирург;
Terrier Louis-Felix (1837–1908), французский хирург.
Курвуазье – Террье с. – симптомокомплекс опухоли фатерова соска: увеличенный желчный пузырь, желтуха, ахолический кал.
Синдром Пейтца-Егерса
Peutz J.L.A. (родился в 1886 г.), голландский врач.
Jeghers H., голландский врач.
Пейтца-Егерса с. – наследственный полипоз желудочно-кишечного тракта (полипоз пигментно-пятнистый), сочетающийся с коричневой мелкоточечной пигментацией слизистой оболочки губ и полости рта, а также кожи в окружности рта и тыльных поверхностей мелких суставов кистей.
Синдром Dieulafoy.
Ulcus simplex Dieulafoy, exulceratio simplex Dieulafoy, erosio Dieulafoy.
Dieulafoy Georges (1839–1911), французский врач.
Дьелафуа с. – массивное желудочное кровотечение, вызванное повреждением (аррозией) подслизистой артериальной ветви: преимущественно болеют лица молодого возраста без так называемого желудочного анамнеза. Массивная кровавая рвота наступает внезапно; диагноз подтверждается либо фиброгастроскопией, либо во время операции; быстро прогрессирующая острая постгеморрагическая анемия. Без срочного хирургического вмешательства — летальный исход в течение нескольких дней.
Синдром Gardner.
Gardner E.J. (род. в 1909 г.), американский врач, генетик.
Гарднера с. – наследственная болезнь, характеризующаяся полипозом толстой кишки в сочетании с доброкачественными опухолями, чаще костей и кожи (остеомы, фибромы, липомы), наследуется по аутосомно-доминантному типу.
Синдром Leriche.
Bifurcatio-syndromus, thrombosis aortae terminalis.
Leriche Rene (1879–1955), французский хирург
Лериша с. – симптомокомплекс у больных с облитерацией аорты и в области бифуркации: половое бессилие и чувство усталости в нижних конечностях, атрофия мускулатуры ног; холодные конечности, кожа на них имеет бледность слоновой кости, синюшные пятна на стопах. Часто (в поздних стадиях) расстройства трофики нижних конечностей; слабая или исчезающая пульсация в ногах и на поверхности стоп. Болеют преимущественно мужчины после 40 лет.
Синдром Маllогу – Weiss.
Lacerationes gastrooesophagales haemorrhagicae.
Mallory G. Kenneth (род. в 1900 г.), американский патолог;
Weiss Soma (1898–1942), американский врач.
Маллори-Вейсса с. – проявления разрывов слизистой оболочки в переходной зоне между пищеводом и желудком: повторная рвота, позже рвота становится кровавой. Рентгенологически – без патологии; при гастроскопии – разрывы слизистой оболочки длиной 2-4 см, расположенные продольно по отношению к оси пищевода и желудка и локализующиеся преимущественно на границе между пищеводом и кардией. Чаще наблюдаются у лиц, злоупотребляющих алкоголем.
Синдром Mirizzi, morbus Mirizzi, stenosis ductus hepatici.
Mirizzi Pablo Luis (род. 1893), аргентинский хирург.
Мирицци с. – обозначение клинической картины закупорки общего желчного протока различной этиологии (спазм, воспаление, опухоль, камни): неопределенная боль в правом подреберье и эпигастрии, тошнота, желтуха, гипербилирубинемия; часто прощупывается увеличенный болезненный желчный пузырь; нередко — картина острого живота.
Синдром Raynaud.
Raynaud Maurice (1834–1881), французский невропатолог.
Рейно (Рено) с. – в отличие от болезни синдром Рейно является всегда вторичным. Сопутствует склеродермии, красной волчанке, атеросклерозу, облитерирующему тромбангииту, коллагенозам. Наблюдают при опухолях спинного мозга, сирингомиелии, травме головного мозга. Характеризуется явлениями вазомоторного невроза, изменением цвета кожи: мертвенно-бледная окраска сменяется синюшной или розовой, особенно под влиянием эмоций, напряжения, холода. Ангиоспастические явления длительное время преобладают над трофопаралитическими. Характерна асимметрия поражения (появление на одной верхней конечности, одной половине лица и др.). В основе синдрома – спазм сосудов. Язвенно-гангренозные процессы развиваются редко.
Синдром Sahli.
Синоним: венозная корона Сали.
Sahli Hermann (1856–1933), швейцарский врач.
Сали с. – наблюдают при сдавлении верхней полой вены: расширение подкожных вен верхней половины туловища, местами образующих сплетения.
Синдром Trousseau.
Trousseau Armand (1801–1867), французский терапевт.
Труссо с. – тромбофлебит у больных с висцеральной карциномой: острый спонтанный тромбофлебит (обычно в одной из больших вен), нередко мигрирующего характера; антикоагулянты в обычных дозах не дают эффекта. Симптомы тромбофлебита обычно исчезают только после оперативного удаления опухоли.
Синдром Winiwarter – Buerger.
Синдром Buerger, morbus (Leo) Buerger, morbus Billroth – Winiwarter thrombangiitis obliterans.
Winiwarter Felix von (1848–1917), австрийский хирург;
Buerger Leo (1879–1943), американский терапевт.
Винивартера – Бергера с. – клиническая картина пресенильного облитерирующего тромбангиита: болезнь начинается в среднем возрасте; для течения характерна смена рецидивов и ремиссий; расстройства периферического кровообращения — холодные ноги, боль в икроножных мышцах и стопах (даже в состоянии покоя); тыльная артерия стопы, подколенная и задняя большеберцовая артерии не прощупываются. Наблюдается перемежающаяся хромота, позднее — гангрена больших пальцев ног. Изменения глазного дна, гемианопсия. В случаях повреждения мозговых сосудов — головная боль, мигрень, головокружения, иногда потеря сознания, расстройства чувствительности, афазия; в иных случаях присоединяются психические расстройства.
Синдром Zollinger-Ellison.
Zollinger Robert Milton (род. 1903), американский врач;
Ellison Edwin Homer (род. 1918), американский врач.
Золлингера – Эллисона с. – опухоль поджелудочной железы из бета-клеток островкового аппарата с рецидивирующей пептической язвой желудочно-кишечного тракта: рецидивирующая боль в животе, понос, симптомы язвы, рецидивирующее желудочно-кишечное кровотечения, иногда перфорация язвы. Желудочный сок — массивная гиперсекреция и гиперхлоргидрия. Прогноз зависит от характера опухоли и является весьма серьезным.
Смерть – необратимое прекращение жизнедеятельности организма, являющееся неизбежной заключительной стадией его индивидуального существования.
Смерть клиническая – терминальное состояние, наступающее после прекращения сердечной деятельности и дыхания и продолжающееся до наступления необратимых изменений в высших отделах центральной нервной системы.
Стома – созданный оперативным путем наружный свищ полого органа.
Торакоцентез – эвакуация из плевральной полости скопившейся в ней жидкости путем прокола грудной стенки (пункцией плевральной полости).
Транссудат – бедная белками жидкость, скапливающаяся в тканевых щелях и полостях тела при отеках.
Треугольник Garland.
Garland G.M. (1848–1926), американский врач.
Гарланда с. – определяется при плевральных экссудатах: расположен кнутри от линии Дамуазо, между ней и позвоночным столбом. Катетами служат позвоночный столб и линия, проведенная от него к вершине линии Дамуазо, а гипотенузой – сама линия Дамуазо.
Треугольник Grocco.
Grocco Pietro (1856–1916), итальянский терапевт.
Раухфуса – Грокко треугольник – треугольник, длинный катет которого образован позвоночным столбом, а второй катет имеет горизонтальное положение и соответствует нижней границе легкого здоровой половины грудной клетки; гипотенузу образует продолжение линии Дамуазо на противоположную сторону. Притупление перкуторного звука на здоровой стороне — в области треугольника Раухфуса — Грокко определяют, когда на противоположной половине грудной клетки, в плевральной полости жидкость достигает уровня VII—VIII ребер. Притупление вызвано смещением средостения в здоровую сторону, плевральным выпотом и частично тем, что позвоночный столб проводит перкуторные колебания по направлению к экссудату, что обусловливает присоединение к легочному звуку тупого звука выпота.
Троакар – хирургический инструмент, представляющий собой стальной осроконечный стилет с надетой на него трубкой, предназначенной для прокола грудной или брюшной стенки с целью выведения стенки из полостей тела человека.
Флегмона – острое, четко неотграниченное гнойное воспаление клетчатки.
Эвентрация – выпадение внутренних органов брюшной полости через дефект ее стенки.
Экссудат – богатая белком жидкость, содержащяя форменные элементы крови, выходящая из мелких вен и капилляров в окружающие ткани и полости тела при воспалении.
Экстирпация – хирургическая операция с полным удалением органа.
Эмпиема – значительное скопление гноя в какой-либо полости тела или в полом органе.
Эрозия – поверхностный дефект слизистой оболочки или эпидермиса.
Язва – дефект кожи или слизистой оболочки и подлежащих тканей, процессы заживления которого (развитие грануляций, эпителизация) нарушены или существенно замедлены.
Язва каллезная – хроническая язва желудка, кишки или пищевода с плотными краями и дном вследствии интенсивного развития рубцовой ткани.
Язва малигнизированная – язва, в краях которой появились комплексы атепичных клеток, склонные к пролиферации.
Язва пенитрирующая – язва желудка, кишки или пищевода, характеризующаяся разрушением всех слоев стенки пораженного органа и повреждением соседнего органа с образованием полости (канала), не сообщающейся с полостями тела (брюшной, плевральной).
Язва перфоративная – язва слизистой оболочки какого-либо органа, характеризующаяся разрушением его стенки на всю толщу с образованием канала, сообщающего полость или просвет пораженного органа с соседней полостью.
Русско-латинский словарь необходимых медицинских терминов
А
ампутация amputatio,onis f
анальгин Analginum,i, n
аппендицит appendicitis,tidis f
аппетит appetitus,us m; appetitio,onis f
аптека officina, ae f
артериальный arteriacus, a, um; arterialis, e
артерия arteria, ae f
асептический asepticus a,um
асептически aseptice
атропина сульфат Atropini sulfas, sulfatis
Б
бедренная кость femur,oris n
бешенство rabies, el f
биопсия biopsia,ae f
болезнь morbus,i f
болеть doleo,ui, -, ere
болеющий dolens,ntis;laborans,ntis
боль dolor,oris m
больница clinica, ae f
большеберцовая кость tibia,ae f
большой magnus, a, um
бугорок tuberculum, i n
бугристость tuberositas,atis f
быстро cito
быть sum,fui, -, esse
В
в асептических условиях aseptice
в таблетках in tabulettis
вазелин Vasellnum, i n
величина magnitudo,inis f
вена vena, ae f
венечный coronarius, a, um
венозный venosus, a, um
вертел trochanter, eris m
верхний superior, superius
ветвь ramus, i m
вещество substantia, ae f
вид, способ modus, i m
видеть video,vidi, visum, ere
витамин Vitaminum, i n
вкус gustus, us m
внешний вид habitus, us m
внимательно diligenter
внутренний internus, a, um
внутривенный intravenosus, a, um
внутримышечный intramuscularis, e
вода aqua, ae f
восходящий ascendens,ntis
впрыскивание, инъекция iniectio,onis f
врач medicus, i m
вредить noceo,nocui,nocitum, ere
выздоровление sanatio,onis f
выздоравливать convalesco,lui, ere; sanitatem recipere
выздоравливающий reconvalescens, ntis
выслушивать ausculto, avi, atum, are
высокий altue, a, um
Г
гиперемия,переполнение кровью hyperaemia, ae f
гипертония hypertonia, ae f
гипотония hypotonia, ae f
гистология histologia, ae f
глаз oculus,i m
глазная впадина orbita,ae f
глицерин Glycerinum, i n
глубокий profundus, a,um
глюкоза Glycosa, ae f
гной pus, puris f
гнойное воспаление кожи pyodermia, ae f
голень crus, cruris n
головокружение kephalodynia,ae f; vertigo, inis f
грамм gramma, atis n
грудина sternum, i n
грудная клетка thorax,acis m
грудной thoracalis, e; pectoralis, e
грудь pectus,oris n
губчатый spongiosus, a, um
густой spissus, a, um
Д
двенадцатиперстная кишка duodenum, i n
действие effectus,us m
диагноз diagnosis, is f
диаметр diameter, tri f
диафрагма diaphragma,atis n
дистиллированный destillatus,a, um
длина longitudo,inis f
длинный longus, a, um
для pro(предл. с твор. пад.), ad (предл. с вин. пад.)
для внутреннего употребления pro usu interno
для внешнего употребления pro usu externo
для наркоза pro narcosi
добавочный accessorius,a, um
доброкачественный benignus, a, um
доза dosis,is f
доля lobus, i m
дорсальный dorsalis, e
дуга arcus,us m
дурной запах oze, es f
дыхание respiratio, onis f
Ж
железа glandula, ae f
железо Ferrum, i n
желудок, желудочек ventriculus, i m
жёлчный felleus,a,um
жёлчь fel,fellis n
женский femininus, a, um
живой animatus, a, um
живот abdomen,inis n
жидкая мазь linimentum,i n
жидкий fluidus,a,um; liquefactus, a, um
жидкость liquor, oris m
жизнь vita, ae f
жировой, ожирелый adiposus, a, um
жить vivo, vixi, victum, ere
З
заболевание aegritudo,inis f
закупоренный clausus,a,um
запах odor, oris m
заражать inficio,feci,fectum, ere
заразный infectiosus,a,um; contagiosus,a,um
зашивать praesuo,sui,sutum, ere
защищать defendo,ndi,nsum, ere
здоровье sanitas,atis f; valetudo,inis f
зелень бриллиантовая Virile nitens, Viridis nitentis
зелёный viridis e
злокачественный malignus, a, um
знание scientia,ae f
зоб struma, ae f
зрительный opticus, a, um
зуб dens, dentis m
зубчатый serratus, a, um; dentatus, a, um
И
известный notus,а,um
излечение sanatio,onis f
измерение тонуса tonometria, ae f
изъязвление ulceratio,onis f
инородный alienus, a,um
искусственный artificialis, e
истинный verus,a, um
история болезни anamnesis,is f
источник fons, fontis m
исхудание macies,ei f
Й
йод iodum,i n
К
капилярный capillaris, e
капсула capsula,ae f
касторовое масло oleum Ricini
кислота аскорбиновая Acidum ascorbinicum, i n
кислота ацетилсалициловая Aciduma acetylsalicylicum, i n
кислота салициловая Acidum salicylicum, i n
кишечная колика enteralgia,ae f
клетка cellula, ae f
клизма clysma, atis n
клиновидный cuneiformis, e;
кожа cutis, is f
кожный cutaneus, a, um
кожный зуд pruritus cutaneus,pruritus cutanei
консервативный conservativus, a, um
консилиум consilium, ii n
концентрированный concentratus, a,um
копчик coccyx, ygis m
копчиковый coccygeus, a, um
короткий brevis, e
косой obliquus, a, um
костный osseus,a,um
кость os,ossis n
красный ruber, bra, brum
крестцово-копчиковый sacrococcygeus, a, um
крестцовый sacralis, e
кривой curvus, a, um
кристаллический crystallisatus, a, um
критический criticus, a, um
кровохарканье haemoptoe, es f
Л
латеральный lateralis, e
левый sinister, tra, trum
лёгкое pulmo,onis m
лекарство medicamentum,i n; pharmacon, i n
лейкоцит leucocytus,i m
лечение curatio, onis f
лечить curo, avi, atum, arc; sano, avi, atum,are
лимфатический lymphaticus, a, um
линия linea, ae f
липкий adhaesivus, a, um
ложный spurius, ar,um
локтевая кость ulna, ae f
лопатка scapula,ae f
луковица bulbus,i m
лучевая кость radius, ii m
М
магнезия сульфат Magnesii sulfas,sulfatis
магний Magnium,ii n;Magnesium, ii n
мазь unguentum,i n
мазь жидкая linimentum, i n
максимальный maximus, a, um
малоберцовая кость fibula, ae f
малоберцовый fibularis, e; peroneus, a, um
малый parvus, a, um
марля tela,ae
масло oleum, i n
масло вазелиновое oleum Vaselini,olei Vaselini
масло касторовое oleum Ricini, olei Ricini
масляный oleosus, a, um
медиальный medialis,e
медицина medicina,ae f
медицинский medicatus, a, um
межкостный interosseus, a, um
мелкий subtilis, e
мельчайший subtilissimus, a, um
мельчайшим образом subtilissime
место locus, i m
метод methodus, i f
мешок saccus, i m
миллиграмм milligramma, atis n
минеральный mineral is, e
минимальный minimus, a, um
множественное воспаление суставов polyarthritis,tidis f
моча urina, ae f
мочевой urinarius, a, um
мужской masculinus, a, um
мускул, мышца musculus, i m
мягкий mollis, e
Н
наркоз narcosis, is f
наружный externus, a, um
натрия гидрокарбонат Natrii hydrocarbonas,atis
натрия тиосульфат Natrii thiosulfas, atis
натрия хлорид Natrii chloridum, i
неизвестный ignotus, a,um
некротический necroticus,a, um
необходимый necessarius, a,um
непарный impar, imparis
нерв nervus, i m
нервный nervosus, a, um
нижний inferior, ius
нисходящий ascendens, ntis
нитевидный filiformis, e
нитроглицерин Nitroglycerinum,i n
нога pes, pedis m
нож culter,cultri m
ножка crus, cruris n
нормальный normalis, e
О
обморожение congelatio,onis f
обморок syncope, es f
ободочная кишка colon,i n
оболочка tunica, ae f
общая слабость asthenia, ae f
обыкновенный ordinarius,a, um
обыкновенный,общий communis, e
оксациллин Oxacillinum, i n
опасность periculum, i n
операция operatio, onis f
опухоль tumor, oris m
опытный peritus,a, um
орган organum, i n (organon, i n)
организм organismus, i m
острый acer, acris, acre
ость spina, ae f
отверстие foramen, inis n
П
палец digitus, i m
панкреатический pancreaticus, a, um
пенициллин Pencillinum, i n
пепсин pepsinum, i n
передний anterior, anterius
перекись водорода Hydrogenii peroxydum, peroxydi
перелом fractura, ae f
перемежающийся intermittens, ntis
перемена mutatio, onis f
печень hepar,hepatis n
пиридоксина гидрохлорид Pyridoxini hydrochloridum, i
пластырь emplastrum, i n
плеврит pleuritis,tidis f
плечо,плечевая кость humerus, i m
плод кориандра fructus Coriandri
поверхностный superficialis, e
поверхность, лицо facies, ei f
повреждение laesio,onis f
поврежденный laesus, a, um
поджелудочная железа pancreas, atis n
поджелудочный pancreaticus, a, um
подкожный subcutaneus, a, um
подколенный popliteus,a,um
позвонок vertebra,ae f
позвоночный vertebralis,e
покой quies,etis f
покраснение rubor,oris m
полезный utilis, e
полный plenus, a, um; completus, a, um
полость cavum, i n
полый cavus,a,um
понос diarrhoea, ae f; alvus laxa
поперечный transversus, a, um; transversalis, e
по правилам искусства lege artis
поправляться reficio, feci, fectum, ere
порок сердца vitium cordis
постель lectum, i n
поставить диагноз dignosco, gnovi, gnotum, ere
постоянный perpetuus, a, um
потеря amissio, onis f
почка (анат.) ren, renis m
правый dexter, tra, trum
препарат praeparatum, i n
признак signum, i n; nota, ae f; symptoma, atis n
применение applicatio, onis f
принимать surno, sumpsi, sumptum, ere
причина causa, ae f
прогноз prognosis, is f
продолжительный diuturnus, a, um
пролежень decubitus, us m
промежуточный intermedius, a, um
прописывать (лекарство) praescribo, scripsi, scriptum, ere
простой simplex, icis
против contra (предлог с вин. пад.)
противоядие antidotum, i n
проток ductus,us m
прямая кишка rectum, i n
прямой rectus, a, um
пузырь vesica, ae f
пульс pulsus, us m
Р
разлитой diffusus, a, um
различный varius, a, um
различать distingue, nxi, nctum, ere
размещать loco, avi, alum, are
разный varius, a, um
рак cancer,cri m
рана vulnus, eris n
распознавать dignosco, novi, notum, ere
распылённый pulveratus, a, um
раствор solutio, onis f
растворенный solutus, a, um
растворимый solubilis, e
рваный laceratus, a, um; lacer, era, erum
рвота vomitus, us m
рёберный costalis, e
ребро costa, ae f
рука manus, us f
С
свеча suppositorium, ii n
свободный liber, era, erum
связка ligamentum, i n
сигмовидный sigmoideus,a,um
сила vis, - f
сильный validus, a, um; fortis, e (pulsus)
симптом symptoma, atis n
система systema, atis n
складка plica, ae f
сколько нужно quantum satis
скорый celer, eris, ere
слабость asthenia, ae f; atonia, ae f
слепой caecus, a, um
слизистый mucosus, a, um; gummosus, a, um (mixtura)
слизь mucilago,inis f
сложный compositus, a, um
смертельный letalis, e
смертоносный mortifer, fera, ferum
снотворный somnifer, fera,ferum
совет consilium, ii n
сок succus, i m
сок желудочный succus gastricus, i m
соляный hydrochloricus, a, um
сон somnium, ii n; somnus, i m
сонный caroticus, a, um
сопротивляться adversor, atus sum, ari
состояние status, us m
сосуд vas,vasis n
спайка commisura, ae f
спирт spiritus, us m
способ modus, i m
средний medianus, a, um
средство remedium, ii n
старческий senilis, e
ствол truncus, i m
стерилизованный sterilisatus, a, um
стерилизовать steriliso,avi, atum, are
стерильный sterilis, e
судорога spasmus, i m;crampus, i m
суеверие superstitio, onis f
сумка bursa, ae f
сустав articulatio, onis f
суставной articularis, e
сухой siccus, a, um
Т
тальк Talcum, i n
твёрдый durus, a, um
тело corpus,oris n
тёмный fuscus, a,um
толщина crassitudo, inis f
тонкий tenuis, e
точный certus, a, um
тошнота fastidium, ii n
трубка, труба tuba, ae f
тыльный posterior, ius
тяж taenia, ae f
тяжёлый gravis, e; molestus, a, um
У
уголь carbo, onis m
удалять evacuo, avi, atum, are
узел ganglion, ii n
урология urologia, ae
учащённый frequens, ntis
учёный doctus, a, um
Ф
фаланга phalanx, ngis f
фасция fascia, ae
фиброзный fibrosus, a, um
флеботомия phlebotomia, ae
флегмона phlegmone, es f
фосфат phosphas, atis m
функция functio,onis f
Х
хирург chirurgus, i m
хирургический chirurgicus, a, um
хрящ cartilago,inis f
Ц
целебный medicatus, a, um; saluber, bris, bre
центральный centralis, e
Ч
частый frequens, ntis (pulsus)
часть pars, rtis f
чашечка, лоханка calyx, ycis m
человек homo,inis m
человеческий humanus, a, um
через прямую кишку per rectum
через рот per os
чистый purus, a, um
чувствовать себя sentio, ivi,itum, ire(se); habeo, bui,bitum, ere (se)
Ш
шов sutura, ae f
Щ
щель fissura, ae f
щитовидный thyreoideus, a, um
Э
этиловый aethylicus, a, um
этиология aethiologia, ae f
эфирный aethereus, a, um
Я
ядовитый toxicus, a, um
ядро nucleus, i m
язык lingua, ae f